
Abstract
Two immunoglobulin G enzyme-linked immunosorbent assay (ELISA) versions using whole promastigotes of Leishmania infantum (syn. Leishmania chagasi) treated either with β-mercaptoethanol (β-ME-ELISA) or trypsin (TRYP-ELISA) as antigens were developed for the diagnosis of canine visceral leishmaniasis (CVL). By comparison with the direct agglutination test (DAT; 100%, 31/31; 95% confidence interval [CI]: 86.3–100%), slightly lower sensitivity was demonstrated for the newly developed β-ME-ELISA (93.5%, 29/31; 95% CI: 77.2–98.9%). Sensitivity was higher for β-ME-ELISA compared with TRYP-ELISA (87.1%, 27/31; 95% CI: 69.2–95.8%) in serum samples from dogs with CVL. When tested with sera from 37 healthy dogs and from 45 dogs with clinical conditions other than CVL, a specificity of 97.6% (80/82; 95% CI: 90.1–99.6%) was estimated for β-ME-ELISA as compared to 100% (82/82; 95% CI: 94.4–100%) and 95.1% (78/82; 95% CI: 87.3–98.4%) for DAT and TRYP-ELISA, respectively. Observed agreement was 94.0% (95% CI: 88.7–97.1%) between DAT and β-ME-ELISA (κ = 0.879; 95% CI: 0.803–0.956) and 87.4% (95% CI: 80.8–92.1%) between DAT and TRYP-ELISA (κ = 0.743; 95% CI: 0.636–0.851). Current results advocate application of the new β-ME-ELISA for diagnosis of CVL at the laboratory level and confirmation of results obtained with the DAT in field studies.
Keywords
In spite of its proven efficiency for diagnosis of canine visceral leishmaniasis (CVL), indecisive marginal titer readings (1:80–1:160) were reported for direct agglutination test (DAT) in dogs presenting clinical signs compatible with Leishmania infection (Semião-Santos SJ: 1996, Canine visceral leishmaniasis in Évora district, Portugal: a seroepidemiological study, PhD thesis, University of Amsterdam. Academic Pers BV, Amsterdam, The Netherlands). Recent improvements in the protocol of the DAT included the incorporation of β-mercaptoethanol (β-ME) in antigen processing and the addition of urea in the serum diluent to denature nonspecific agglutinating antibodies, subsequently contributing to enhance its diagnostic efficiency.1,4 In the present report, use of promastigote surface antigen favorably modified by β-ME or trypsin treatment and defined immunoglobulin conjugate for targeting immunoglobulin G (IgG) antibodies were combined to optimize the diagnosis of CVL.
A total of 151 serum samples from male and female dogs of different breeds, ages, and abilities were divided into 4 groups. Group 1 (G1) consisted of 31 dogs with confirmed CVL (lymph node aspirates positive for Leishmania). Group 2 (G2) consisted of 38 dogs with clinical signs typifying CVL but with negative lymph node aspirates for Leishmania. Group 3 (G3) consisted of 45 dogs with diseases other than CVL: 26 collected during the annual antirabies vaccination campaign in 2010 carried out in the municipality of Évora, Portugal; 16 from dogs diagnosed at the Veterinary Hospital of the University of Évora; and 3 from Brazilian dogs (municipality of Patos, state of Paraíba, Brazil). Final diagnosis for the 45 dogs was as follows: neoplastic disorders (n = 12), dirofilariasis (n = 8), babesiosis (n = 4), ehrlichiosis (n = 3), trypanosomiasis (n = 3), distemper (n = 3), hemorrhagic gastroenteritis (n = 2), cutaneous disorders (n = 2), autoimmune disorder (n = 1), leptospirosis (n = 1), leukemia (n = 1), conjunctivitis (n = 1), epilepsy (n = 1), acanthocheilonemosis (n = 1), respiratory disorder (n = 1), and toxocariasis (n = 1). Group 4 (G4) consisted of 37 healthy dogs with no history of CVL from the municipality of Évora that had negative lymph node smears and DAT-negative titers (≤1:160).
A Leishmania infantum (syn. Leishmania chagasi) strain (MHON/PT/01/IMT387) was continuously maintained in vitro by subculturing every 7 or 8 days at 26°C in liver infusion medium with tryptose and hemin, as described previously. 4 Preparation of the DAT antigen and performance of the test was done according to the improved version reported previously4,6 for diagnosis of human visceral leishmaniasis (HVL) and CVL. The antigen for β-ME-ELISA was processed as described for the improved version of DAT except for the staining step with Coomassie brilliant blue. The unstained intact promastigote antigen was preserved in a 1.2% (v/v) formaldehyde/citrate saline at a concentration of 1.5 × 108 per ml. For processing of the antigen in TRYP-ELISA the promastigote suspension was subjected to exactly the same handling procedures except that, instead of staining with Coomassie brilliant blue, promastigotes were treated as described for the original DAT version with trypsin. 5 The ELISA was performed according to procedures described previously, 16 with the exception that the whole promastigote antigen was previously treated either with β-ME or trypsin instead of being a soluble extract. After addition of substrate, a reaction was measured at a wave length of 490 nm. b Dilutions for both the β-ME–treated or trypsinized antigen were performed in 0.06 M carbonate/bicarbonate buffer (pH 9.6) at concentrations ranging from 1.5 × 105 to 5 × 107 promastigotes per ml. An antigen concentration of 2.5 × 106 promastigotes per ml, and conjugate c and serum dilutions of 1:1,000 and 1:100, respectively, were found to be optimal for both ELISA versions. The cutoff titers were determined as the averages of absorbance or optical density (OD) values obtained in the 37 sera from healthy dogs (G4) plus 3 times their standard deviation. Values of 0.26 and 0.44 were determined for β-ME-ELISA and TRYP-ELISA, respectively. To evaluate agreement beyond chance between tests, Cohen kappa value (κ) was determined, wherein κ < 0.4 was interpreted as weak, 0.4 < κ < 0.7 as good, and a κ > 0.7 as optimal agreement. Exact binomial test established confidence intervals (CI), with a 95% confidence level. 11
Out of 31 serum samples from dogs with confirmed CVL (G1), 29 (93.5%; 95% CI: 77.2–98.9%) scored positive in β-ME-ELISA, with absorbance values of 0.26–0.59. Only 2 sera reacted as negative in β-ME-ELISA, with absorbance values of 0.21 and 0.25. In none of 37 sera from healthy dogs (G4) were there cross-reactions detected in β-ME-ELISA. However, differently than in G4, 2 out of 45 dogs belonging to G3 revealed positive absorbance values of 0.40 and 0.28. The clinical condition in those 2 dogs was either infection with Trypanosoma cruzi or Microsporum canis. Based on these results, a sensitivity of 93.5% and a specificity of 97.6% (80/82; 95% CI: 90.1–99.6%) were determined for β-ME-ELISA. Out of the 31 dogs with confirmed CVL (G1) tested by TRYP-ELISA, 27 (87.1%; 95% CI: 69.2–95.8%) showed positive absorbance values of 0.44–0.83. Four dogs in this group revealed negative absorbance of 0.25, 0.30, 0.32, and 0.36. As for β-ME-ELISA, no cross-reactions were recorded for TRYP-ELISA with any of the 37 sera from the healthy dogs (G4) tested. However, when testing sera from dogs with diseases other than CVL (G3), 3 with Babesia canis, Acanthocheilonema, or M. canis infections and 1 with epilepsy scored positive absorbance values of 0.53, 0.48, 0.57, and 0.57, respectively. A sensitivity of 87.1% and specificity of 95.1% (95% CI: 87.3–98.4%) were calculated for TRYP-ELISA based on these results.
Among the 38 dogs with suspicion for CVL in G2, 25 (65.8%) tested positive in both β-ME-ELISA and TRYP-ELISA. Further, 8 (21.1%) dogs tested positive in β-ME-ELISA but negative in TRYP-ELISA, and 2 (5.3%) others were positive in TRYP-ELISA but negative in β-ME-ELISA. Only 3 (7.9%) dogs in group 2 tested negative in both tests. Should, in addition to parasite demonstration, clinical CVL manifestation and positive DAT titer (≥1:320) be accepted as criteria for final CVL diagnosis, as generally accepted for HVL cases, a sensitivity of 89.9% (62/69; 95% CI: 79.6–95.5%) or 78.3% (54/69; 95% CI: 66.4–86.9%) can be determined for β-ME-ELISA and TRYP-ELISA, respectively. Considering only results obtained with the serum samples from dogs with confirmed CVL, 2 were positive in β-ME-ELISA but negative in TRYP-ELISA. Compared with TRYP-ELISA, β-ME-ELISA showed higher sensitivity in detecting CVL (93.5% vs. 87.1%). At their respective absorbance cutoff levels, both antigens showed negative values (0.06–0.25 in β-ME-ELISA, and 0.08–0.38 in TRYP-ELISA) in the 37 sera from healthy dogs (G4). However, β-ME-ELISA revealed 2 cross-reactions, and TRYP-ELISA revealed 4 cross-reactions out of 45 sera samples from dogs with diseases other than CVL (G3). Based on these results, β-ME-ELISA showed higher specificity (97.6%, 80/82) than TRYP-ELISA (95.1%, 78/82). Observed agreement was 94.0% between DAT and β-ME-ELISA (κ = 0.879) and 87.4% between DAT and TRYP-ELISA (κ = 0.743), representing a good agreement beyond chance (Table 1).
Comparative diagnostic performance of direct agglutination test (DAT) and 2 enzyme-linked immunosorbent assays with β-mercaptoethanol (β-ME-ELISA) or trypsinized (TRYP-ELISA) modified antigens, in dogs with either confirmed visceral leishmaniasis (CVL; n = 31), suspicion for CVL (n = 38), disorders other than CVL (n = 45), and healthy dogs (n = 37).
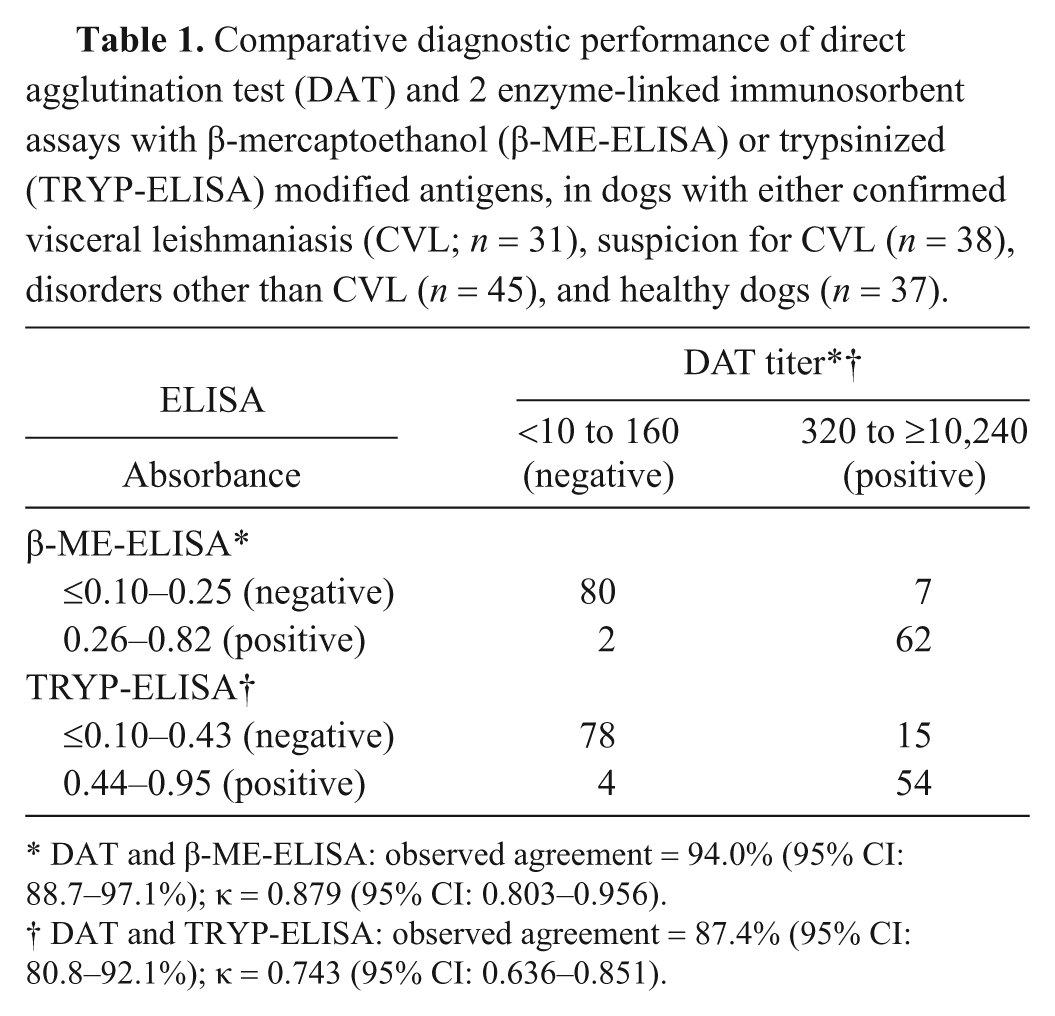
DAT and β-ME-ELISA: observed agreement = 94.0% (95% CI: 88.7–97.1%); κ = 0.879 (95% CI: 0.803–0.956).
DAT and TRYP-ELISA: observed agreement = 87.4% (95% CI: 80.8–92.1%); κ = 0.743 (95% CI: 0.636–0.851).
Several techniques using differently processed antigens have been introduced for detection of leishmaniasis in the canine host. Generally, for processing most of these antigens, intricate purification techniques and sophisticated equipment are required. Compared with these purified antigens, low specificities were reported for their crude equivalents in ELISA.8,9 The use of heterologous Leishmania strains and diversity of epitopes on the surface and somatic parts of the promastigotes are among the reasons for the low specificity reported. The urgent need for more sensitive and specific diagnostic tools has resulted in an increase in the number of ELISA versions.2,8-10,12,13,15 A previous study 1 combined the use of intact promastigote antigen modified through treatment with β-ME in an ELISA version for diagnosis of HVL, reporting a sensitivity of 93.3% and a specificity of 90.4%. Compared with a sensitivity of 93.5% herein recorded for β-ME-ELISA, the TRYP-ELISA version revealed a lower value of 87.1%. Although it had a lower sensitivity than the level reported previously 8 (87.1% vs. 100%), the newly developed β-ME-ELISA showed a relatively higher specificity (97.6% vs. 91.2%). Using a crude antigen of L. chagasi (syn. L. infantum), another study 15 obtained sensitivity of 98% and specificity of 100%. However, a much lower sensitivity (81%) was reported for an ELISA version in which a recombinant antigen was used. 14 The cross-reactions recorded for β-ME-ELISA in 2 out of 45 dogs could be due to either T. cruzi or M. canis infection. Similar cross-reactions were reported earlier against infections with Dirofilaria immitis, Cryptococcus species, B. canis, Ehrlichia canis, Neospora caninum, Toxoplasma gondii, Leptospira interrogans, and also T. cruzi.7,10,12,13,15
Following similar criteria currently adopted for HVL diagnosis, the combination of clinical signs typifying CVL and a positive DAT titer was considered as definitive also for CVL diagnosis. Accordingly, a sensitivity of 89.9% and specificity of 97.6% were estimated for β-ME-ELISA. The higher specificity rate herein recorded for β-ME-ELISA can be attributed to the favorable cleavage effect of β-ME on the promastigote surface of the Leishmania parasite as respectively suggested previously 1 in CVL and HVL. Both of the formaldehyde-fixed antigens in β-ME-ELISA and TRYP-ELISA showed comparable stable reactivity at 4 different occasions during the 2-month storage period at 4°C (data not shown). Microscopic examination of antigen aliquots during the period of storage revealed normal promastigote morphology and homogenous antigen suspensions.
Because none of the available serological procedures can provide absolute accuracy for CVL detection, the combined application of this newly developed β-ME-ELISA version together with DAT will increase the chance of better disease management both at the early and advance stages. One merit for β-ME-ELISA over DAT is that the former can be applied to specifically target IgM antibodies that are known to be good indicators of early disease onset. 3 Furthermore the use of the same (unstained) antigen makes it quite handy to perform the 2 procedures simultaneously. It is difficult however to conclude based on this limited number of sera that the β-ME-ELISA has the optimal efficiency for detecting CVL at both the early and advance stage. Nevertheless, the current study represents a practical and reliable laboratory method for the diagnosis of CVL.
Based on the high diagnostic usefulness and the relatively longer shelf-life time of the formaldehyde-fixed antigens (at 4°C), the newly developed β-ME-ELISA version can be recommended for routine CVL diagnosis at the laboratory level and as confirmation of results obtained with the DAT in field studies. Effective CVL can be achieved by a strategy of detecting asymptomatic Leishmania infection and prompt chemotherapy.
Footnotes
Acknowledgements
The authors thank Dr. A. J. Flor Ferreira, veterinary medical authority of the municipality of Évora (Câmara Municipal de Évora), Portugal, for his cooperation with the field work; Professor Lenea Campino, Laboratory of Leishmaniases, Institute of Tropical Medicine and Hygiene, Lisbon, Portugal, for providing the Leishmania strain; and the veterinary surgeons at the Veterinary Hospital of the University of Évora, for their support in collection of samples from dogs.
Notes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Saul J. Semião-Santos was financed by Science Program 2008 (contract no. C2008-UE/ICAAM05). This study was funded by FEDER through Operational Programme for Competitiveness Factors (COMPETE) and Foundation for Science and Technology (FCT) under Strategic Project PEST-C/AGR/UI0115/2011.