
Abstract
Results of a rapid prenatal aneuploidy screening in uncultured amniocytes using FISH are available within 24 hr. However, care has to be taken of possible pitfalls in connection with the commercially available probe sets and in the interpretation of results in general. Here we present our cut-off rates for and the way in which we handle the Aneu Vysion kit (ABBOTT/Vysis), based on the experience of 1200 studied cases. In summary, the method is reliable, and the risk for misdiagnosis is low (~0.4%). Nonetheless, the test should be used exclusively as a preamble to full chromosome analysis by microscopy.
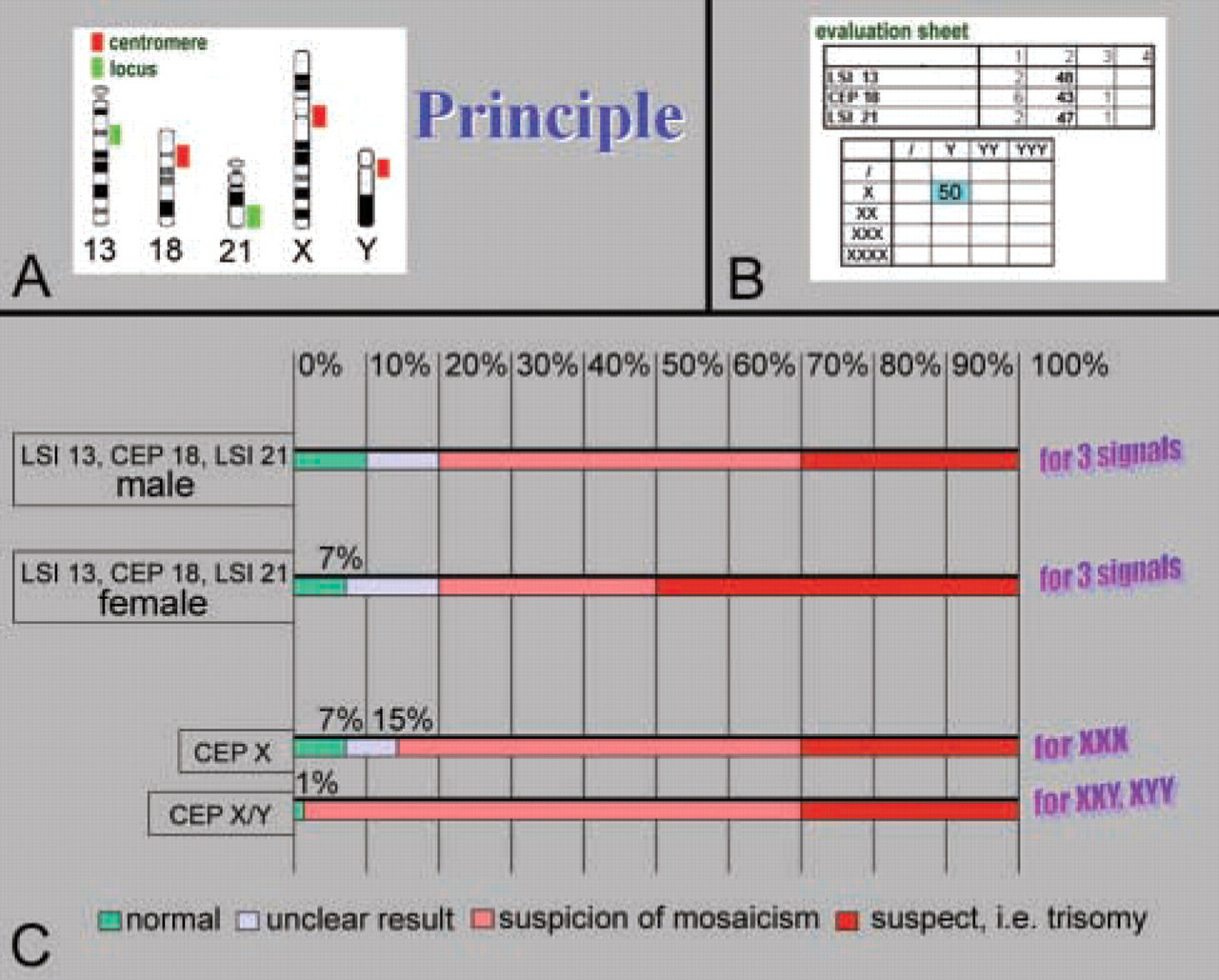
A
We exclusively apply the only FDA-approved FISH test for rapid aneuploidy screening in uncultivated amniocytic cells, the Aneu Vysion kit (commercially available at ABBOTT/Vysis; Downers Grove, IL) consisting of three α-satellite DNA probes for chromosomes X, Y, and 18 (cep X, cep Y, and cep 18) and two locus-specific probes for 13q14 (LSI 13) and 21q22.13~ 22.2 (LSI 21) (Figure 1A). The three centromeric probes and the two locus-specific probes are applied to the samples in two different hybridizations. Using this probe set, it is possible to detect chromosomal aberrations as listed in Table 1, column A. However, one should be aware that genetic disorders such as those listed in Table 1, column B are not excluded after a “normal” result of the rapid aneuploidy screening.
For rapid aneuploidy screening, it is necessary to prepare the uncultivated amniocytes as recommended in the Aneu Vysion kit protocol. In brief, 2 or 3 ml of amniocytic fluid is centrifuged (1000 rpm, 5 min) and the pellet is suspended in 3 ml trypsin/EDTA and incubated for 15 min at 37C. After centrifugation, the pellet is resuspended in 5 ml 0.075 M KCl and incubated at 37C for 20 min. After addition of 2 ml Carnoy fixative [methanol:acetic acid (3:1)], centrifugation, resuspension, and incubation at −20C for 5 min in 3 ml Carnoy fixative, the preparation is finalized with a last centrifugation. The supernatant is discarded, and the cells are diluted in 200 μl of the remaining supernatant and placed on a slide. After air drying of the slide, a standard FISH procedure follows, including an overnight hybridization step. After the posthybridization washings, the slides are mounted with an antifade plus coverslip and 50 interphase nuclei per case and probe combination are evaluated under the fluorescence microscope. This is a semistatistical evaluation, which in “normal” cases leads to results as shown, for example, for a male fetus in Figure 1B.
Genetic disorders that can (column A) and cannot (column B) be detected by rapid aneupoidy screening (FISH)

In our laboratory, we analyzed 1200 cases (between 1998 and 2004) with the FISH test for rapid aneuploidy screening followed by conventional banding cytogenetics. Initially, we performed a retrospective study (Table 2) to obtain control values to serve as an orientation for the further studies. Fifty nuclei from uncultivated amniocytic fluid derived from 20 male and 20 female cases known to have a normal karyotype according to GTG banding were analyzed by the Aneu Vysion kit probe set. The range observed in these samples for 1, 2, and 3 signals for LSI 13, LSI 21, cep 18, cep X, and cepY showed high sample-specific variability (Table 2), and the lab internal cut-off rates for one and three signals were defined as 10%. Therefore, the values for a suspected trisomy were much higher than, e.g., for our own previous studies on tumor cytogenetic samples (e.g., Gebhart et al. 1993). On the basis of the data shown in Table 2 and the experience obtained from the 1200 samples studied, we developed a cut-off scheme for trisomies, as shown in Figure 1C. As long as not more than 7–10% of the studied cells present with three specific signals, no trisomy of the corresponding chromosomal region is suspected and a normal report is issued. At between 7–10% and 20%, the evaluation is regarded an “unclear result,” which is with high probability a normal result. However, in such cases, we try to evaluate 100 or more nuclei for the probe in question to come to a final decision. A value of >20% is indicative of a trisomy, at least as a mosaic, or of a translocation trisomy t(21,21) (Liehr et al. 1999). Figure 1C shows the difference between female and male fetuses and in the interpretation of the results, owing to the fact that in amniocytic fluid of male fetuses, maternal cell contamination can be detected but that in fluid of female fetuses, such contamination is not present. Therefore, the results for female fetuses should be interpreted with more care, and the cut-off rates are lower. Similar suggestions are made for the handling of XXX, XYY, or XXY results (Figure 1C).
(
In the overwhelming majority of the 1200 cases studied, the results obtained by the rapid aneuploidy test and the banding cytogenetics were in complete concordance. However, there were five cases which led to false-positive or false-negative results due to centromeric polymorphisms or to the presence of a small supernumerary marker chromosome or a dicentric marker chromosome not detectable in the interphase (Liehr et al. 2001,2002). Therefore, the rapid aneuploidy test has a reliability of 99.6% in our hands, which is in good concordance with other studies (e.g., Eiben et al. 1999; Tepperberg et al. 2001; Weremowicz et al. 2001). As we have previously suggested, all of the observed pitfalls and the misdiagnoses of the prenatal aneuploidy screening by FISH could easily be obviated by the exclusive use of locus-specific probes (Liehr et al. 2002). The advantage of such probes, such as probes LSI 13 and LSI 21, has been proven, e.g., by the fact that the LSI 21 probe is suitable for distinguishing between free and translocation trisomy 21 in the interphase (Liehr et al. 1999).
Fifty nuclei from uncultivated amniocytic fluid derived from 20 different cases known to have a normal karyotype according to GTG banding were analyzed with the Aneu Vysion kit probe set a
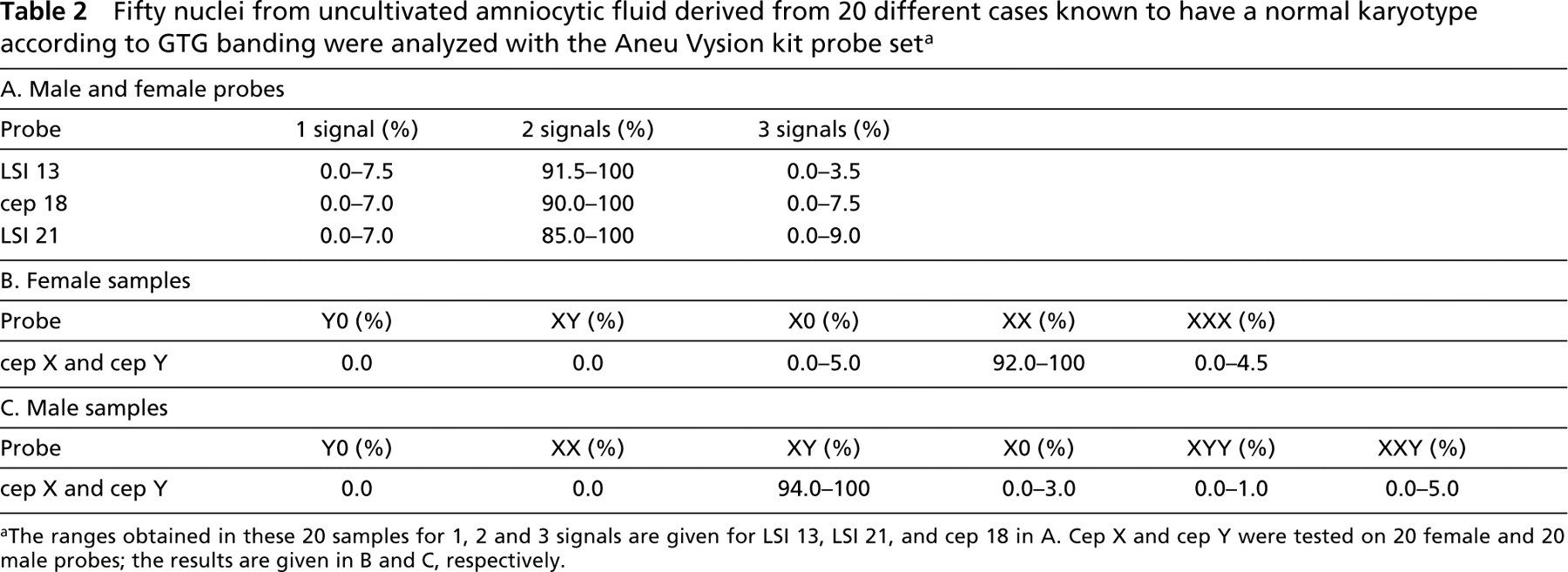
The ranges obtained in these 20 samples for 1, 2 and 3 signals are given for LSI 13, LSI 21, and cep 18 in A. Cep X and cep Y were tested on 20 female and 20 male probes; the results are given in B and C, respectively.
In summary, the rapid prenatal aneuploidy test is, if applied with the necessary caution and with careful explanation of its possibilities and limitations, a powerful tool for the clinician in the care of pregnant women. In the future it may become possible to extend this FISH test to samples of chorionic villi, as demonstrated in a recent report (Goumy et al. 2004).
Footnotes
Acknowledgements
Supported in part by the EU (ICA2-CT-2000-10012).