
Abstract
We report on the case of a pregnant woman with hyposomia who was previously suspected of having Turner syndrome. Prenatal cytogenetic diagnostics showed a fetal karyotype of 46,XX,dup(13)(q14.2q21.1) ish.13q14(RB1 × 3). Parental and grandparental chromosome analyses were performed and the dup(13) was found to be of maternal origin (de novo). The pregnancy was continued and a healthy female child was born with normal development apart from growth retardation. The reported chromosomal aberration is, together with two other cases reported in the literature, the first hint of a short stature–like phenotype due to dup(13)(q14.2q14.3).
S
We report on a case of a young, healthy pregnant women (CII) with hyposomia. CII was 23 years old and it was her first pregnancy. Short stature was remarkable in CII, with an adult height of only 146 cm. Her shortness was exceptional throughout her entire lifetime (Figure 1). Even though no other symptoms and no menstrual irregularities were observed, at the age of 8 years, CII was suspected of having Turner syndrome, because chromosome analysis revealed a very mild mosaic karyotype 46,XX/45,X (72/2). The young woman requested genetic counseling for a potential recurrence risk for her unborn child (CI) having a Turner syndrome. A normal fetal development was found at sonographic examination in 10 + 5 and 20 + 1 gestational weeks. In week 16 + 1, amniocentesis was performed and prenatal banding cytogenetics showed for CI a karyotype of 46,XX,dup(13)(q14q21); even a trisomy 13 was suspected after the prenatal rapid test (reported in Liehr et al. 2002a, case 1). Using multicolor banding(MCB) with a chromosome 13–specific probe set (Liehr et al., 2002b), the breakpoints could be refined to 13q14.2 and 13q21.1 (Figure 2). A chromosomal analysis of the parents revealed that the mother (CII) had the same unbalanced karyotype as the fetus (CI), caused by a de novo aberration in CII, as proven by exclusion of that aberration in her parents. In addition, a very mild Turner mosaic was found in CII (45,X,dup(13)(q14.2q21.1)[9]/46,XX,dup(13) (q14.2q21.1)[190]/47,XXX,dup(13)(q14.2q21.1)[1]. nuc ish(DXZ1 × 1)[21]/(DXZ1 × 2)[1476]/(DXZ1 × 3)[3]), a finding that is in concordance with the earlier analysis of CII during childhood. The partner of CII and her parents had normal karyotypes according to GTG banding analysis.
A polyhydramnion was detected by ultrasound in weeks 27 + 5 and 30 + 0, and a growth arrest must have occurred after the last sonographic examination in CI. At week 40 of gestation, the female child was born by cesarean section with Apgar scores of 6/8/9, a weight of 2750 g, and a length of 44 cm. Although the body mass index was within the normal range, the birth length fell below the third percentile. Postnatal examinations revealed a healthy girl with normal development apart from short stature and very mild dysmorphic signs (low-set ears, sandal gaps, mongoloid palpebral axis, long eyelashes). At the age of 6 months, the girl weighed 7220 g and her body height was 64.5 cm (>15th percentile). Motor and social development were 4 weeks accelerated. As an adult, the mother (CII) did not show any of the aforementioned mild dysmorphic signs present in CI, apart from hyposomia.

Family photo kindly provided by CII herself. CII (arrowhead) is shown at the age of 7 years. The difference in size from her parents and from her sister, only 2 years older, is obvious.
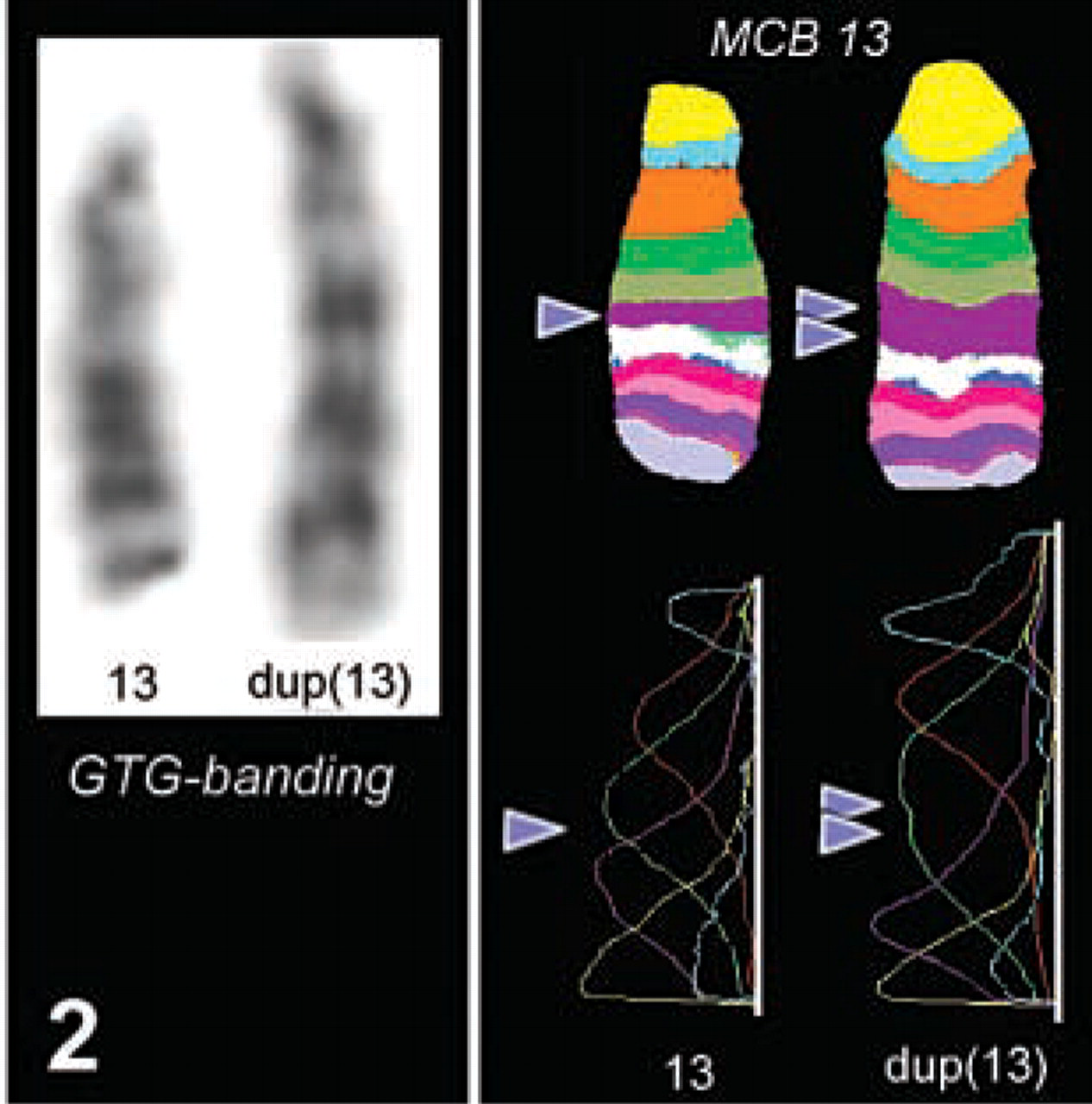
GTG banding and multicolor banding (MCB) result of the normal (13) and the aberrant chromosome [dup(13)] detected in CII and her child, CI. In GTG, the enlarged chromosome is clearly visible. However, the duplicated region, 13q14.2-q21.1, could be described exactly only after application of the MCB probe set for chromosome 13. The MCB result is shown in pseudocolor depiction and a fluorochrome profile (for technical details see Liehr et al. 2002b).
To the best of our knowledge, no patients with the identical chromosomal aberration, a dup(13)(q14.2-q21.1), are described in the literature. However, cases suited to pinpoint the critical region for short stature on chromosome 13 were reported previously. Duplications of the chromosomal region 13q13–13q14 were described as compatible with a normal (Rivera et al. 1981; Strong et al. 1981) or almost-normal phenotype (Turleau et al. 1983). In addition, Hermann et al. (2000) reported a dup(13)(q12q14) with short stature, heart defect, and developmental delay. On that basis, it can therefore be suggested that the critical “short stature region” of chromosome 13 is located in band q14.2-q14.3. However, this has to be confirmed by additional case reports.
In summary, this report presents another new differential diagnostic aspect for the short stature–like phenotype and underlines the importance of analyzing chromosomes in ambiguous cases.
Footnotes
Acknowledgements
Supported in part by the EU (ICA2-CT-2000–10012).