
Abstract
The parasite load in cervical, mandibular, and parotid lymph nodes and in the skin of the nose and the pinna from dogs infected with Leishmania infantum were investigated by histologic and immunohistochemical studies. Twenty-two infected dogs with and without signs of infection were examined to demonstrate correlation of signs with parasite load and the correlation of facial skin lesions with parasites in regional lymph nodes. Chronic inflammation of the skin was demonstrated in infected dogs that had no gross skin lesions, confirming that normal-appearing skin can harbor the parasite, likely playing a role in transmission. Dogs with facial skin lesions showed a higher parasite load in parotid lymph nodes than dogs without lesions of the facial skin, based on Leishman-Donovan unit analysis. Based on immunohistochemical analysis, parasite load in parotid and cervical nodes was correlated with that of skin of the nose and pinna, as was the parasite load in mandibular lymph nodes and skin of the external nose. We demonstrated a logical involvement of the lymphatic vessels and their specific anatomic draining sites.
Canine visceral leishmaniasis (CVL) is a severe zoonotic disease of the dog caused by protozoa of the Leishmania donovani complex, which are obligate intracellular parasites that represent an important public health problem in the tropical and subtropical regions of the world. Natural transmission of Leishmania is carried out by a species of sand fly of the genus Phlebotomus (Old World) or Lutzomyia (New World). 3 The dog is the domestic reservoir for human visceral leishmaniasis and many of the clinical and pathologic signs observed in dogs are similar to the pattern of the disease in humans. 1
There are few studies describing a systematic histopathologic evaluation of lymph nodes of dogs naturally infected with Leishmania infantum. Martinez-Moreno, 5 in a histologic and immunologic study, described a noticeable B-cell response in lymphoid tissues of dogs that were naturally and experimentally infected by L. infantum. Ciaramella et al., 1 in a retrospective clinical study of canine leishmaniasis in 150 dogs naturally infected by L. infantum, reported that cervical nodes were more reactive because of their anatomic position. Lima et al., 4 reported a histopathologic description of lymph nodes in dogs with a defined clinical status and the parasite burden of lymph node tissues. The aim of this study was to evaluate for Leshmaniasis in symptomatic and asymptomatic dogs and confirm that dogs with cutaneous facial lesions present higher amounts of parasite in regional lymph nodes.
Twenty-two mongrel dogs of unknown age were identified during an epidemiologic survey of CVL carried out by the City Hall Zoonosis Department of Belo Horizonte, MG (Brazil Southeast), based on positive test results using an enzyme-linked immunosorbent assay (ELISA) (optical density >100; >1 : 400 dilutions). Previous work with dogs obtained from the municipality of Belo Horizonte showed parasites identified as Leishmania infantum using a polymerase chain reaction (PCR) protocol. Indeed, liver tissue from a naturally infected dog showed a conserved region of kinetoplastidae (kinetoplast mini-circle DNA or kDNA) and hybridization with kDNA probes verified the presence of L. infantum. 8 The kDNA, which is present at thousands of copies per cell, has been used as a target for selective amplification of parasite DNA. All infected dogs were clinically classified as in previous studies 4 as follows: 10 symptomatic dogs (6 males and 4 females), 6 oligosymptomatic dogs (3 males and 3 females), and 6 asymptomatic dogs (2 males and 4 females). Of these, 6 dogs (2 oligosymptomatic and 4 symptomatic) had lesions on the skin of the head, specifically of the nose (dorsum of the muzzle) and pinna; and 16 did not have skin lesions on the head (6 asymptomatic, 4 oligosymptomatic, and 6 symptomatic). All the animals, independent of the presence or absence of facial lesions, showed parasites in internal organs (usually liver or spleen). An additional 6 dogs (1 male and 5 females) that tested negative by ELISA composed the control group. These dogs were obtained from the same epidemiologic survey.
All the dogs previously scheduled for euthanasia were sacrificed with 1.0 ml/kg of 2.5% intravenous thiopental and 0.3 ml/kg T61. The experimental protocol using dogs was approved by CETEA (Comitê de ética em experimentação animal – UFMG – number 034/2004). Samples of cervical, mandibular, and parotid lymph nodes and of skin from the external nose and pinna were fixed in 10% neutral-buffered formalin for 72 hours, and HE-stained sections were routinely prepared. Histologic sections were scored from 0 (no inflammation) to 3 (severe inflammation), considering the mononuclear cell (mainly macrophages) infiltrate in all anatomic regions of the cervical, mandibular, and parotid lymph nodes. Samples of liver, spleen, bone-marrow, and axillary, popliteal, and abdominal lymph nodes were also examined to confirm the Leishmania infection. Impression smears of tissues were air-dried and stained with 10% Giemsa. Amastigote forms of Leishmania were detected by light microscopy at 1000× under oil immersion. The lymph node parasite burden was expressed as Leishman-Donovan units (LDU) 4 determined by microscopic enumeration of Leishmania amastigotes per 1000 cell nuclei; the result was multiplied by the organ/tissue weight. The immunohistochemical protocol was carried out according to Tafuri et al., 2004. 9 The parasite burden was classified as follows: 0 = no amastigotes detected; 1 = small number of parasites (1–5 amastigotes or macrophages containing amastigotes); 2 = moderate number of amastigotes (5–10); 3 = large number of amastigotes (>10). Spearman nonparametric correlation test was used to identify relationships between the groups. The inflammation score and the score for the number of immunolabeled amastigotes were compared by the Kruskal-Wallis test. The LDU analyses were compared by the Mann-Whitney test. In all the tests, the accepted level of significance corresponded to P < .05.
Skin abnormalities were the most common manifestations of CVL. Thickening and distortion of the claws (onychogryphosis) (50%) and chronic cutaneous ulceration (45%), mainly located on the head, were the most frequent clinical features observed, followed by lymphadenopathy (32%). Other symptoms, such as alopecia (14%), anemia (9%), weight loss (9%), and dry desquamation/scaling (18%), were also observed.
In all lymph nodes, the capsules contained a moderate infiltrate consisting of lymphocytes, macrophages with or without intracellular Leishmania, and occasional neutrophils. The subcapsular sinuses were colonized by moderate numbers of mononuclear cells, and expansion of the sinus by edema was evident in some cases. The cortical region showed moderate follicular hyperplasia with germinal centers. The increased numbers of medullary cords and sinus mononuclear cells was the most prominent histologic alteration. In fact, it occurred in all cases, independently of the defined clinical status of the infected dogs. The medullary areas were closely packed with plasma cells, medium-sized and large lymphocytes (lymphoblasts), and macrophages (Figs. 1–3). Immunolabeled parasites were mainly found inside macrophages of medullary cords (Fig. 4).
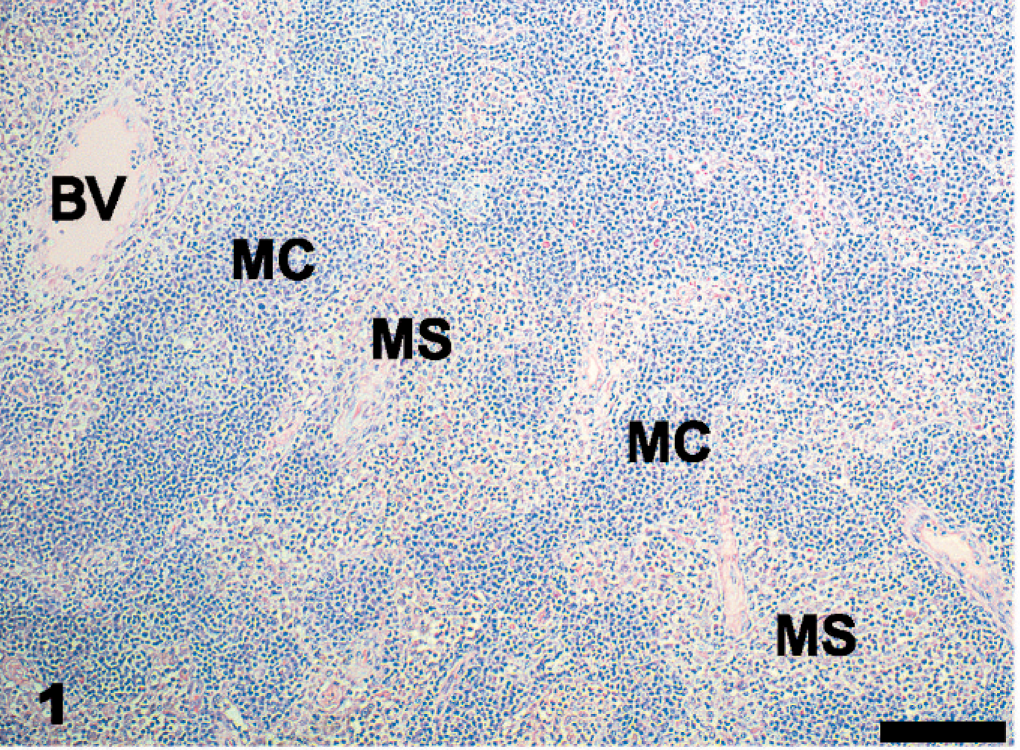
Parotid lymph node; dog. Medullary cords (MC) and sinus (MS) occupied by higher numbers of mononuclear cells. BV, blood vessel. HE. Bar = 100 µm.
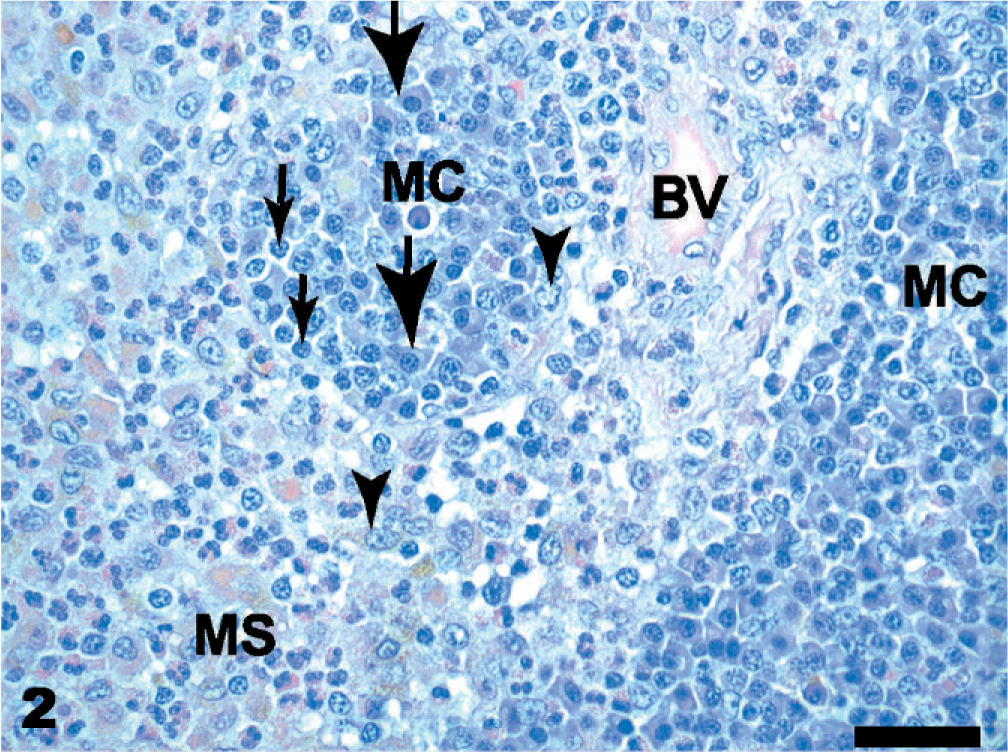
Parotid lymph node; dog. High magnification showing the increased numbers of plasma cells (large arrows), lymphocytes (thin arrows), and macrophages (arrowheads) of medullary cords (MC) and sinus (MS). BV, blood vessel. HE. Bar = 50 µm.
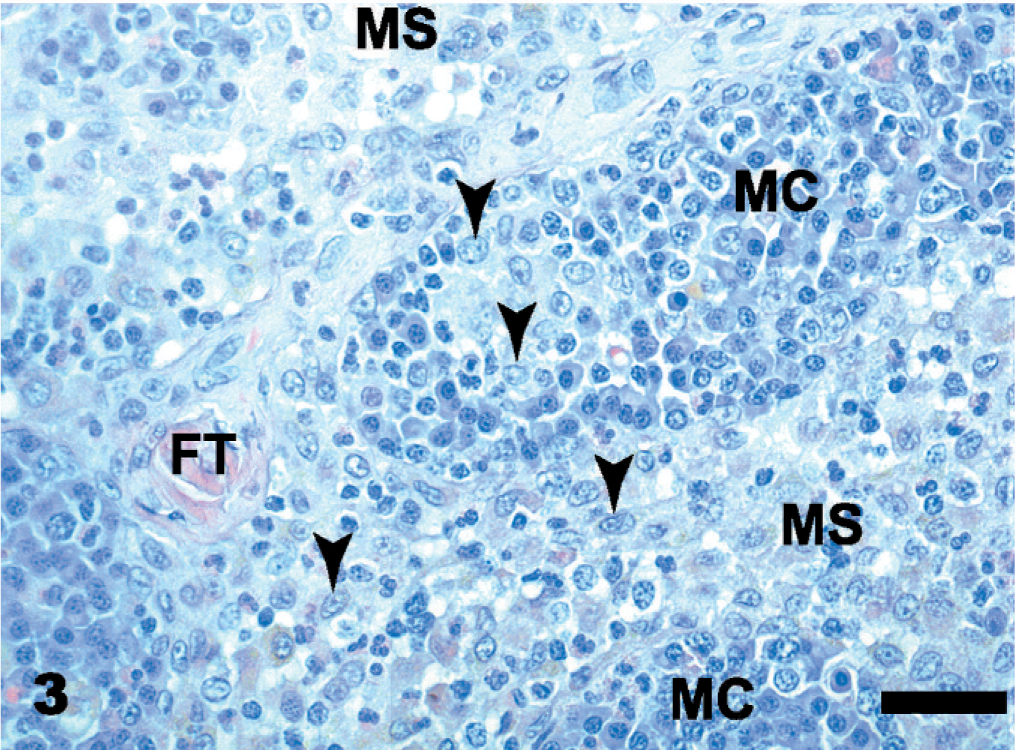
Parotid lymph node; dog. Higher magnification of epitheliod macrophages in medullary cords (MC) and sinuses (MC). FT, fibrous trabecula. HE. Bar = 50 µm.
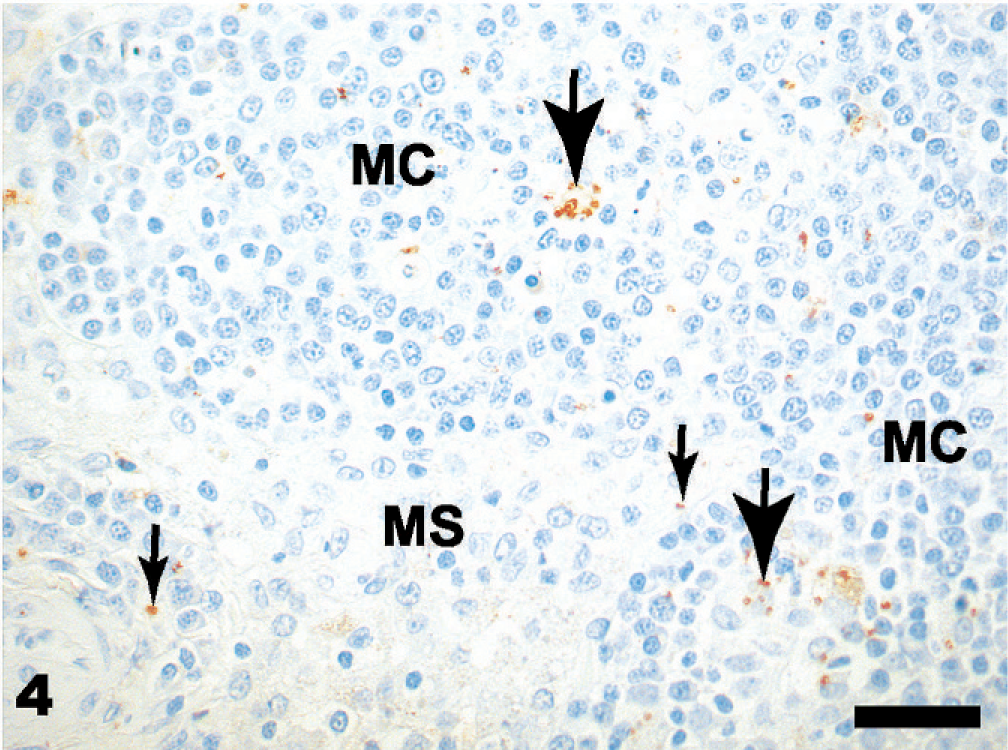
Parotid lymph node; dog. Immunolabeling of amastigotes of Leishmania sp. inside macrophages of medullary cords (large arrows) and sinus (small arrows) in a symptomatic serologically positive dog. Streptoavidin-peroxidase complex. Bar = 50 µm.
The medullary sinuses of mandibular lymph nodes had significantly higher inflammation scores in oligosymptomatic than in asymptomatic dogs (P = .027; Tukey test–analysis of variance [ANOVA]) (Fig. 5). The most intense histologic alteration in the parotid, mandibular, and cervical lymph nodes was in the medullary cords and sinus as compared with capsule, subcapsular sinus, and cortical region for each lymph node in all groups of dogs (Kruskal-Wallis test; P < .05).
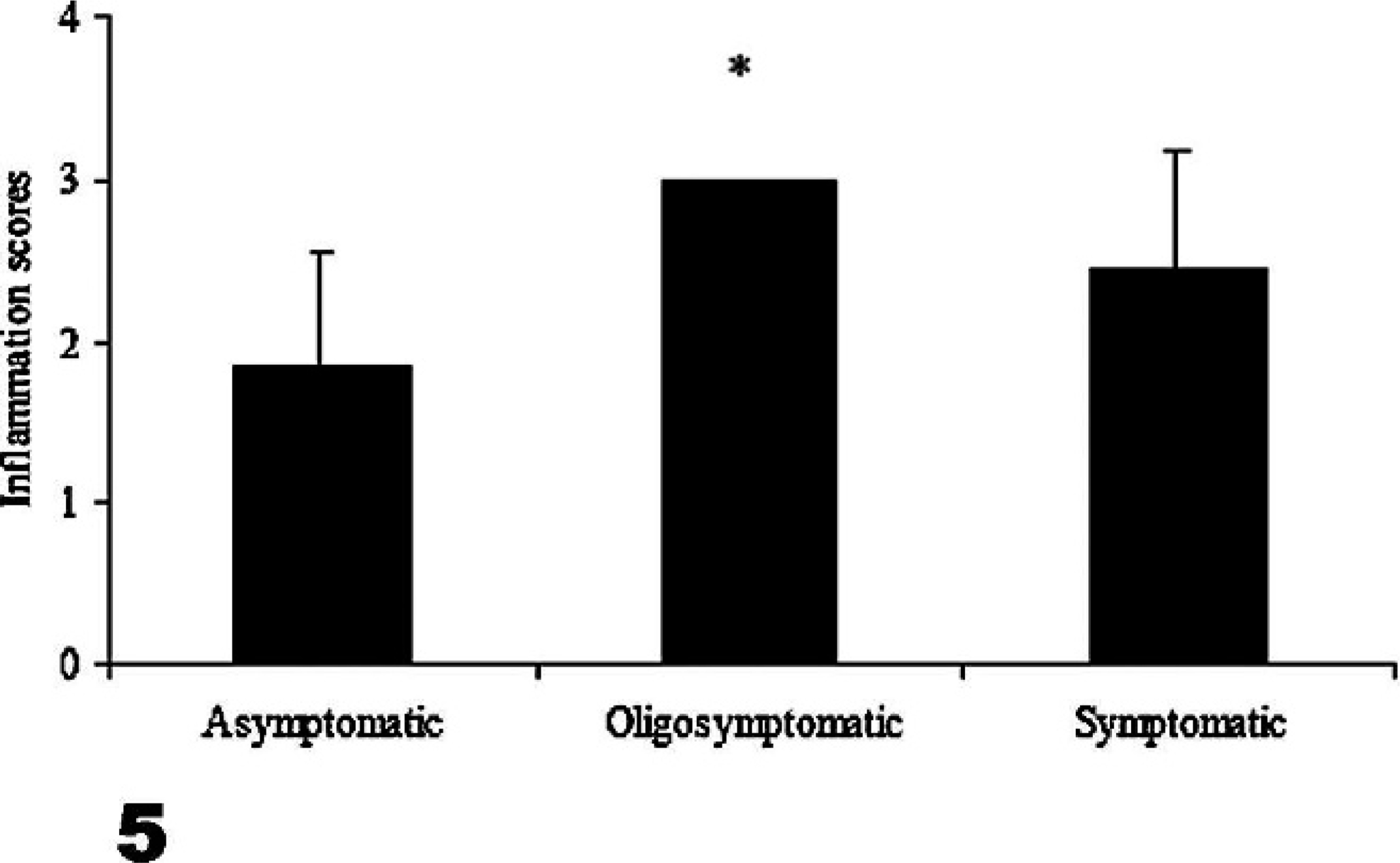
Inflammation scores in the medullary sinuses of mandibular lymph nodes, in dogs infected with Leishmania infantum. Inflammation scores were significantly higher in oligosymptomatic than in asymptomatic dogs (∗P = .027, Tukey test).
The various skin samples from the pinna and muzzle showed a chronic inflammatory reaction, characterized by a diffuse infiltrate of macrophages, plasma cells, and lymphocytes in the upper dermis, and focally around the small vessels and glands in the deep dermis. Many amastigote forms of Leishmania could be found in macrophages in all the skin samples, but parasitism was more intense in the sections from the pinna.
LDU analysis revealed that dogs with skin lesions affecting the head had higher parasite numbers in the parotid lymph nodes than dogs without skin lesions of the head (mean ± standard deviation [SD]: 0.03 ± 0.06 versus 0.0007 ± 0.002, P = .033, Mann-Whitney test), but similar differences were not detected for the mandibular or cervical lymph nodes.
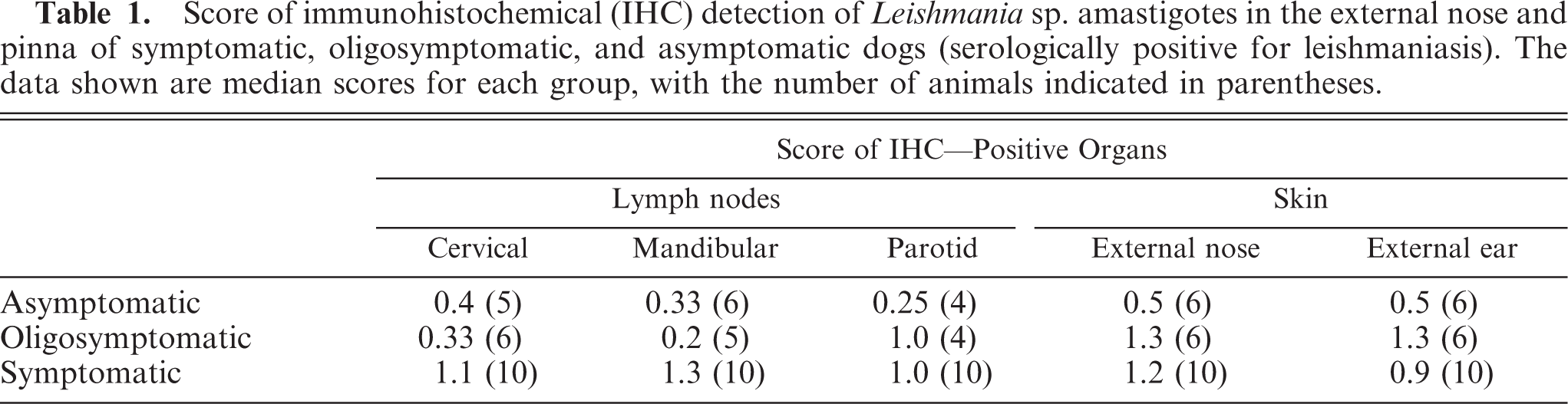
The immunohistochemical technique detected Leishmania in tissues of 13/22 (59%) dogs, compared with 6/22 (28%) for histologic examination of HE-stained sections. The semiquantitative immunohistochemical data showed a correlation between parasite load in lymph node and skin (Table 1). In particular, significant correlations were detected between the parasite load in parotid lymph nodes versus the skin of the pinna (P = .019, Spearman test) and nose (P = .005), between cervical lymph nodes versus skin of pinna (P = .012) and nose (P = .04), and between mandibular lymph node versus external nose skin (P = .021). However, there was no statistical difference among the tissue parasite loads of asymptomatic, oligosymptomatic, and symptomatic dogs.
Score of immunohistochemical (IHC) detection of Leishmania sp. amastigotes in the external nose and pinna of symptomatic, oligosymptomatic, and asymptomatic dogs (serologically positive for leishmaniasis). The data shown are median scores for each group, with the number of animals indicated in parentheses.
The parotid lymph receives afferent drainage from the external nose and pinna. In contrast, the superficial cervical (prescapular) lymph node drains the skin and subcutaneous tissue of the caudal regions of the head and auricle; and the mandibular lymph node drains the external nose, lips, cheeks, eyelids, lacrimal gland, and superficial muscles of the head. 6 In this work, we found that dogs with skin lesions of the head showed higher parasitism loads in the parotid lymph node than those without head skin lesions, confirming the relationship between lesions on the head and greater involvement of the lymph nodes that drain skin in the cranial region, as previously inferred by other researchers. 1, 4 The gross pathologic picture of the cervical lymph nodes was more prominent than that of the other nodes (data not shown), 1, 4 suggesting that cervical lymph nodes are more reactive because of their anatomic position. All lymph nodes of infected dogs showed chronic lymphadenitis. The histopathologic picture was similar for all cases irrespective of the anatomic location of the lymph node. Hypertrophy and hyperplasia of the cortical and medullary zones was a common feature. However, in most of the dogs, the essential architecture of the lymph nodes was preserved with no atrophic or degenerative areas. These alterations are in accordance with those described by Lima et al. in 2004. 4
Of interest, we found no relationship between clinical status and tissue parasite loads as detected by immunohistochemistry. Thus, although there were no statistical differences between symptomatic and asymptomatic dogs, it was possible to find asymptomatic dogs with heavier parasite loads than symptomatic ones. We believe that it may be of limited practical clinical use to classify dogs by the number and type of clinical signs during the course of visceral leishmaniasis. For example, some dogs with clinically severe leishmaniasis can present without cutaneous lesions or lymphadenomegaly and be classified as oligosymptomatic or even asymptomatic. Thus, these dogs could have been in a terminal stage of disease but were classified as asymptomatic. New classifications need to be developed by researchers to obtain more accurate results and conclusions regarding canine L. infantum infection. This finding also emphasizes the importance of asymptomatic dogs in the epidemiology of visceral leishmaniasis, since dogs without apparent clinical signs are able to infect sand flies and play a part in transmitting the parasites. 2, 4, 7, 10
Footnotes
Acknowledgements
This work was supported by a grant Consellho Nacional de Desenvolvimento da Pesquisa Tecnológica e Científica (grant CNPq 472287/01-0-NV), Brazil.