
Abstract
Ossifying fibroma (OF) and fibrous dysplasia (FD) are benign, intraosseous, proliferative fibro-osseous lesions (PFOLs) characterized by replacement of normal bone by a fibrous matrix with various degrees of mineralization and ossification. Osteomas are benign tumors composed of mature, well-differentiated bone. Clinical, imaging, and histologic features of 15 initially diagnosed benign PFOLs and osteomas of the canine oral cavity were evaluated. Final diagnoses after reevaluation were as follows: OF (3 cases), FD (4 cases), low-grade osteosarcoma (LG-OSA) (3 cases), and osteoma (5 cases). Histology alone often did not result in a definitive diagnosis for PFOL. OF appeared as a well-circumscribed, radiopaque mass with some degree of bone lysis on imaging. Most lesions of FD showed soft tissue opacity with bone lysis and ill-defined margins. Low-grade OSA appeared as a lytic lesion with a mixed opacity and ill-defined margins. Osteomas were characterized by a mineralized, expansile, well-circumscribed lesion. Although histologic features of PFOLs were typically bland, the lesions diagnosed as LG-OSA had some features of malignancy (eg, bone invasion or a higher mitotic index). Treatment varied widely. Of the 10 dogs with benign PFOL or osteoma with known outcome (10/12), 9 showed either complete response (6/10) or stable disease (3/10) after treatment. Of the 2 dogs with LG-OSA with known outcome, 1 showed complete response after curative intent surgery, but 1 patient had recurrence after partial maxillectomy. Definitive diagnosis of mandibular/maxillary PFOL is challenging via histopathologic examination alone, and accurate diagnosis is best achieved through assimilation of clinical, imaging, and histopathologic features.
Keywords
Benign, intraosseous, proliferative fibro-osseous lesions (PFOLs) are a group of lesions characterized by replacement of normal bone by a proliferative fibrous matrix with various degrees of mineralization and ossification. In human medicine, benign PFOLs include ossifying fibroma (OF), fibrous dysplasia (FD), and cemento-osseous dysplasia (COD), among others. 1,13 Malignant lesions that may histologically resemble these benign intraosseous proliferations in the oral cavity must also be taken into consideration, including the rare low-grade osteosarcoma (LG-OSA). 1,30 Reports of PFOLs in small animals are few, 4,6,17,35,45,53,55 and some of the differential diagnoses considered in humans have never been described in animals. In veterinary species, in addition to “true” PFOLs (OF and FD), other disease processes that may be included in the differential diagnosis of these intraosseous lesions include osteoma, osteitis/osteomyelitis, fibrous osteodystrophy, conventional osteosarcoma (OSA), and multilobular tumor of bone (MLTB). 35,45,48,49
Ossifying fibroma is a rare benign neoplasm in the oral cavity of dogs, 4,10,35,45 while FD is classified as a dysplastic rather than neoplastic process as these lesions tend to be self-limiting. 13,20,43 Reaching a definitive diagnosis of PFOL poses a challenge for human and veterinary pathologists due to the extensive similarity in their microscopic appearance. OF, FD, and COD are characterized histologically by bland spindle-shaped cells surrounding woven bone trabeculae with no evidence of malignancy. 4,6,12,17,28,35,45,53,55 It is widely accepted that certain histologic features can distinguish between various types of PFOLs, such as the presence of osteoblasts lining woven bone spicules (osteoblastic rimming) in OF and lack of this lesion in FD. 35,45 Recently, however, it has been noted that osteoblastic rimming may be seen in both FD and OF, and therefore this criterion cannot accurately distinguish these 2 PFOLs. 20,44 Therefore, imaging features are used in human medicine to help distinguish these 2 entities: FD is characterized by poorly discernible borders that blend in with the surrounding bone (ill-defined margins), while OF appears well-circumscribed with sharply defined borders. 1,12,13,20,44 COD lesions are also well-circumscribed on imaging but often smaller in size than other PFOLs, self-limiting, and associated with tooth apices or at sites of previous tooth extractions. 1,20 Although not “true” PFOLs, osteomas, benign tumors of bone, also present as well-circumscribed mineralized masses on imaging but are histologically distinct, characterized by mature, well-differentiated bone. 15,16,24,39,51 Osteomas arise on the surface of intramembranous bones and rarely occur in extracranial locations. 24,39
The rare LG-OSA is included in the differential diagnosis of oral PFOL in human patients, given their benign histologic appearance. 3,27,30,50 LG-OSA often contains well-formed osteoid and bone, does not show extensive cytological atypia, is less cellular than conventional OSA, and has few mitotic figures. Bone invasion and subtle cytologic atypia help differentiate LG-OSA from benign PFOL histologically, and imaging may be suggestive of a more aggressive lesion. 3,27,30 LG-OSA may histologically resemble desmoplastic fibromas, low-grade fibrosarcomas, or FD. 3,30
To provide appropriate treatment and to rule out a more insidious process, definitive diagnosis of a benign PFOL requires assimilation of clinical and radiographic data, in addition to the microscopic features of these lesions. 1,13,44 The present study evaluated the clinical, diagnostic imaging, and histopathologic features of fibro-osseous and osseous lesions of the jaws in dogs and defined diagnostic criteria to help differentiate these lesions.
Materials and Methods
Medical records were reviewed from 15 dogs with oral masses initially diagnosed as OF, probable OF, FD, or osteoma. The biopsy specimens had been submitted to the Laboratory of Pathology and Toxicology at the University of Pennsylvania School of Veterinary Medicine between 2008 and 2012. Dogs were included in the study if they met the following criteria: (1) diagnosis of an intraosseous oral OF, FD, or osteoma confirmed on histologic examination of tissue samples; (2) diagnostic quality intraoral radiographs, radiographs, and/or computed tomography scan (CT) of the head; and (3) medical records available for review. Data reviewed for each dog included results of physical examination (including oral examination), complete blood count (CBC), serum biochemical panel, intraoral radiographs evaluated by board-certified dentists and a radiologist (JL, AR, JR); CT of the head evaluated by a board-certified radiologist and dentists when available (MSR, JL, AR, JR); histopathologic tissue samples examined by board-certified anatomical pathologists (MS, JE); cytopathologic mandibular lymph node examination by board-certified clinical pathologists; 3-view thoracic radiographic examination by board-certified radiologists; treatment duration; and outcome. Specimens were submitted in 10% neutral buffered formalin and demineralized in 15% formic acid, if needed, prior to trimming. Tissues were embedded in paraffin, sectioned at 5 μm, and stained with hematoxylin and eosin. The mitotic index was determined for 10 consecutive high-power fields (except for dog No. 5, in which multiple small samples were submitted for evaluation).
Results
Clinical Presentation
Patient age, location of the lesion, original and final diagnosis, follow-up, and treatment are listed in Table 1 (Suppl. Table S1 contains more complete information of population demographics). Clinically, the majority of the masses were described as nonulcerated, firm, and broad-based swellings. The most common location for OF, FD, and osteomas in the present study was the upper jaw (ie, maxillary, palatine, zygomatic, and incisive bones) (9/12). Only 1 osteoma, 1 OF, and 1 FD lesion were located in the mandible. All 3 cases of central LG-OSA were also located away from the mandible, in the maxilla, palatine, and incisive bones. Dog No. 7 had a necrotic center and dog No. 13 had a soft, fluctuant swelling behind the area of the missing left maxillary second molar tooth (210). Tumor volume ranged from 0.04 to 160.88 cm3.
Clinical and Follow-up Information of 15 Dogs With Maxillary and Mandibular OF, FD, LG-OSA, or Osteoma.
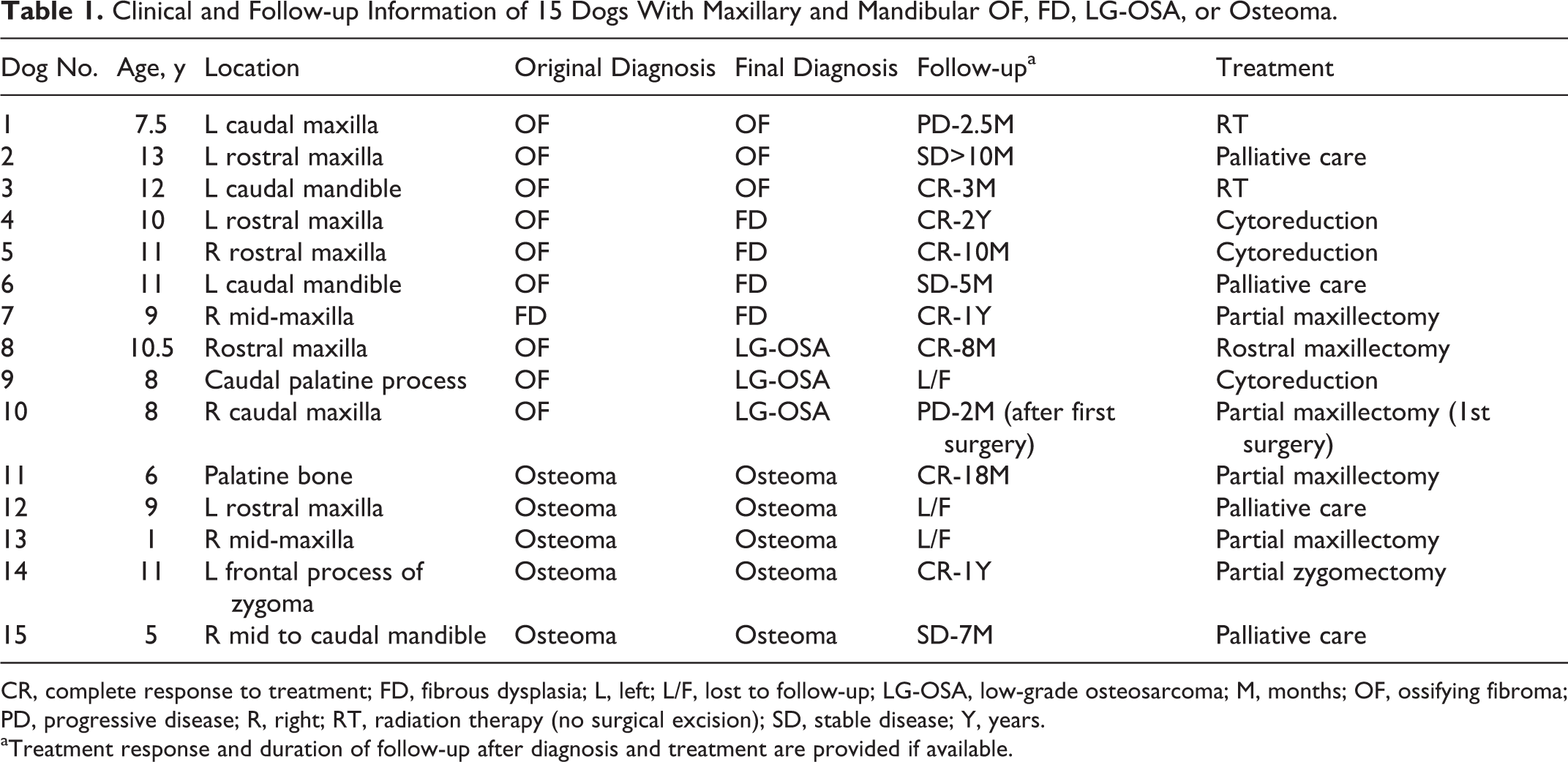
CR, complete response to treatment; FD, fibrous dysplasia; L, left; L/F, lost to follow-up; LG-OSA, low-grade osteosarcoma; M, months; OF, ossifying fibroma; PD, progressive disease; R, right; RT, radiation therapy (no surgical excision); SD, stable disease; Y, years.
aTreatment response and duration of follow-up after diagnosis and treatment are provided if available.
Pain was reported in only 2 cases (dog Nos. 1 and 3), both diagnosed as OF. Dog No. 3 was unable to fully open the mouth and had ipsilateral temporal muscle atrophy. Stertor and decreased nasal airflow were noted in dog No. 9. The jaw was reported to lock in an open-mouth position in dog No. 14. CBC and chemistry panel results are detailed in Supplemental Materials.
Histopathology and Imaging Findings
Nine dogs had an initial histopathologic diagnosis of OF, of which 3 were reclassified as FD based on imaging features (ill-defined margins), and 3 were reclassified as LG-OSA based on histopathologic features and review of imaging data (Table 1). One case was initially diagnosed as FD, and 5 cases were initially diagnosed as osteoma, and these were unchanged after assimilation of clinical, imaging, and histologic data. Computed tomography (CT) was performed in 8 dogs: 2 cases of OF (dog Nos. 1 and 3), 1 case of FD (dog No. 7), 2 cases of LG-OSA (dog Nos. 8 and 10), and 3 cases of osteoma (dog Nos. 11, 13, and 14). Pertinent CT findings are discussed below and expanded in Supplemental Materials.
All OF (3/3) consisted clinically and radiographically of well-circumscribed masses. Histopathologic evaluation revealed bland spindle-shaped cells surrounded by scant to moderate amounts of fibrovascular stroma and trabeculae of woven bone or mineralized spicules. Bone trabeculae were variable in number and thickness and, in some areas, lined by a single layer of osteoblasts (Fig. 1). Spindle-shaped cells of OF exhibited mild to moderate pleomorphism, and mitoses were rare (mitotic index ranged from 0–1 per 10 high-power field [hpf]). Osteoclasts were present in some of the lesions, often remodeling the bone trabeculae. Dog No. 2 was slightly different histologically, containing irregular mineralized spicules with “feathered” margins and occasional osteoid seams in addition to woven bone trabeculae (Fig. 3). OFs were expansile, mineralized masses with well-demarcated transition zones on imaging (Fig. 2 and Suppl. Fig. S1). Occasionally, there was bone thinning/destruction (dog No.1), most likely due to pressure atrophy (rather than active lysis). Tooth resorption was observed in 1 case (dog No. 3). CT of dog No. 3 (Suppl. Fig. S1) revealed a proliferative mass with an aggressive appearance but with well-demarcated transition zones.
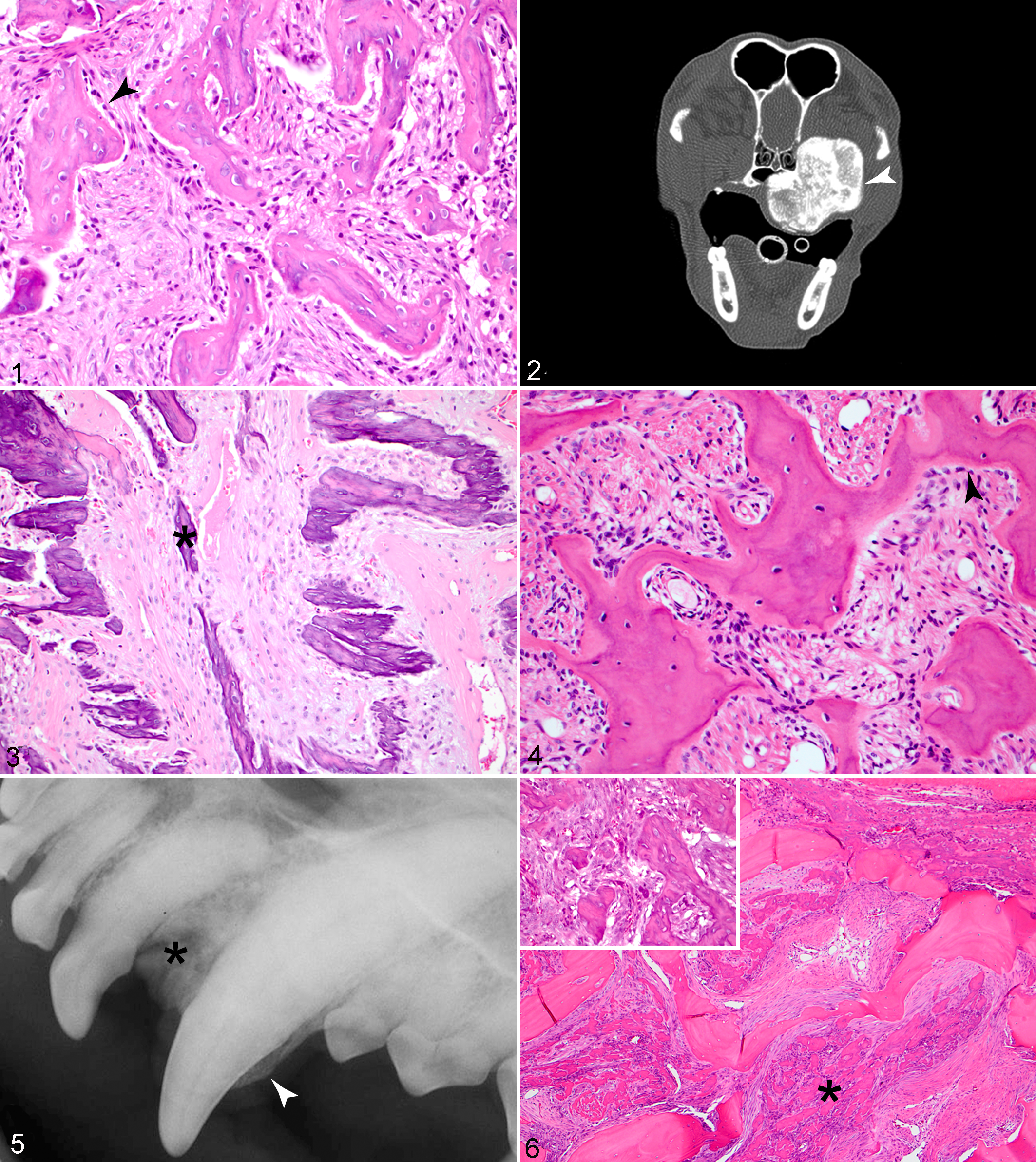
Four cases of FD were evaluated. Histologic findings were very similar to those described for OF in all cases, with bland spindle-shaped cells surrounded by scant to moderate amounts of fibrovascular stroma and woven bone trabeculae, occasionally lined by osteoblasts (Fig. 4). In some of the samples, the lesional bone merged with the adjacent cortical or alveolar bone, a key histologic feature of FD. However, it is important to note that many of the samples of OF and FD consisted only of small incisional biopsies, and the fragments often did not contain adjacent bone to evaluate this feature. Therefore, lesions were reclassified to FD if ill-defined margins were present radiographically and no evidence of malignancy was observed histologically. Mitotic index ranged from 0 to 1 (per 10 hpf), similar to OF. Dog No. 7 was originally diagnosed with FD, and arriving at a final diagnosis was challenging since an LG-OSA was considered in the differential diagnosis. Histologically, the fibro-osseous proliferation extensively replaced the adjacent alveolar bone, expanding bone marrow spaces, although not exhibiting invasion and expansion of osteonal canals (Fig. 6). In addition to ill-defined margins (Fig. 5), imaging findings for these cases included a soft tissue (dog Nos. 4 and 6) to mixed opacity (dog Nos. 5 and 7), cortical (dog Nos. 4 and 7), or permeative lysis (ie, multiple, small areas of radiolucency; dog Nos. 5 and 6); tooth resorption (dog Nos. 4, 5, and 7); and sclerosis mixed with lysis (dog Nos. 5, 6, and 7).
Three additional cases originally diagnosed as OF were reclassified as LG-OSA. On reexamination, these cases did not exhibit the typical histopathologic features expected of a benign OF or FD. Unusual features included a dense collagenous (almost desmoplastic) stroma (dog No. 8) (Fig. 7), invasion into osteonal canals (Fig. 9 inset and Suppl. Figs. S2 and S3) (dog Nos. 8 and 9), presence of cartilage (dog No. 9) (Suppl. Fig. S4), and/or increased nuclear pleomorphism and mitotic figures with small irregular mineralized woven bone trabeculae (Fig. 10) (dog No. 10). The mitotic index was 0 in 2 cases (dog Nos. 8 and 9) and 5 in dog No. 10. Intraoral dental radiographs and CT findings in 2 of 3 LG-OSA cases (dog Nos. 8 and 9) showed an aggressive bony lesion with bone lysis and/or cortical thinning (Fig. 8), a “sunburst” (ie, spiculated) periosteal reaction, and a mixed to mineral opacity with ill-defined margins. Since only head radiographs were available for dog No. 10, the periosteal reactions at the margins and transition zones of this lesion were difficult to assess due to the superimposition that occurs in these types of radiographs.
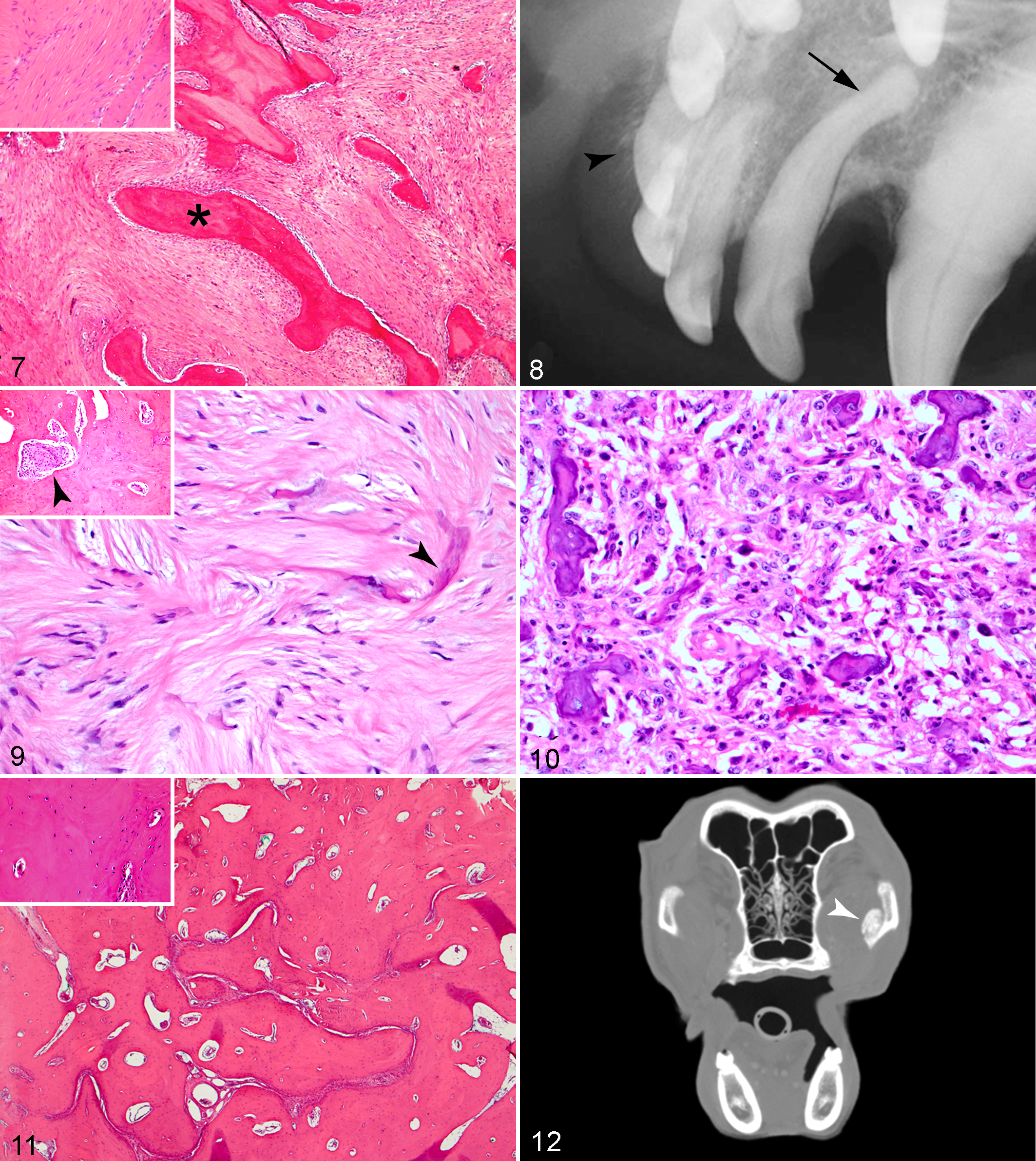
All osteomas (5/5) consisted histologically of dense bone with irregularly spaced osteocytes within lacunae (Fig. 11 and inset). The medullary spaces contained adipose tissue, blood vessels, scant amounts of fibrous connective tissue, and, occasionally, loosely arranged bone marrow stromal cells, osteoblasts, and osteoclasts. All osteomas also appeared as well-circumscribed, bony masses in imaging studies (Fig. 12). Peculiarities of certain cases included tooth resorption in dog No. 12, sclerosis of an edentulous region in dog No. 13, and a heterogeneous appearance in dog No. 14. Table 2 summarizes the imaging findings for all lesions in this study. Table 3 summarizes the differentiating histologic and imaging features of OF, FD, LG-OSA, and osteoma cases in this study (more detailed histologic and imaging information for many cases is presented in Supplemental Materials).
Imaging Characteristics of Maxillary and Mandibular OF, FD, LG-OSA, and Osteoma in 15 Dogs.
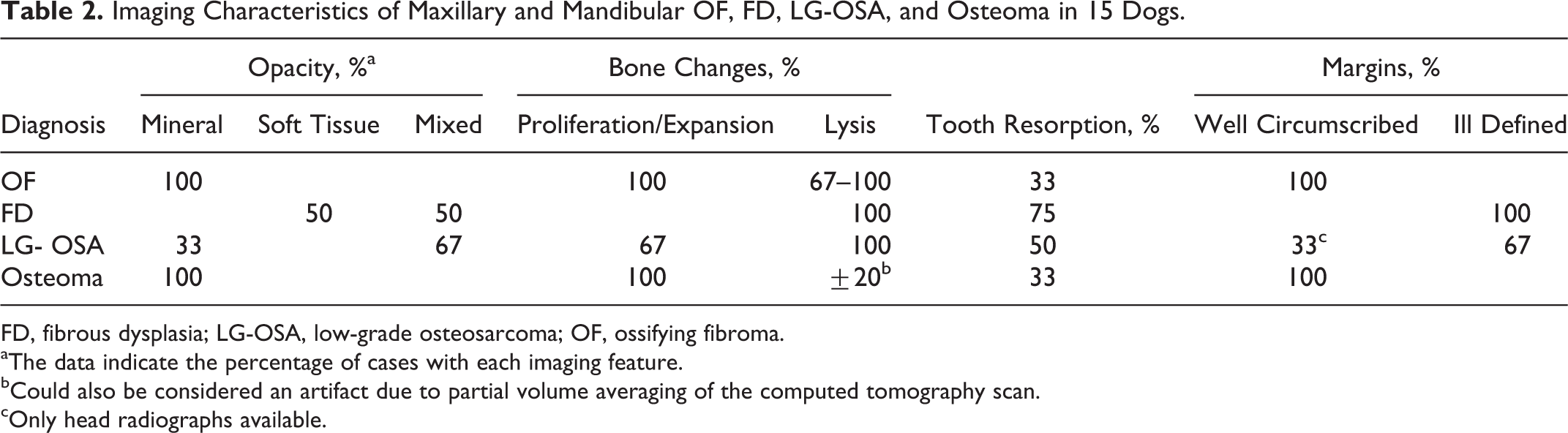
FD, fibrous dysplasia; LG-OSA, low-grade osteosarcoma; OF, ossifying fibroma.
aThe data indicate the percentage of cases with each imaging feature.
bCould also be considered an artifact due to partial volume averaging of the computed tomography scan.
cOnly head radiographs available.
Summary of Diagnostic Histologic and Imaging Features of Canine Maxillary and Mandibular OF, FD, LG-OSA, and Osteoma.
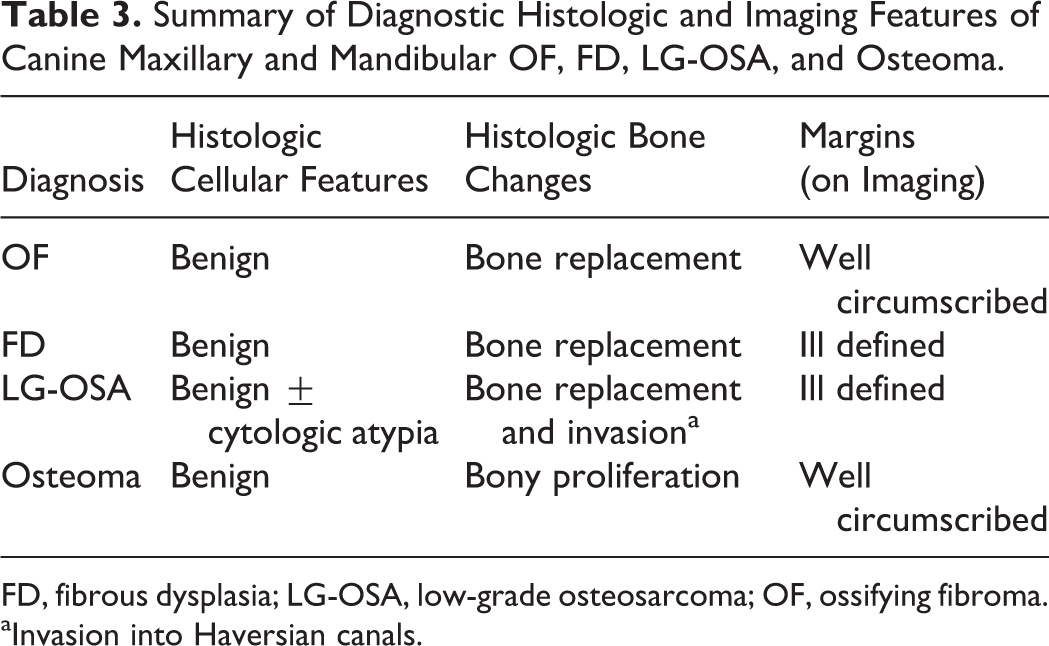
FD, fibrous dysplasia; LG-OSA, low-grade osteosarcoma; OF, ossifying fibroma.
aInvasion into Haversian canals.
Staging
Dog Nos. 1 and 4 presented with palpable mild enlargement of the ipsilateral mandibular lymph nodes. Dog No. 10 had evidence of mandibular and medial retropharyngeal lymphadenomegaly on CT. Mild bilateral mandibular lymphadenomegaly was noted in dog No. 11. Dog No. 14 had a larger retropharyngeal lymph node on the contralateral side seen on CT. Fine-needle aspirate of an ipsilateral or enlarged mandibular and retropharyngeal lymph node was performed in 8 of 15 patients; results were negative for the presence of metastasis in all cases. Evidence of metastatic disease was not reported for any patients receiving 3-view thoracic radiographs or thoracic CT (12/15).
Treatment and Follow-up (Table 1)
Two patients with a final diagnosis of OF were treated with full-course radiation therapy without surgical excision (dog Nos. 1 and 3). Dog No. 1 had continued growth of the mass 2.5 months after diagnosis and was euthanized, while dog No. 3 had no evidence of regrowth on evaluation 3 months after diagnosis. Dog No. 2 had stable disease for at least 10 months after diagnosis, on palliative care alone. Of the cases diagnosed with FD, 1 case had stable disease for 5 months (dog No. 6) with palliative care, 2 cases had no evidence of recurrence 10 months (dog No. 5) and 24 months (dog No. 4) after cytoreductive surgery, and dog No. 7 did not show any evidence of recurrence at 1 year after wide surgical excision. For the LG-OSA group, dog No. 10 showed recurrence approximately 2 months after initial resection. The patient died of acute respiratory distress syndrome soon after extubation from a second surgery to remove the neoplasm. Dog No. 8 did not show any evidence of recurrence at 8 months after wide surgical excision. Dog No. 9 was lost to follow-up. Two cases of osteoma (dog Nos. 12 and 13) were lost to follow-up, 1 case had stable disease for at least 7 months (dog No. 15) with palliative care, and 2 cases had no evidence of recurrence at 12 (dog No. 14) and 18 (dog No. 11) months after surgery.
Discussion
The occurrence of benign, intraosseous PFOLs in dogs is considered uncommon, and only individual case reports of these lesions exist in the veterinary literature, specifically OF and FD. 4,6,7,17,34,36,37,45,53,55 Differentiating benign PFOL of the jaw by histopathology alone is extremely difficult given the significant overlap in histologic features; therefore, diagnosis of a specific PFOL must take into consideration radiographic and clinical features. 1,13,44 Small biopsy samples and heterogeneity in the histologic appearance in the same PFOL are also often limitations for the pathologist. The histologic appearance of the PFOL in this case series (OF and FD) was similar among many specimens and often did not lead to a definitive diagnosis. In all cases of OF and FD described in this report, there was variable osteoblastic rimming of the woven bone trabeculae. Ultimately, final classification of a lesion as OF or FD relied on imaging data concerning a well-circumscribed mass for OF vs ill-defined margins for FD, as described in the human literature. 1,13,20,44 Sixty percent of the PFOLs (6/10) were reclassified upon reevaluation of biopsy samples in light of the imaging and, occasionally, histologic features. Of those initially diagnosed as OF, 3 cases were reclassified to FD based on imaging findings, and 3 cases were reclassified as LG-OSA based on imaging and histologic findings. In the present study, we also examined osteomas in addition to PFOLs (OF and FD). All initial diagnoses of osteomas remained the same after reevaluation.
Clinical signs of the patients with OF were similar to those previously reported, often asymptomatic with bone deformity and signs associated with continued expansion of the bony lesions. 35,45 However, pain has been occasionally reported previously, 35 as seen in this case series. Median age of OF cases in this case series was 11 years (7.5–13 years), which is within the range of 9 to 15 years previously reported in dogs. 4,35,45 Radiographic and CT appearance of OF in the present study was similar to previous reports in veterinary and human patients; these lesions were well-circumscribed (100%), proliferative (100%) lesions with a mineral opacity (100%). 4,33,35 The opacity of OF corresponds to the degree of mineralization and thus is largely dependent on the chronicity of the lesion. 42 Lysis was seen on imaging in 67% to 100% of OF cases in this study and has been previously described with canine OF. 35,45 A subset of OF in humans and horses, juvenile ossifying fibromas, also has been shown to have a more aggressive appearance with cortical destruction or breach. 37,40
FD has been reported in a variety of veterinary species. 6,17,25,29,31,54,55 In the present study, FD was diagnosed in patients between 10 and 11 years old. Radiographically, FD can vary from a radiolucent lesion to a uniformly mineralized mass. 17 FD was characterized by a soft tissue (50%) or mixed (50%) opacity, ill-defined margins (100%), and bone lysis (100%). A common feature in all cases was mild sclerosis intermixed with the areas of lysis. However, the characteristic ground glass or finely trabeculated appearance that is considered classic in human medicine was not appreciated in the cases described herein. The age of patients diagnosed with osteoma in this study ranged from 1 to 11 years with a mean of 6.4 years. Osteomas appeared as mineralized (100%), expansile (100%) masses with well-circumscribed margins (100%), with characteristic histologic features.
A rare neoplastic process known as central LG-OSA is included in the differential diagnosis of oral PFOL in human patients, given their benign histologic appearance. 1,3,27,30,44 In general, OSAs of the jaw are aggressive lesions, but the rare LG-OSA carries a better prognosis after complete, wide surgical excision. 3,30 A more invasive and infiltrative pattern histologically is often used as a differentiating feature of LG-OSA from FD, 3,27,30 although in reality, the distinction can be difficult based on histology alone. The presence of unusual histologic features in 3 cases, previously diagnosed as OF, resulted in their reclassification as LG-OSA. In the cases examined herein, aggressive bone invasion manifested as invasion and expansion of osteonal canals as described for human patients, 27 not just bone replacement or permeation/growth of the proliferating cells through bone marrow spaces. The entire lesion with wide surgical margins was submitted for histopathology in 2 of 3 cases that were reclassified as LG-OSA. The ability to evaluate the interaction of the lesion with the adjacent bone to identify bone invasion aided reclassification in these cases. Ill-defined margins (67%), mixed opacity (67%), and bone lysis (100%) were commonly noted in cases of LG-OSA. Hence, there is overlap in imaging findings for FD and LG-OSA. One LG-OSA showed well-defined margins on imaging, but only head radiographs were available for evaluation, and these showed mild lysis of the vomer bone. It is difficult to determine if the LG-OSAs described herein correlate to the grade I OSA previously reported in dogs. 8,21,23,32,46 Conventional, high-grade OSAs were not included in this study.
Tooth resorption was a common finding in the present report regardless of the final diagnosis, occurring in 33% of OFs, 75% of FDs, 50% of LG-OSAs, and 33% of osteomas with tooth involvement. Although tooth resorption has been associated with oral tumors in canine patients, including OF 35,45 and equine juvenile OF, 37 it occurs both at tumor sites and at sites distant from tumors, irrespective of tumor type. 38
A limitation to accurate classification of lesions in this study is the lack of 3-dimensional imaging for all cases. CT is considered an ideal imaging method for oral cavity masses since it allows for cross-sectional imaging and improved contrast resolution over conventional dental radiology. Although performed in only a few cases of this study, CT provided additional, valuable information that aided in determining the exact location and full extent of the tumor, the enhancement pattern, and the effect of these lesions on the surrounding structures. 26
The gold standard of treatment for PFOLs, osteomas, and LG-OSAs is removal with up to 2-cm margins to avoid recurrence. 4,17,35,44,46,51 Radiation therapy may be considered when complete surgical excision is not possible, but development of malignancies has been reported in previously radiated cases of human FD. 2,5,9,14,41,43,56 In human patients, recently it has been postulated that these cases of FD may have actually represented LG-OSA originally. 1,27 Of the 10 dogs with benign PFOL or osteoma for which the outcome was known (10/12), 9 showed either complete response (6/10) or stable disease (3/10) for at least 3 months (up to 2 years) after treatment, regardless of the final diagnosis. For LG-OSA, 1 case did not recur after wide surgical excision, while another case recurred approximately 2 months after initial surgical excision (cannot rule out initial incomplete excision).
The present study highlights the importance of collaboration between the pathologist, radiologist, and clinician in evaluating benign PFOLs due to their microscopic resemblance as well as their variable appearance on imaging. We have delineated diagnostic features of these lesions, as accurate classification remains a challenge. OF and FD exhibited variable and similar histologic features, only differing consistently in the radiographic appearance (well-circumscribed vs ill-defined margins, respectively). The term PFOL can be used in diagnostic veterinary pathology to encompass both OF and FD in the absence of imaging information. LG-OSA also had ill-defined margins on imaging; however, it showed histologic features of bone invasion or cytologic atypia. Osteomas, benign osseous lesions also included in this study, had characteristic histologic and imaging appearances. Taking into consideration the possibility of progression of disease, malignant transformation, and how little is known about these lesions in animals, consistent follow-up becomes extremely important during their long-term management. Prospective studies evaluating multimodal therapy and longer follow-up periods, CT and magnetic resonance imaging features, and perhaps the use of potential biomarkers 11,18,19,22 and assessing for genetic mutations described in human patients (eg, GNAS) are recommended. 47,52
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.