
Abstract
A 13-year-old spayed female Labrador Retriever with a 1-year history of progressive exercise intolerance was diagnosed with an interventricular mass in the heart via echocardiogram. The animal's general condition progressively declined over the next 8 months, and it was euthanatized. The intracardiac mass, which protruded into the lumen of the right ventricle, was removed at necropsy and fixed in 10% buffered formalin. Histopathologic diagnosis was an ectopic thyroid carcinosarcoma based on the presence of 3 distinct neoplastic tissue types. Intermixed within the tumor were neoplastic thyroid follicles containing colloid and solid nests of thyroid follicular epithelial cells, vascular channels and clefts filled with blood and lined by neoplastic endothelium, and osteoid surrounded by spindle cells and often rimmed by large multinucleated cells. Immunohistochemical reaction for thyroglobulin was positive in the tumor cells forming the colloid-filled follicles and solid nests of epithelial cells. Neoplastic endothelium was positive for factor VIII-related antigen. The thyroid gland was located in its normal anatomic position and was histologically normal, ruling out the possibility that the intracardiac tumor was a metastatic lesion. To the authors' knowledge this is the first reported case of an intracardiac ectopic thyroid carcinosarcoma, and possibly the first ectopic thyroid carcinosarcoma in any location in any species.
Primary cardiac neoplasms are rare occurrences in all species. Hemangiosarcoma is the most commonly reported cardiac tumor in dogs and is more commonly primary than metastatic in that location. 26 Intracardiac rhabdomyosarcoma, 20 osteosarcoma, 23 fibrosarcoma, 17 chondrosarcoma, 7 lipoma, 2 myxoma, 3 and an ectopic thyroid carcinoma 3 have all been documented in the canine. This report describes the clinical history, cardiac diagnostic findings, gross postmortem lesions, microscopic, and immunohistochemical features of an intracardiac ectopic thyroid carcinosarcoma in a dog.
A 13-year-old spayed female Labrador Retriever had a history of exercise intolerance for approximately 1 year and a grade III/VI left basilar systolic murmur ausculted on physical exam. Previous thoracic radiographs were considered normal and an electrocardiogram revealed atrial premature contractions with periods of supraventricular tachycardia. An echocardiogram revealed a mass associated with the interventricular septum and protruding into the right ventricular outflow tract resulting in elevated blood flow velocities at that site. Serum chemistry values were within normal limits as was a total T4 (23.7 nmol/l with reference range of 10.0–45.5 nmol/l). Over the next 8 months the dog became progressively more exercise intolerant, and eventually was reluctant to rise or eat. Because of declining quality of life, the owner elected euthanasia. A postmortem examination was performed.
Significant gross lesions were confined to the heart, with no evidence of generalized heart failure. Protruding into the right ventricle was a pedunculated oval mass, which was anchored to the endocardium of the interventricular septum by a thin stalk, cranial to the tricuspid valve and ventral to the pulmonic valve (Fig. 1). The mass was approximately 4 × 3 × 2 cm with 2 smaller red circular raised areas, 1 approximately 1 cm in diameter, the other approximately 2 cm in diameter, protruding from the surface of the primary mass. One end was extremely firm and the other more fluctuant. On cut section the mass was mottled with areas that were light tan and others that were dark red to black. Texture varied from friable to fibrous to bony (Fig. 2).
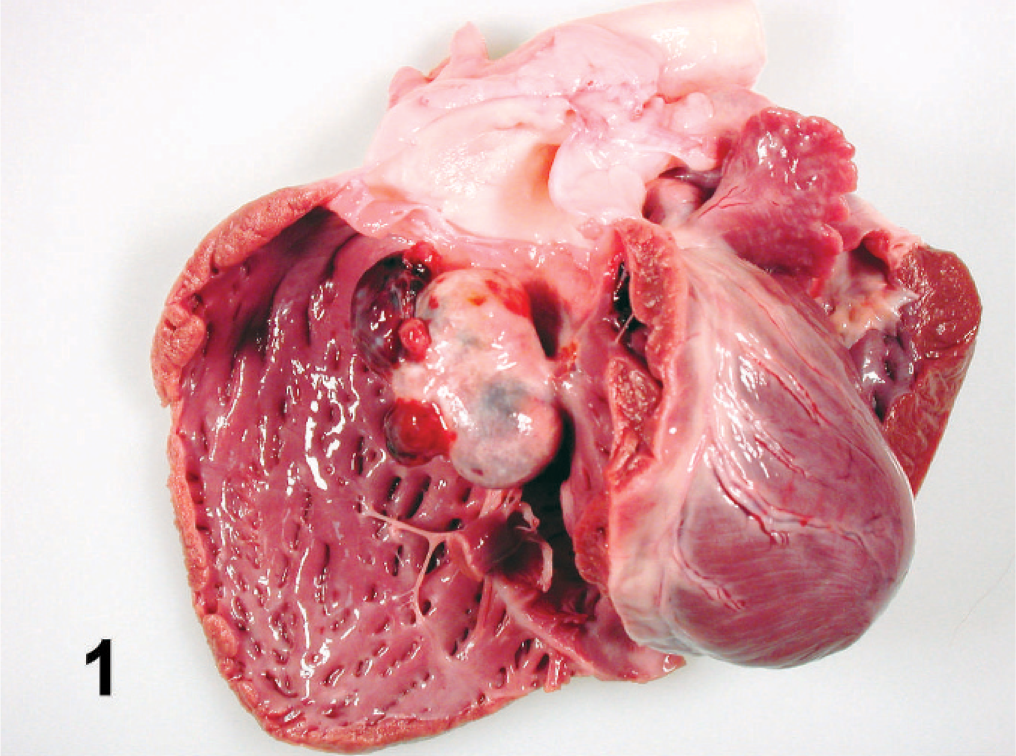
Heart; dog. A 4 cm × 3 cm × 2 cm pedunculated mass protrudes into the right ventricle, ventral to the pulmonic valve.

Intracardiac thyroid carcinosarcoma cut section; dog. The mass is multilobulated and mottled with light tan to dark red or black areas and friable to fibrous to bony texture. Bar = 1 cm.
Histologically, the mass was moderately cellular, well circumscribed, and surrounded by a thick fibrous capsule. The mass extended into the stalk that connected it to the interventricular septum but did not invade the myocardium. Three distinct neoplastic tissue types were identified. The predominant tissue type was composed of cuboidal to columnar epithelial cells, approximately 15–20 µm in diameter, arranged into solid nests, cords, and follicles in a fine fibrovascular stoma. Follicles were often filled with an eosinophilic, homogenous material (colloid). Neoplastic cells had indistinct borders with moderate amounts of eosinophilic foamy or vacuolated cytoplasm. Nuclei were centrally located, approximately 5–8 µm in diameter, contained finely stippled chromatin, and often contained a single basophilic nucleolus (Fig. 3). There was moderate anisocytosis and anisokaryosis. Three mitotic figures were counted per 10 40× microscopic fields. Immunohistochemistry was performed for thyroglobulin, calcitonin, and chromogranin A using normal canine thyroid gland as a positive control tissue. For each immunohistochemical reaction, the appropriate cell type in the control tissue was strongly and specifically stained. In the neoplastic tissue, thyroglobulin was expressed in the colloid, with strong cytoplasmic reactivity in neoplastic cells that bordered the colloid-filled follicles, and variable cytoplasmic reactivity in cells in the solid areas between follicles (Fig. 4). Calcitonin and chromogranin A immunoreactivity was uniformly negative throughout the tumor tissue. The immunohistochemical results confirmed the neoplastic cell origin to be thyroid follicular epithelium.
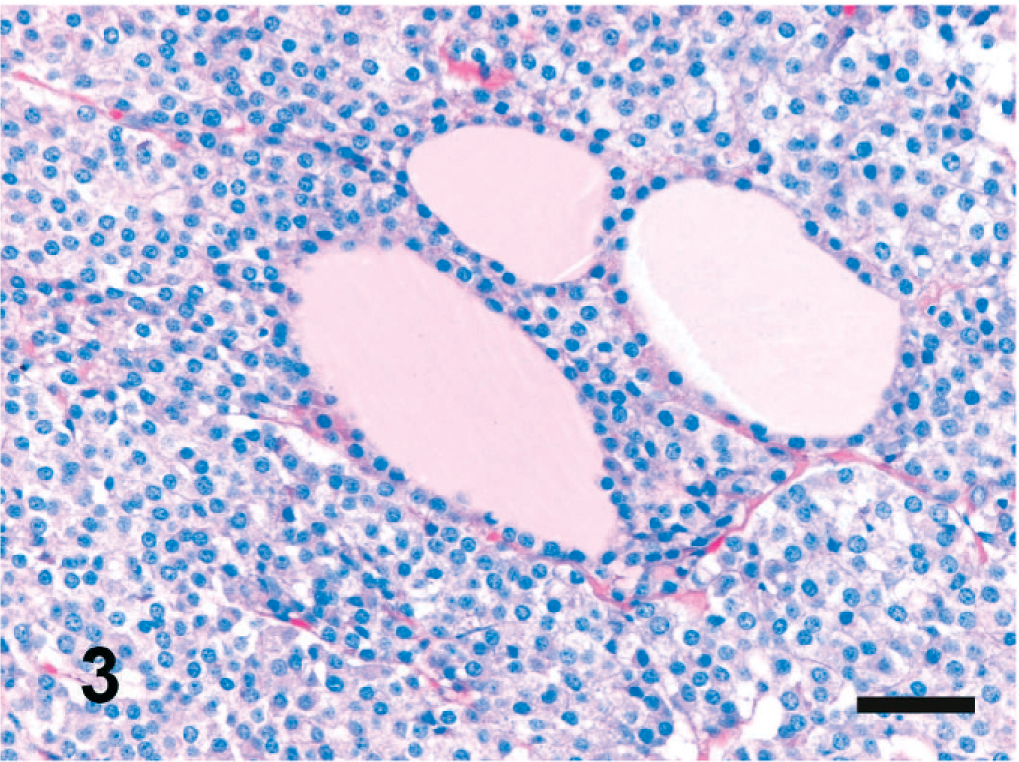
Intracardiac thyroid carcinosarcoma; dog. Neoplastic thyroid tissue composed of solid nests of epithelial cells and colloid-filled follicles in a fine fibrovascular stroma. HE. Bar = 50 µm.
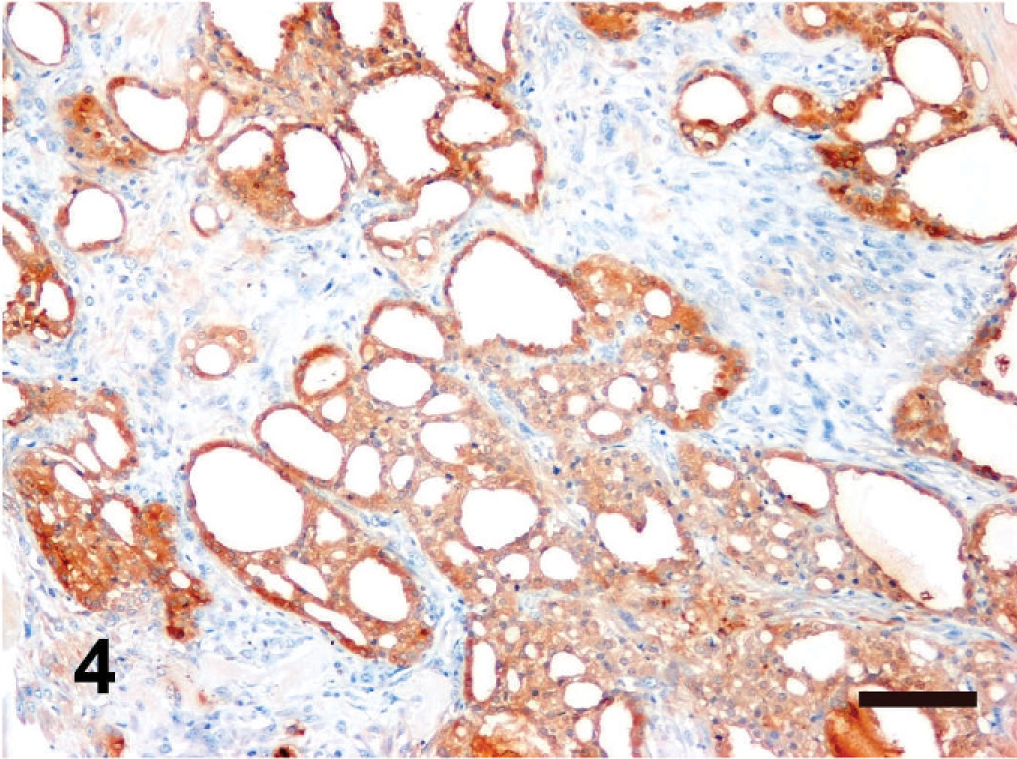
Intracardiac thyroid carcinosarcoma; dog. Neoplastic cells lining follicles have strong cytoplasmic immunohistochemical expression of thyroglobulin, with slightly less intense cytoplasmic reactivity in cells in solid areas between follicles. Immunohistochemically negative spindle cells between follicles are cells of the sarcomatous component of the carcinosarcoma. Immunoreactive colloid is also present (lower and lower right). Antithyroglobulin immunohistochemistry, DAB chromogen, hematoxylin counterstain. Bar = 100 µm.
The second tissue type was composed of interlacing bundles and streams of spindyloid to stellate cells that surrounded islands, trabeculae, or spicules of tumor osteoid (Fig. 5). These cells had indistinct cell borders, scanty eosinophilic fibrillar cytoplasm, and elongate to oval, paracentral nuclei with vesicular chromatin and a single nucleolus. Multifocally rimming the osteoid were multinucleated cells with up to 25 nuclei with coarsely stippled chromatin. These cells ranged from 40–120 µm in diameter and had lightly basophilic homogeneous cytoplasm. There was marked anisocytosis and anisokaryosis. One mitotic figure was counted per 10 40× microscopic fields. Multiple areas of mineralization were present. Small areas of hemorrhage and necrosis were scattered throughout the neoplasm. Neoplastic thyroid tissue and neoplastic bone tissue were frequently intermixed (Fig. 6).
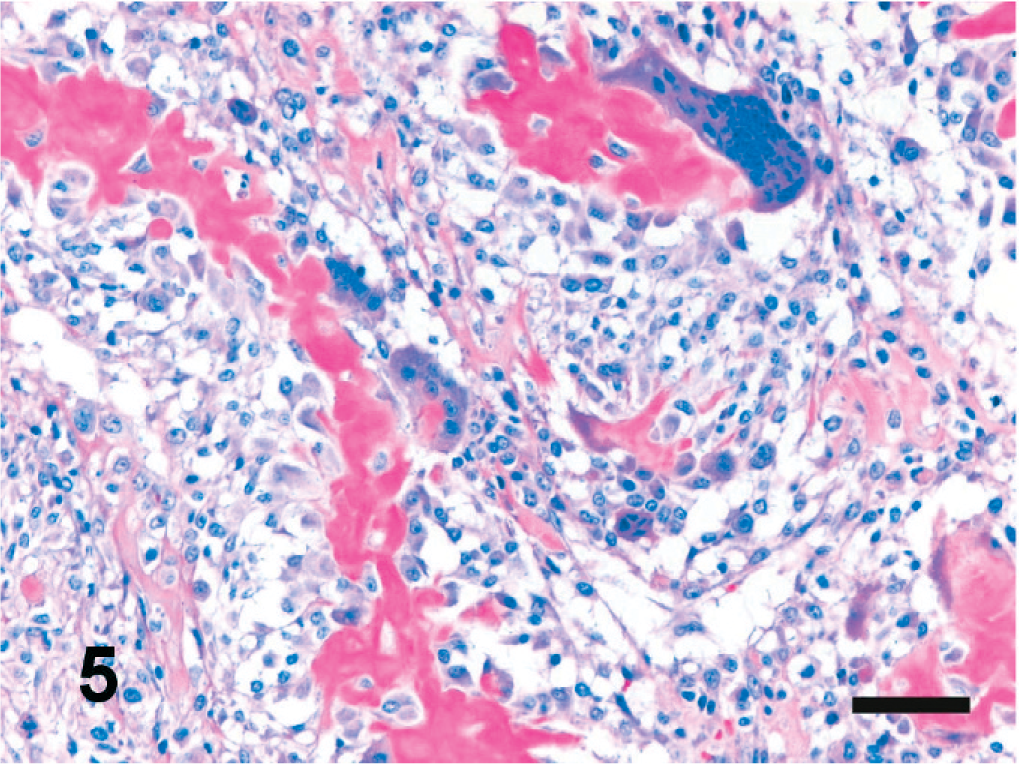
Intracardiac thyroid carcinosarcoma; dog. Pleomorphic spindloid to stellate cells surround islands of tumor osteoid. Multinucleated cells up to 120 µm in diameter are multifocally adjacent to the osteoid. HE. Bar = 50 µm.
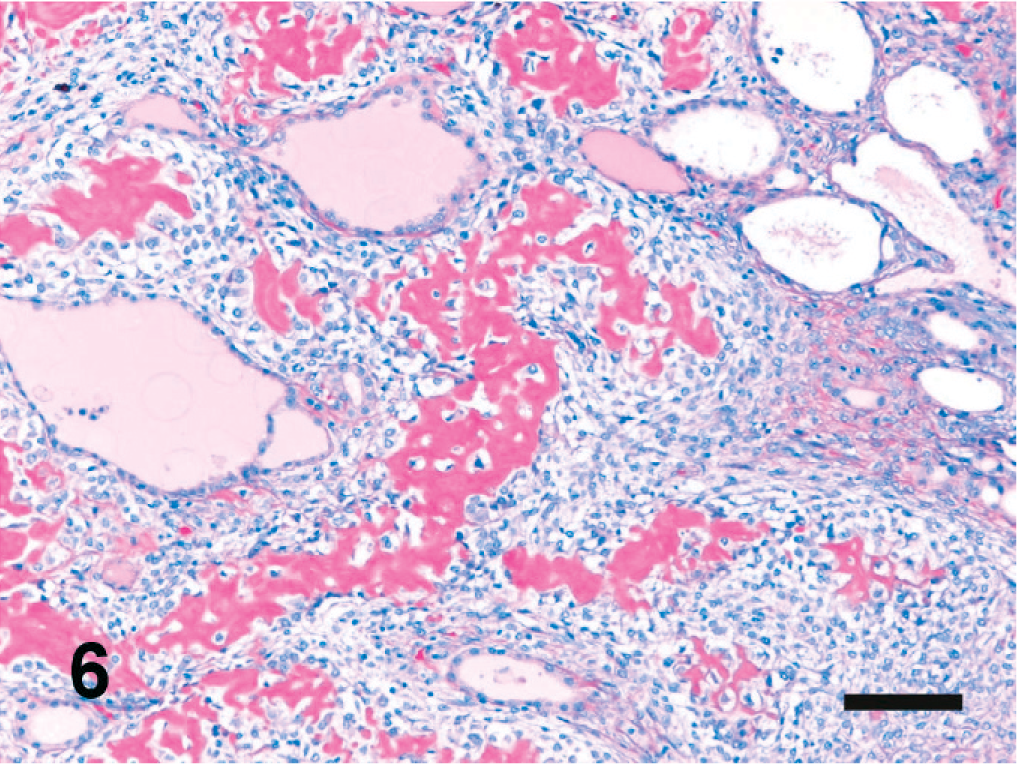
Intracardiac thyroid carcinosarcoma; dog. Neoplastic bony tissue admixed with neoplastic thyroid tissue. HE. Bar = 100 µm.
A small portion of the tumor was made up of a third tissue type composed of neoplastic cells arranged in blood-filled vascular channels, clefts, and caverns on a coarse fibrovascular stroma. Cells were pleomorphic, spindloid to stellate, with indistinct cell borders and scanty eosinophilic fibrillar cytoplasm. Nuclei were elongate, centrally located, and contained finely stippled chromatin (Fig. 7). Sixteen mitotic figures were counted per 10 40× microscopic fields. Numerous hemosiderophages were present throughout this area of the neoplasm. The neoplastic cells lining the blood-filled channels were immunohistochemically positive for factor VIII–related antigen confirming their endothelial cell origin (Fig. 8).
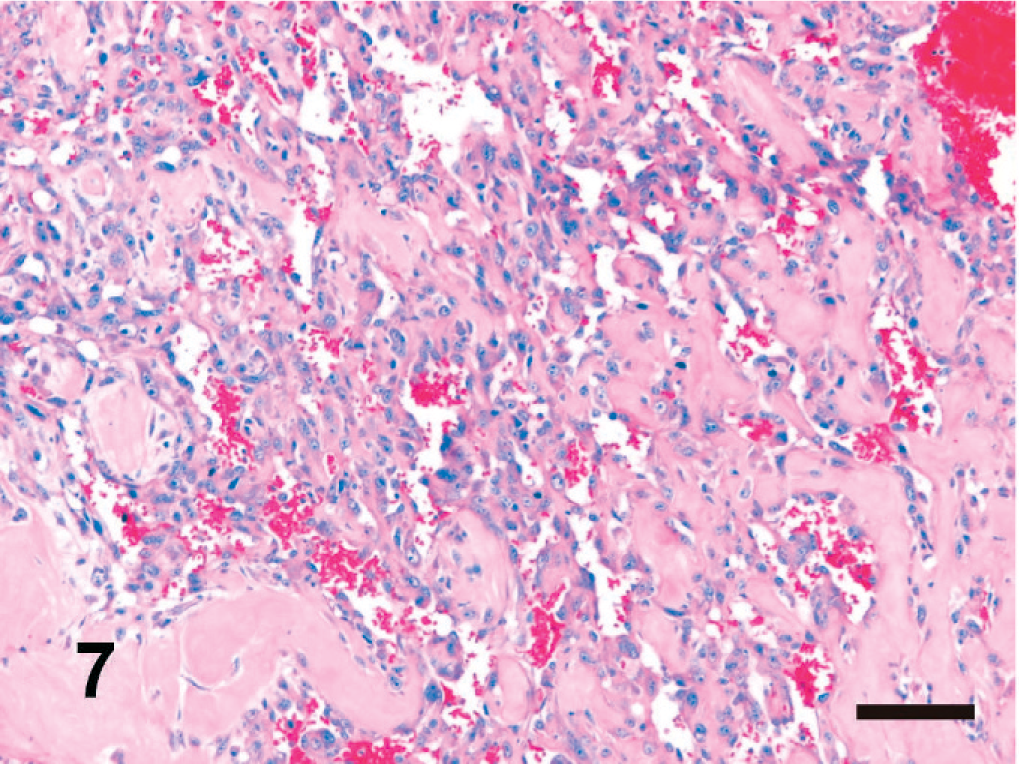
Intracardiac thyroid carcinosarcoma; dog. Neoplastic endothelial cells loosely arranged into blood-filled vascular channels, clefts, and caverns. HE. Bar = 100 µm.
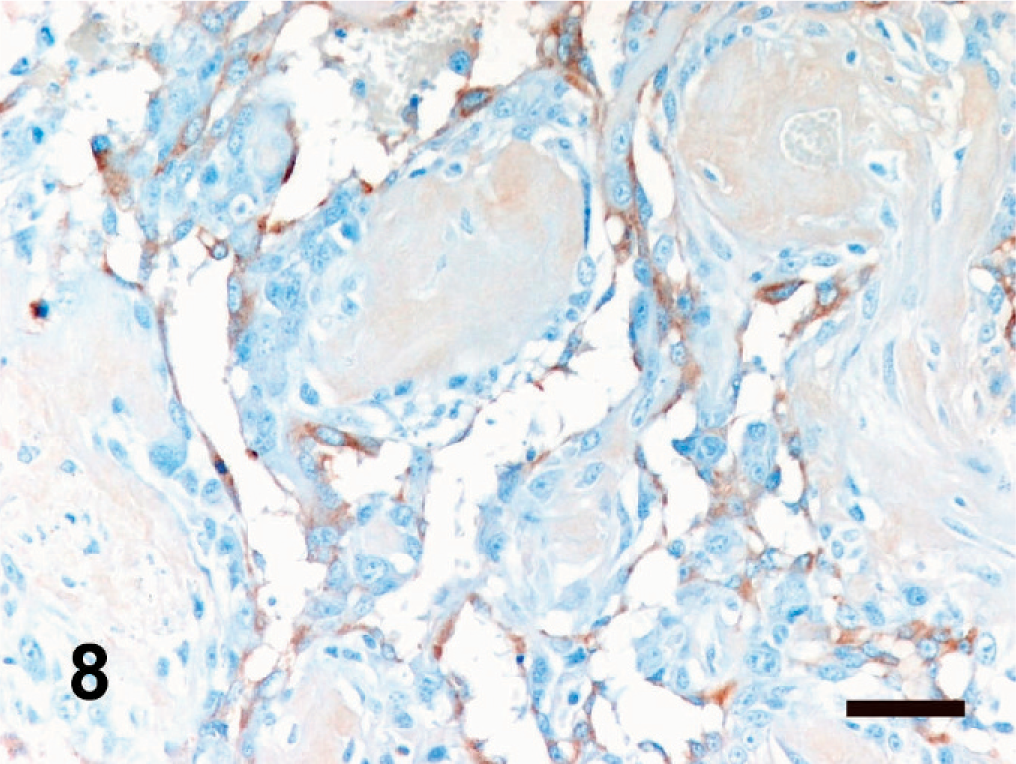
Intracardiac thyroid carcinosarcoma; dog. Positive immunohistochemical reaction of neoplastic endothelial cells with antibody to factor VIII-related antigen. DAB chromogen, hematoxylin counterstain. Bar = 50 µm.
Based on the cell/tissue morphology and immunohistochemistry, the histologic diagnosis was intracardiac ectopic thyroid carcinosarcoma. The neoplastic thyroid tissue provided the carcinomatous portion, and the osteosarcoma and hemangiosarcoma contributed the sarcomatous components. The thyroid gland was in its normal anatomic position and was histologically normal, ruling out the possibility that the intracardiac tumor was metastatic from a primary thyroid neoplasm. No metastases were found in the other visceral organs.
Ectopic thyroid tissue has been documented from the tongue to the diaphragm in domestic animals, with the ventral wall of the pharynx, base of the tongue, heart base, and the region of the thyroglossal duct all reported. 5, 6, 14 In the canine embryo, the thyroid gland develops from a thickened plate of endodermal epithelium in the floor of the pharynx. This occurs on midline at the level of the first pharyngeal pouch and the dorsolaterally migrating tissue is anchored to the pharyngeal area by the thyroglossal duct. This migrating tissue is intimately associated with the aortic sac during its development, which results in frequent remnants of ectopic thyroid parenchyma in the mediastinum and associated tissues. 6 This association and prolonged contact with the developing myocardium may seed thyroid epithelium into what will later become the interventricular septum, giving rise to intracardiac ectopic thyroid tissue. 22 This is supported by the majority of intracardiac ectopic thyroid tissue being located on the interventricular septum within the right ventricle. 8 Although it is considered rare, multiple cases of intracardiac ectopic thyroid tissue have been reported in humans. 8, 21, 22 Ectopic thyroid tissue has also been reported in the adrenal gland of a 50-year-old woman 24 and in a branchial cyst in a 36-year-old woman. 12 A small number of these cases have involved neoplastic transformation of this ectopic tissue.
Neoplastic ectopic thyroid tissue has been documented in the dog: in the previously mentioned case of intracardiac thyroid carcinoma 3 and in multiple cases located in the more common location at the heart base. A tumor with a similar echocardiographic appearance to the mass in this case report consisted of functional ectopic thyroid tissue based on thyroid levels and nuclear scintigraphy. 19 Two heart-base tumors were classified as carcinomas 9, 25 and a third was classified by its immunohistochemical profile as positive for thyroglobulin and neuron-specific enolase, and negative for calcitonin. 15
Thyroid carcinosarcomas have only been reported in the normal anatomic location of the thyroid gland in dogs and humans. Five cases have been reported in the dog, 4, 13, 16, 18, 27 with the most recent described by Grubor and Haynes, with a review of the previously reported cases. Human cases are also rare and typically have an aggressive disease course. 1, 10, 11 The dog in this case report is believed to be the first reported case of ectopic thyroid carcinosarcoma in the heart or any other location, in any species.