
Abstract
Postsurgical follow-up information was obtained on 64 dogs with 69 histologically well-differentiated melanocytic neoplasms that involved the mucous membranes of the lips and oral cavity. The patients received no adjunct therapy. Sixty one of 64 dogs (95%) were alive at the end of the study or had died of causes unrelated to the tumor, with a mean survival of 23.4 months and a median survival of 34 months after surgery. Twenty-eight dogs alive at the end of the study had a mean survival of 31.3 months after surgery. There were 2 dogs, which had recurrent tumors, that were still alive at the end of the study. All dogs that died of tumor-related causes (3) and all dogs with recurrent tumors (2) had tumors in the oral cavity.
Results of this study indicate that a favorable clinical course and prolonged survival can be expected in most dogs with histologically well-differentiated melanocytic neoplasms of the mucous membranes of the lips and oral cavity, with only local excision of the lesions and no adjunct therapy.
Melanomas are reported in multiple studies to be the most common oral malignancy in dogs. 10, 14, 15, 31 The aggressive behavior of malignant melanomas of the lips and oral cavity of dogs has been well documented, and some reports indicate that all melanocytic neoplasms that occur in these locations should be considered malignant. 6– 8, 14, 15, 19, 26, 31, 34, 35 It has been stated that melanomas may be one of the few neoplasms in animals for which location is an important prognostic indicator in its own right. 31 Use of the term “benign” for any melanocytic neoplasm of the lips or the oral cavity has been said to be unwise. 7 Survival time of dogs with malignant melanomas of the lips and oral cavity is reported to be short, ranging from less than 4 months in some studies 7, 34 to 5.7 months 27 and 8 months 18 in other studies. One of these earlier studies found that the time of survival after surgical excision of lip and oral melanomas was not significantly different according to the volume or location of the tumor. 18 However, several studies in the last 15 years showed that progress has been made in treating the least-aggressive forms (lower World Health Organization [TNM] Classification System stages 2, 17 ) of this disease. Dogs with some less-aggressive subgroups of oral melanocytic neoplasms are known to survive long periods after surgery, with or without adjuvant therapy. One study proposed an alternative staging system for oral malignant melanoma based on tumor size, location, and mitotic index. This alternative staging system resulted in improved prognostic predictability for both remission length and survival time. 17 After radiation therapy of 5 dogs with stage I tumors, 3 dogs with tumors of the lip survived or died of unrelated causes, whereas 2 dogs with tumors of the buccal mucosa died of tumor-related disease. 2 Another study of oral malignant melanomas reported median survival after radiation therapy of 86 weeks for tumors <5 cm3, which was significantly longer than that of dogs with larger tumors. 5 Postradiation progression-free survival of dogs with T1 oral melanocytic neoplasms was reported to be 38 months (mean) and 18.8 months (median), which was significantly greater than that of dogs with T2 and T3 tumors. 33 Intratumoral injection of a bacterial superantigen with a cytokine gene resulted in a median survival of 57 and 61 weeks for dogs with stage I and stage II tumors, respectively, which was significantly longer than the 24-week survival of dogs with stage III tumors. 11 In another immunotherapy study of oral melanomas, treated dogs in stage I had a significant increase in survival time compared with controls, with 80% of the treated dogs still alive at >2 years. 24 Multiple studies of xenogeneic DNA vaccines for control (but not prevention) of malignant melanomas showed some positive results and are ongoing. 1, 3, 4, 16, 23 For years, pathologists at the author's laboratory and elsewhere have encountered oral melanocytic neoplasms that have a histologically benign appearance, 9, 12, 21, 30 and some studies reported low numbers of these oral melanocytic neoplasms that exhibit benign clinical behavior. 15, 26, 30, 32
In 2000, the American College of Veterinary Pathologists established an ad hoc committee on oncology to address the current and future diagnostic and prognostic needs of veterinarians who treat animal cancer patients. 25 The author chaired a subcommittee of this ad hoc committee charged with investigating the biologic behavior of histologically well-differentiated melanocytic neoplasms (HWDMN) of the mucous membranes of the lips and oral cavity of dogs. Patients that had such HWDMNs surgically excised but received no adjunct therapy were followed up. The results of this study are contained in this article.
Materials and Methods
From surgical pathology samples received at ARUP Laboratories in Salt Lake City, Utah, between 1 October 2001 and 31 December 2003, dogs with melanocytic neoplasms from the mucous membranes of the lips and oral cavity that had a histologically benign appearance, as previously described, 13, 20, 35 were selected for follow-up study. More specifically, the tumors were distinctly pigmented with melanin (Fig. 1). In many tumors, large areas were so intensely pigmented that cytologic features were obscured. In less pigmented tumors and in less pigmented areas of heavily pigmented tumors, neoplastic cells were quite uniform in size and round or elongated. The cells contained small round-to-elongated nuclei; many nuclei exhibited a small, single, centrally placed nucleolus (Figs. 2, 3). The mitotic index was 3 or less per 10 high power fields (HPF), as has been described for benign melanocytic neoplasms of haired skin. 13 When possible, mitotic figures were counted in less pigmented areas or pigmented areas where nuclei could still be visualized. As in a previous study, if areas where nuclei were obscured by pigment were used in mitotic index determination, then these areas were given a mitotic index of 0. 7 To check this assumption, 6 of the heavily pigmented tumors were bleached, and the mitotic index was reassessed. In none of the bleached samples did the mitotic index exceed 1/10 HPF. In 4 of the bleached samples, the mitotic index was 0; one went from 1 in the unbleached sample to 0 in the bleached section.
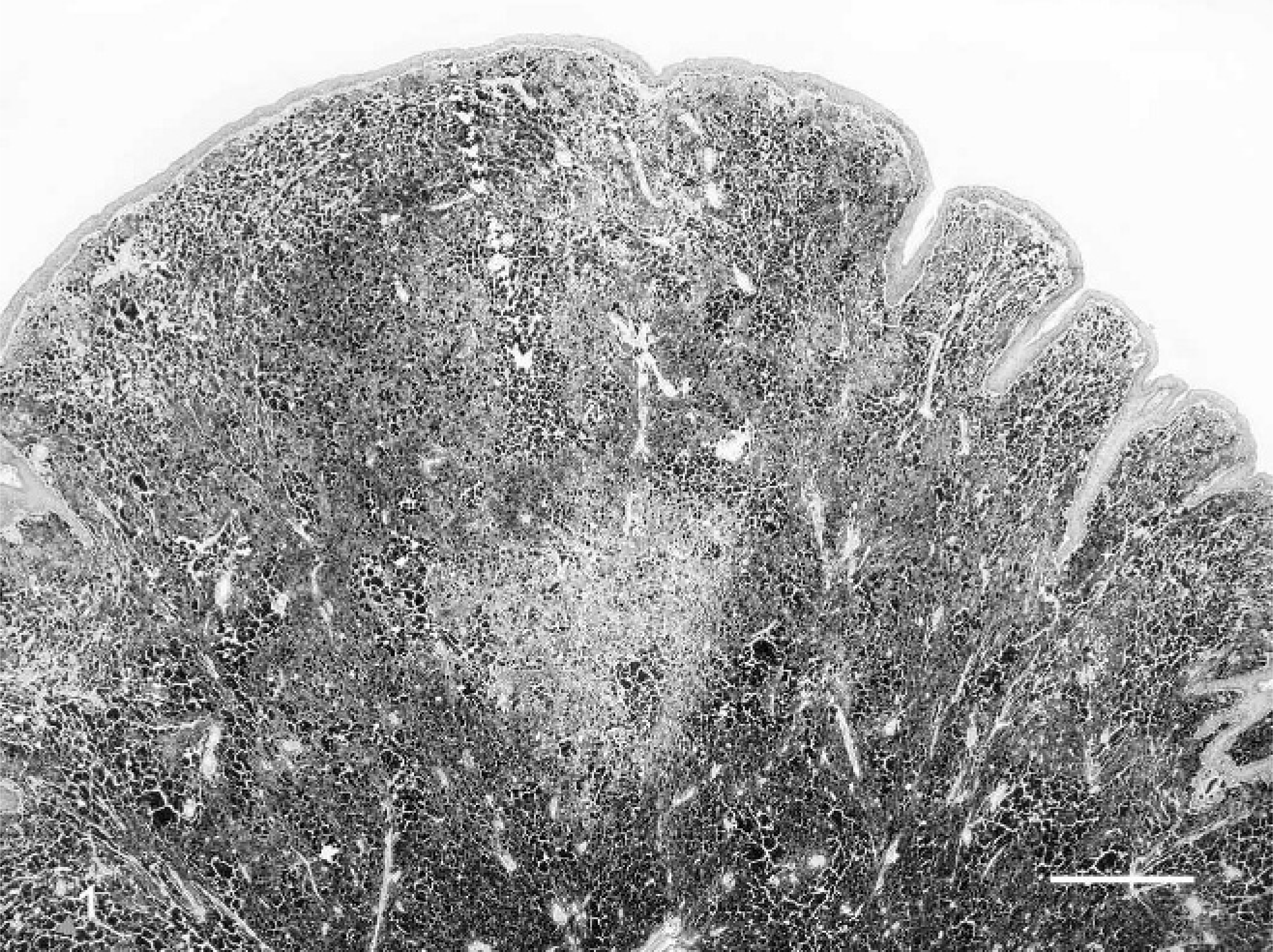
Histologically well-differentiated melanocytic neoplasm, lower lip; 9-year-old dog. Heavy melanin pigment obscures cytologic detail of many cells. An area of less-intense pigmentation is in the center. HE. Bar = 500 µm.
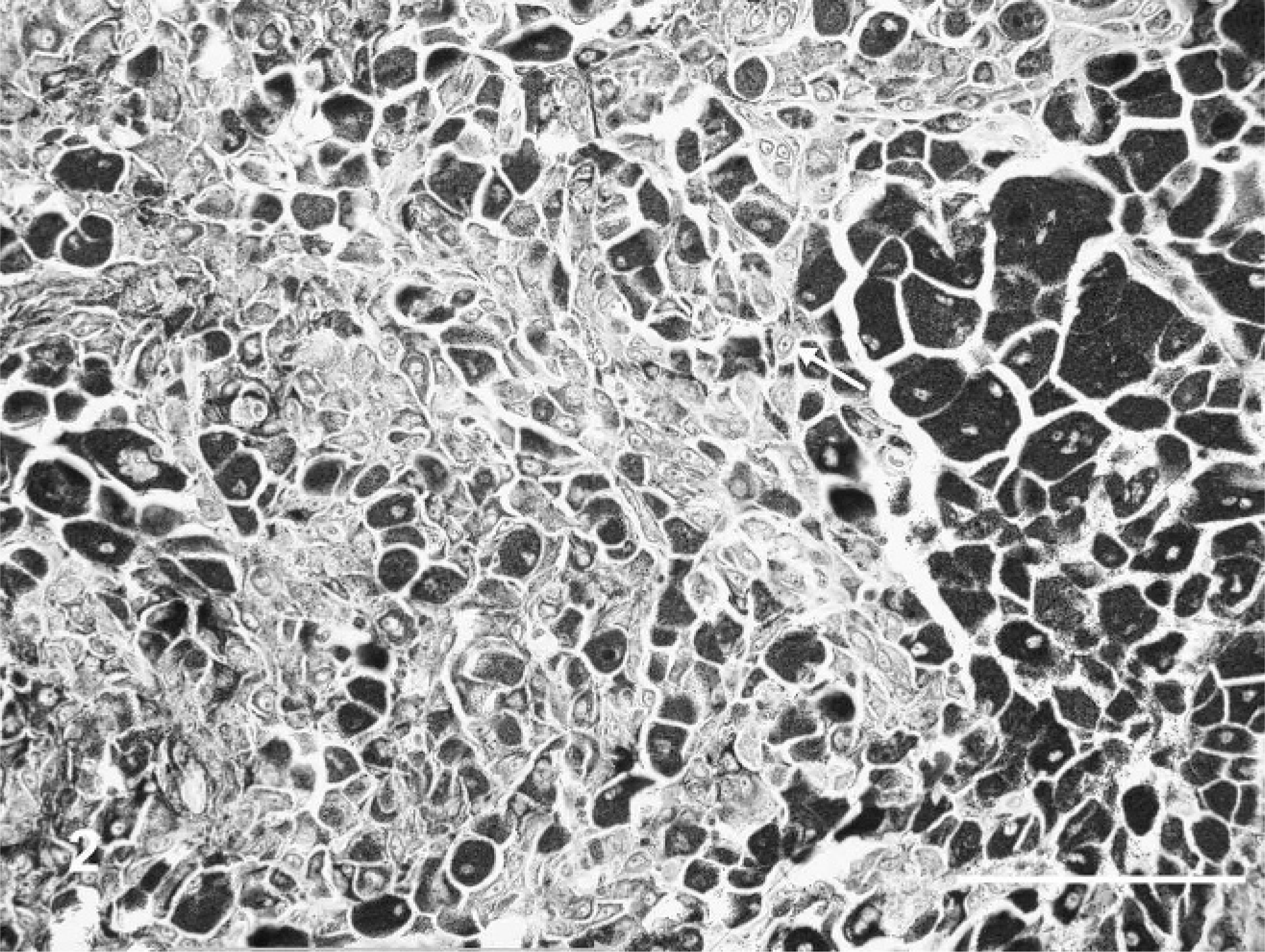
Histologically well-differentiated melanocytic neoplasm, lower lip; 9-year-old dog. Higher magnification of lesion in Fig. 1. Melanin obscures nuclei in some cells. In less intensely pigmented cells, nuclei have a single, small, central nucleolus (arrow). HE. Bar = 100 µm.
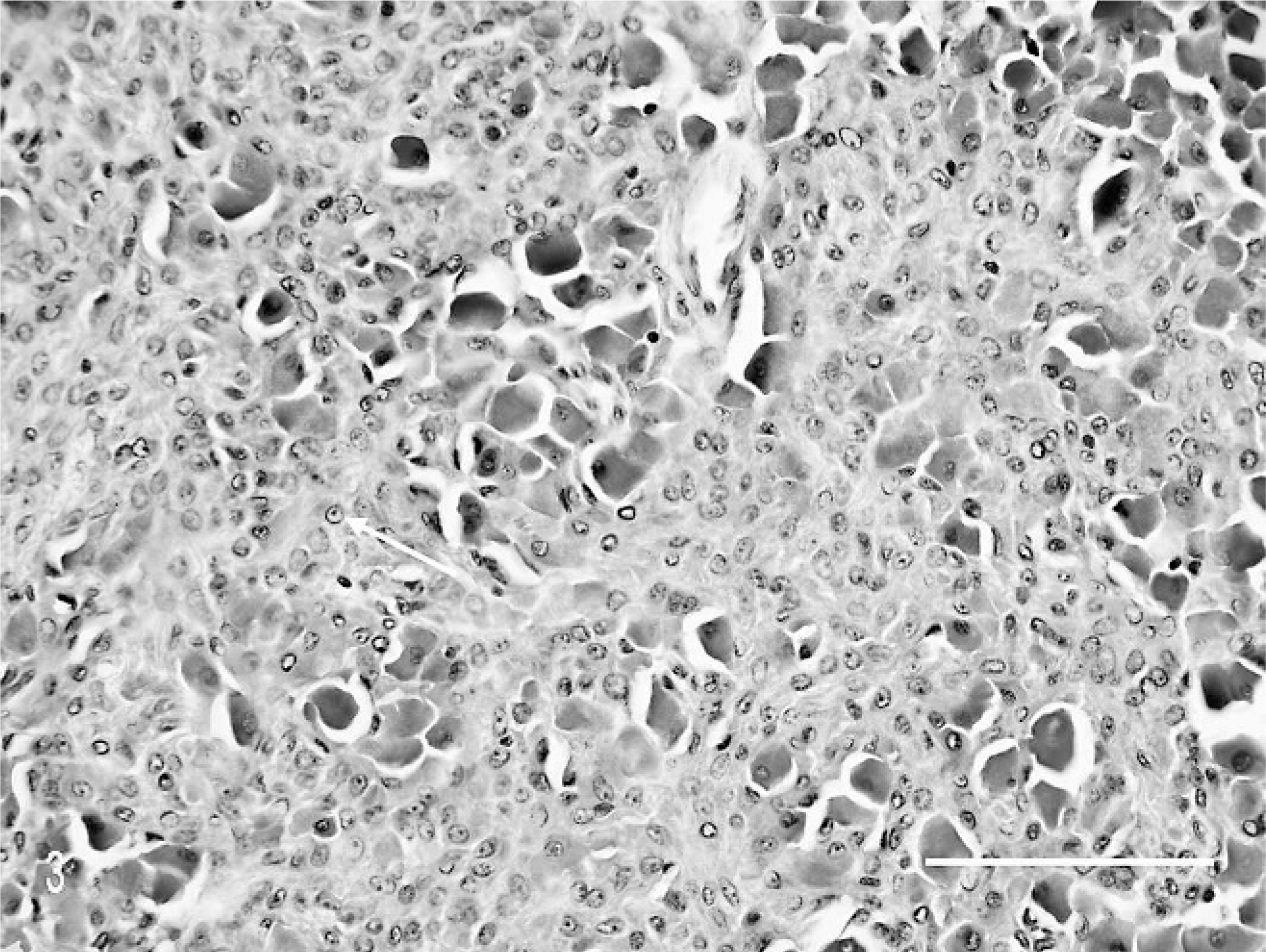
Bleached section of heavily pigmented area of neoplasm in Fig. 2, showing changes similar to those in less-pigmented areas of unbleached section. Note the single, small, central nucleolus in many cells (arrow). HE (bleached). Bar = 100 µm.
An initial report of the lesion(s) was sent to the submitting veterinarian. Every 6 months thereafter the author attempted to contact the veterinarian or, in some instances, the owner, by telephone to determine the status of the dog: 1) Was the dog alive? 2) Had the tumor recurred or spread? or, 3) If the dog had died, the date and cause of death. At the conclusion of the follow-up period on 31 December 2005, a final contact was made to determine the status of the dogs still living. All dogs in the study were placed in 1 of 4 categories: 1) alive with no tumor recurrence, 2) alive with local tumor recurrence, 3) dead of causes unrelated to the tumor, or 4) dead of tumor-related causes. Local recurrence was defined as clinically detectable recurrence of lesions after surgical excision but did not include lesions that were known to be incompletely excised at the time of surgery. Necropsy results were generally not available for any of the dogs in this study, so causes of death were obtained through interviews with the submitting veterinarians.
Comparisons were made, by means of a chi-square test, between outcomes after surgical excision of histologically well-differentiated melanocytic neoplasms of the lips and oral cavity. All values of P < .05 were considered significant. All statistics, including Kaplan-Meier survival estimates and curves, were generated by using SAS software, version 9.1 of the SAS system for Windows (SAS Institute Inc, Cary, NC).
Results
From samples received at ARUP Laboratories between 1 October 2001 and 31 December 2003, 79 lesions surgically excised from the mucous membranes of the lips and oral cavity of 74 dogs were classified as HWDMNs. Six dogs were excluded from the study because of inadequate clinical follow-up. Two dogs that died in the immediate postoperative period of causes unrelated to the tumor and 2 dogs that had a malignant melanoma at another site were also eliminated. Six dogs that were tumor free when lost to follow-up 8 to 18 months after surgery were retained in the study.
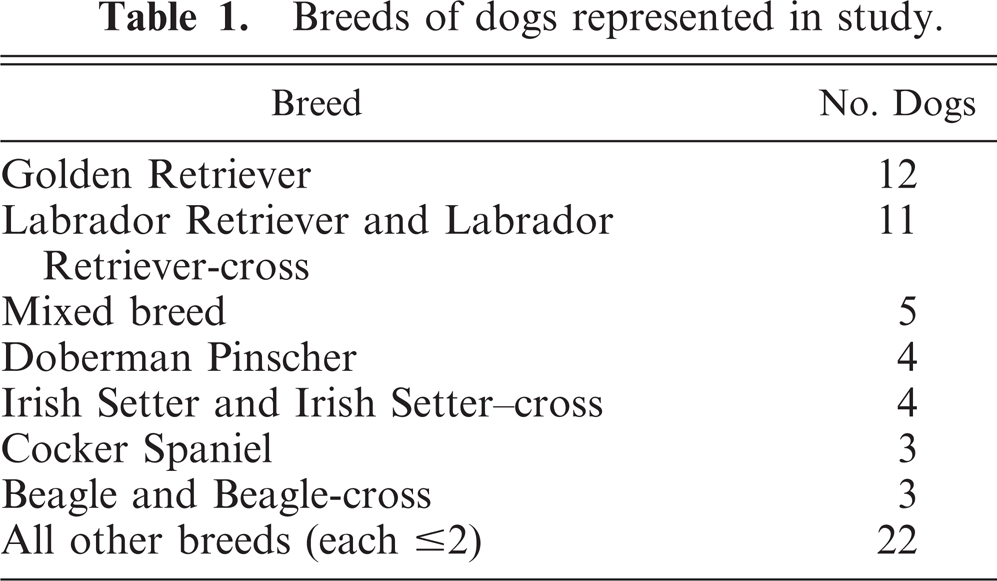
The 64 dogs included in the study represented 23 breeds and breed crosses, including mixed breeds (Table 1). Golden Retrievers (12) and Labrador Retrievers and Labrador Retriever crosses (11) were represented more than twice as many times as any other single breed. All veterinarians and laboratories that submit samples to ARUP Laboratories do not provide breed information, and the computer program used by ARUP Laboratories does not store breed information. Therefore, an accurate breed distribution for samples submitted to the laboratory could not be determined. However, breed popularity may have had some influence on the increased representation of Labrador Retrievers and Golden Retrievers. In 2002, Labrador Retrievers ranked first (and have done so for more than 15 years) and Golden Retrievers ranked second in the number of dogs registered with the American Kennel Club (www.akc.org). However, the breed that ranked third (German Shepherd Dog) was not represented among the 64 dogs included in the study, although there was 1 Rottweiler-shepherd cross. A previous study indicated that German Shepherd Dogs are not predisposed to oral melanomas. 27
Breeds of dogs represented in study.
One dog, which died of tumor-related causes, had an oral tumor removed by partial maxillectomy, and 1 dog, which died of unrelated causes 2 years after surgery, had an oral tumor removed by rostral mandibulectomy. All other tumors were removed by local excision. None of the dogs received postsurgical adjunct therapy. However, several veterinarians reported that the surgical bed was cauterized or lasered after local tumor removal.
Results are summarized in Table 2. Of the 64 dogs with 69 HWDMNs on which follow-up was obtained, 61 dogs (95%) were either alive at the end of the follow-up period or had died of causes unrelated to the tumor. (Included among those considered as having died of unrelated causes were 5 dogs that died at home but had had a tumor-free clinical examination within 3 months of death, and 1 dog that was euthanatized 15 months after surgery for an unrelated cause [posterior paralysis] but whose mouth was not specifically checked at the time of euthanasia.) The dogs that were alive or had died of unrelated causes had survived a mean of 23.4 months and a median of 34.0 months after surgery. The Kaplan-Meier survival curves for dogs dying of tumor-related causes and for dogs dying of all causes are shown in Fig. 4. Of the dogs alive at the end of the study, the longest surviving dog was 42 months after surgery, and the mean survival of all 28 surviving dogs was 31.3 months after surgery (Table 2).
Survival of dogs after surgical excision of histologically well-differentiated melanocytic neoplasms of the mucous membranes of the lips and oral cavity.
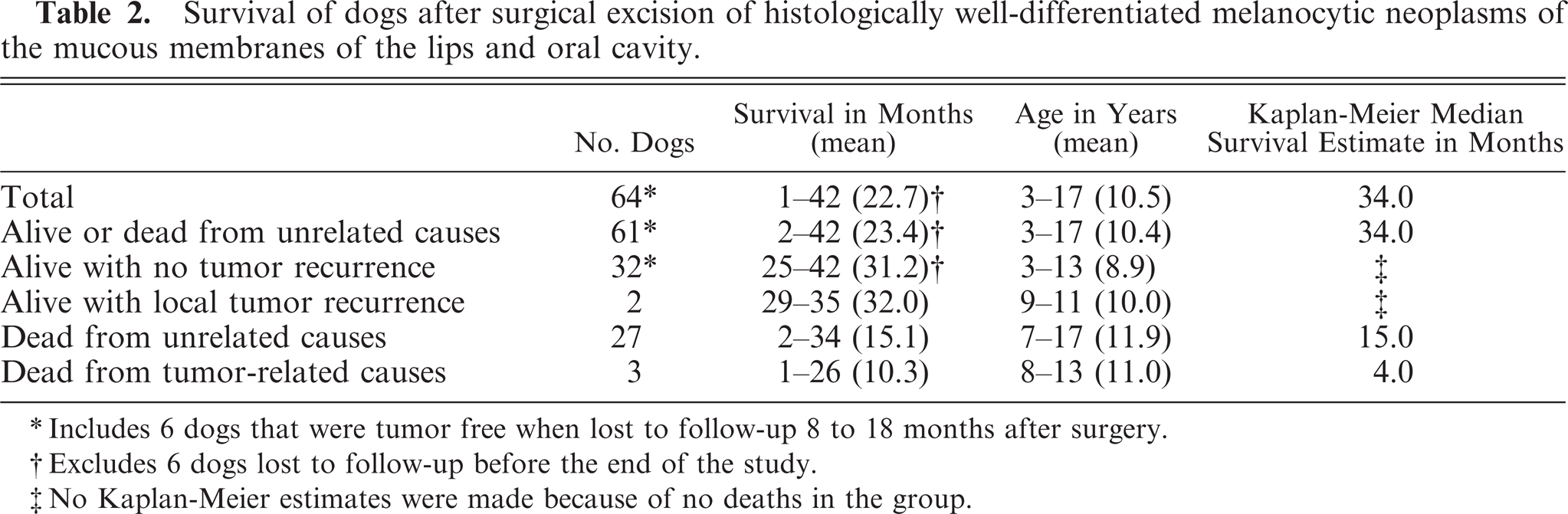
Includes 6 dogs that were tumor free when lost to follow-up 8 to 18 months after surgery.
Excludes 6 dogs lost to follow-up before the end of the study.
No Kaplan-Meier estimates were made because of no deaths in the group.
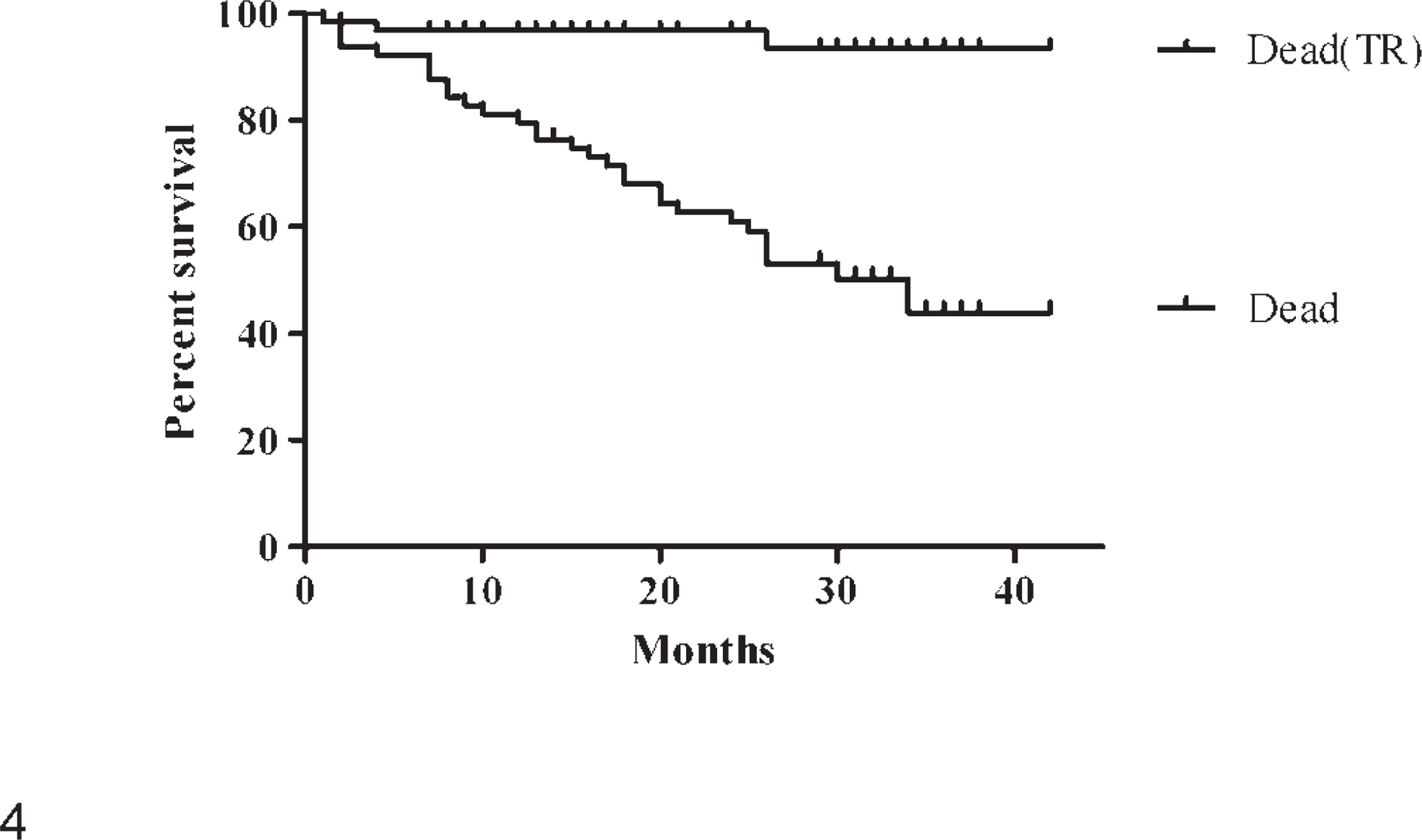
Kaplan-Meier survival curves of 64 dogs with HWDMNs of the mucous membranes of the lips or oral cavity. Dead (TR) = survival curve of dogs dying of tumor-related causes. Dead = survival curve of dogs dying of all (including tumor-related) causes.
Three dogs died of tumor-related causes. Two dogs that were alive at the end of the study had had local tumor recurrence. Two of the dogs that died from tumor-related causes were euthanatized within 4 months of surgery because of suspected metastasis. One of these dogs had had 3 concurrent oral melanocytic tumors removed. The third dog that died of tumor-related causes had repeated local recurrence of the lesion beginning 5 months after surgery and was euthanatized 26 months after surgery, after the tumor spread into an adjoining sinus.
Of the 2 dogs that experienced local tumor recurrence but were still alive at the end of the study, 1 dog had local recurrence 20 months after surgery. The recurrent lesion was excised, and there was no further recurrence 9 months later, at the end of the study. In the second dog with a recurrent tumor, the recurrence occurred 35 months after surgery and was reported in the final follow-up inquiry at the end of the study. The 2 recurrent lesions were histologically evaluated and were still classified as histologically benign. There is a previous report of a histologically benign melanocytic neoplasm on the lip, which recurred locally without an adverse effect on the patient. 29
There were 2 dogs with oral tumors that did not have the entire tumor excised. One dog had a blackened area of gingiva near the lower incisors. The veterinarian did a punch biopsy that was histologically evaluated and was found to be a HWDMN. The blackened area of the gingiva remained static, without further surgery or other treatment, and the dog was alive at the end of the study 29 months after the biopsy. Another dog, included in those that died of unrelated causes, did not have the entire gingival tumor removed, because the owners did not want the surgeon to excise bone to ensure complete excision. The residual tumor remained the same size and the dog died 6 months after surgery of right-sided heart failure.
One dog that was euthanatized for unrelated problems 25 months after removal of a tumor from the lip, had no clinical evidence of local tumor recurrence. However, postmortem microscopic examination of tissue from the original tumor site revealed the presence of a few well-differentiated pigmented neoplastic cells. Neoplastic cells extended to the margin of the original tissue section, so it was not clear whether the clinically undetectable postmortem tumor cells represented residual unexcised tumor or early local recurrence.
Thirty-one dogs in this study had HWDMNs on the mucous membranes of the lips, and 33 dogs had lesions within the oral cavity (Table 3). The oral cavity was the tumor location in all dogs that died of tumor-related causes (3) and in all dogs that experienced local recurrence but were alive at the end of the study (2). The 5 dogs with postsurgical problems represented 15% (5 of 33) of the dogs with HWDMNs that originated in the oral cavity. The risk of postsurgical problems (tumor-related death plus local recurrence) was significantly greater for lesions of the oral cavity compared with those originating on the lips (P < .05). However, the risk of tumor-associated death was not significantly different between the 2 locations.
Outcome after surgical excision of histologically well-differentiated melanocytic neoplasms of the mucous membranes of the lips or oral cavity of dogs.
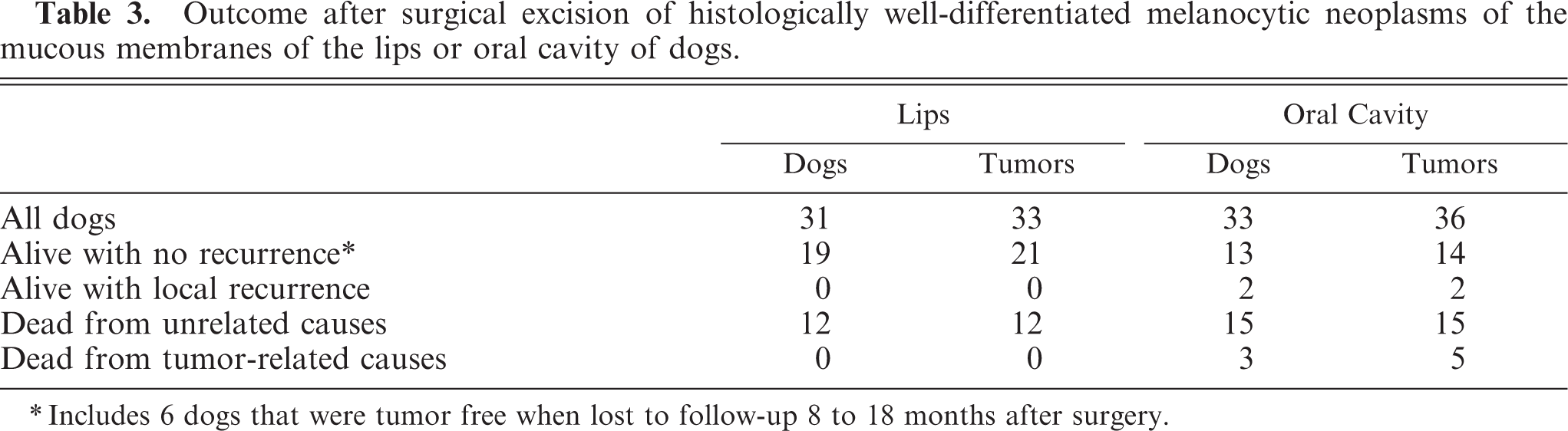
Includes 6 dogs that were tumor free when lost to follow-up 8 to 18 months after surgery.
Discussion
The veterinary literature is filled with reports that indicate the malignant character of melanocytic neoplasms that involve the mucous membranes of the lips and oral cavity of dogs. 6– 8, 14, 15, 19, 26, 31, 34, 35 Some more recent reports indicate progress in treating less aggressive forms of the disease. 2, 5, 11, 17, 24, 33 Some studies describe low numbers of apparently benign oral melanocytic neoplasms, 15, 26, 30 and a recent report identified a distinct subset of oral melanocytic tumors with clinically benign behavior. 32 One of these studies, and others, recognized oral melanocytic neoplasms that lacked histologic features of malignancy. 9, 21, 30
The current study found that most HWDMNs from the mucous membranes of the lips and oral cavity of dogs exhibited benign biologic behavior, with long-term postsurgery survival expected. Only 3 of 64 dogs that had such lesions died of tumor-related causes. Sixty one of 64 dogs were alive at the end of the study or had died of causes unrelated to the tumor, with a median survival of nearly 3 years after surgery (Table 2). This exceeds the 4–8 months survival for malignant melanomas of the lips and oral cavity reported in other studies. 7, 18, 27, 34 The 28 dogs that were still alive at the end of the study had survived a mean of 31.3 months (Table 2).
Even local tumor recurrence or incomplete surgical excision of HWDMNs does not necessarily indicate a poor prognosis and impending death. One dog had a locally recurrent tumor removed a second time and lived another 9 months after the second excision, with no further local recurrence. The dog was alive at the end of the study, 29 months after the original tumor excision. A second dog lived 35 months before a local recurrence and was alive at the end of the study period. Pigmented tumor cells extended to the margins of the original tissue sections from both these dogs, so it was not clear whether the newly detected lesions were truly recurrent or whether they represented residual neoplastic tissue. Another dog had a HWDMN removed from the lip only to have 2 additional HWDMNs develop 1 month later at new sites on the lip. These tumors were also excised, and the dog was alive at the end of the study, 38 months after the first tumor excision. Two dogs with incompletely excised tumors did not experience negative consequences from the tumors. The residual tumors remained static. One dog was alive at the end of the study, 29 months after surgery, and the other dog died of unrelated causes 6 months after surgery.
There are previous reports that indicate that the mitotic index in oral melanocytic neoplasms is not related to clinical behavior and survival. 7, 18, 27 Other reports found a strong correlation between the mitotic index and survival time for such tumors. 17, 32 Two reports indicated that the Ki67 proliferative index is a better prognostic indicator than the mitotic index for melanocytic neoplasms. 22, 28 However, one of these studies did not include melanocytic neoplasms that involved mucous membranes. 22 The HWDMNs in the current study were characterized by low mitotic activity. All tumors had a mitotic index of 3 or less per 10 HPFs, as has been established for benign melanocytic neoplasms in haired skin. 13 In most of the lesions (56/71), no mitotic figures were observed.
The size of the tumor was not a selection criterion in this study. However, most tumors (55/71) had a diameter of 1.0 cm or less in the tissue sections on the microscopic slides; only 1 tumor exceeded 2 cm (2.2 cm). Some of the larger lesions were pedunculated and had a narrow base of attachment. This small size may have contributed to the successful treatment of these HWDMNs, with only local excision.
A prior study found no significant difference between the death rate of malignant melanomas that originated on the mucous membranes of the lips and those in the oral cavity. 7 A more recent study found melanocytic neoplasms in the oral cavity to be more lethal than those that involved mucous membranes of the lips. 32 In the current study of HWDMNs, all 3 dogs that died of tumor-related causes and both dogs that had local tumor recurrence but were still alive at the end of the study had tumors that originated in the oral cavity (Table 3). These findings suggest less-aggressive behavior for neoplasms of the lip. However, other factors should also be considered. The location on the lips may allow for easier and earlier detection of tumors. Also, the structure of the lip may facilitate more complete excision compared with oral lesions where the proximity to bone may require more aggressive, bone-destructive procedures to obtain complete surgical excision.
Pathologists typically evaluate surgical margins by microscopy to determine if they are tumor free. However, a number of veterinarians who submitted tumors in this study indicated that the surgical bed had been cauterized or lasered after tumor removal. Thus, the microscopic surgical margin may not always correlate precisely with the effective tumor-free margin established in the patient.
Many dogs in this study were older (mean age 10.5 years) when the HWDMNs were initially excised. With only local excision, 60 of 62 dogs (97%) were still alive or were dead from causes unrelated to the tumors, which makes it difficult to justify painful and disfiguring surgery, or expensive chemotherapy to treat such well-differentiated lesions. Results of this study suggest that aggressive therapy beyond local excision is of little, if any, value in extending the life of these older dogs with HWDMNs. All dogs that died of tumor-related causes experienced tumor-associated problems within 5 months of surgery, with a median survival of 4 months (Table 2). Thus, in this study, if a dog survived 6 months after surgery without a tumor-related problem, a favorable clinical course related to the lip or oral HWDMN could be expected.
Because it has been well established that malignant melanomas from the mucous membranes of the lips and oral cavity of dogs can be very aggressive, 6– 8, 14, 15, 19, 26, 31, 34, 35 it seems prudent to excise all melanocytic lesions from these anatomic locations. However, clinicians and pathologists should not automatically assign a poor prognosis to all pigmented lesions that involve mucous membranes of the lips and oral cavity. Findings from this study indicate that such lesions should receive careful histologic evaluation, but, with few exceptions, HWDMNs warrant a favorable prognosis, with prolonged survival after only local excision.
Footnotes
Acknowledgements
I thank Drs. L. D. McGill, Sharon Wilson and Gordon Hullinger of the Animal Reference Pathology Division of ARUP Laboratories in Salt Lake City, Utah, for assistance in identification of cases and histologic review of lesions included in this study and Andrew R. Wilson of the Research and Development Informatics Division of ARUP Laboratories for assistance with the statistical analysis. I also thank the veterinarians who submitted cases and provided follow-up information for their cooperation.