
Abstract
An adult male mixed breed dog developed pain, on swallowing, that lasted for 1 week. Physical exam and radiographs revealed a subcutaneous mass in the cervical area and three metastatic nodules in the lung. The cervical mass was surgically removed and fixed in 10% buffered formalin. Histopathologic diagnosis was carcinosarcoma supported by positive immunohistochemistry (IHC) results for cytokeratin and vimentin. IHC for thyroglobulin proved that the tissue of origin was the thyroid gland. This is the fifth canine case of thyroid carcinosarcoma to be documented, but the first one to be confirmed by specific cell markers. It is an extremely rare neoplasm that also occurs in people.
Diseases of the thyroid gland include developmental disturbances, degenerative changes, inflammation, hyperplasia, and neoplasia. 4 , 17 Neoplastic masses encountered in the thyroid gland of humans and domestic animals can be derived from thyroid follicular cells, thyroglossal duct remnants, thyroid C cells (parafollicular cells), or chief (parathyroid) cells. 5 Tumors of thyroid follicular cells in domestic animals (especially dogs, cats, and horses) are classified as adenomas or carcinomas, and there are many subtypes based on histologic and behavioral characteristics. The major types of adenomas are follicular and papillary, whereas their malignant counterparts include follicular, papillary, compact cellular (solid), undifferentiated thyroid (small or giant cell) carcinoma, and malignant mixed thyroid tumor (carcinosarcoma). Canine thyroid carcinomas occur more frequently than adenomas, and there is no sex prevalence as that occurring in humans. Furthermore, thyroglossal duct remnants can form carcinomas and are found in dogs, whereas C cell tumors, most frequently found in adult to aged bulls, certain strains of laboratory rats, and adult to aged horses, are divided into adenomas and carcinomas. Finally, adenomas and adenocarcinomas of parathyroid glands are infrequently reported in older dogs, cats, laboratory rats, and mice.
Thyroid carcinosarcomas of dogs are uncommon malignant tumors, which consist of both malignant epithelial (follicular cells) and mesenchymal (usually osteogenic or cartilaginous or both) elements. 5 Other reported sites where primary carcinosarcomas may arise in dogs are mammary gland, 2 , 13 lung, 18 salivary gland, 16 ceruminous gland, 15 and eyelid. 10 In addition, metastasis of mammary carcinosarcoma to distant cutaneous sites, 9 a pulmonary carcinosarcoma to bronchial lymph nodes, kidney, and liver, 18 and a carcinosarcoma of uncertain origin to lumbosacral bone and soft tissue 14 have also been reported. The mammary carcinosarcoma is uncommon in the dog, 13 whereas all other above-mentioned tumors are very rare and usually only one or a few case reports can be found in the literature. 10 , 15 , 16 , 18
To our knowledge, only four cases of canine thyroid carcinosarcomas have been reported (Table 1). 3 , 11 , 12 , 20 In human medicine, carcinosarcoma of the thyroid gland is extremely rare and occurs predominantly in elderly women. 6 , 8 This tumor is believed to arise through the process of neoplastic metaplasia. 1 , 8 Similar to their human counterparts, canine tumors appear to be locally invasive, to be very aggressive, and to metastasize readily. 1 , 11
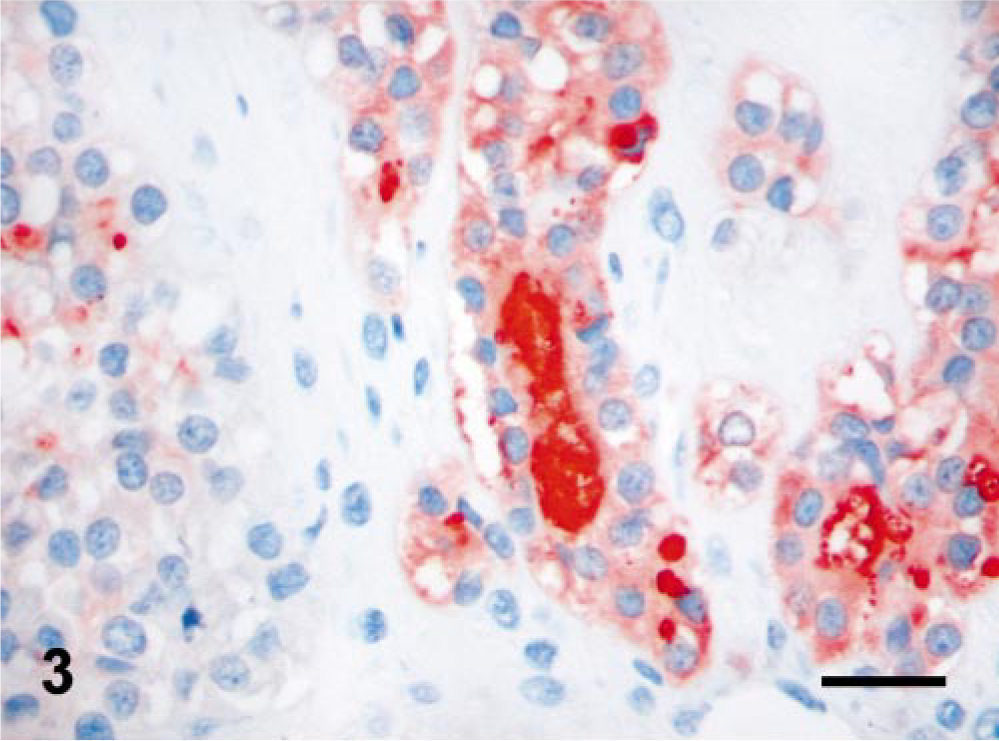
Carcinosarcoma of the thyroid gland in dogs: summary of reported cases.
∗ Multifocal myxedema in the dermis.
† S, sarcomatous elements of the tumor; C, carcinomatous elements; S/C, both sarcomatous and carcinomatous elements; N, not known.
A 14-year-old male mixed breed dog developed pain, on swallowing, that lasted for 1 week. Complete blood count and chemistry results were normal. Radiographs revealed a mass in the cervical area, and fine needle aspirate showed malignant neoplasia of unknown origin. Three metastatic nodules were present in the lung. The mass from the cervical region was excised surgically. It was a subcutaneous mass, fixed in a position because of its attachment to the esophageal wall (paraesophageal location), tan-white in color, firm, about 5 × 3 × 3 cm, well encapsulated, and contained dark liquefied material on the cut surface. After surgical excision, the animal received chemotherapy (doxorubicin, i.v.). After 3 months, the dog was euthanatized because of several systemic problems (persistent fever of unknown origin, neutrophilia, hypoalbuminemia, protein losing nephropathy, hepatomegaly) and enlargement of the pulmonary metastatic sites; however, the dog was not necropsied.
Tissue samples for light microscopy were fixed overnight in 10% neutral buffered formalin, paraffin embedded, and stained with hematoxylin and eosin (HE). Selected 3-µm histologic sections were stained with alcian blue or by standard streptavidin–biotin–immunoperoxidase method with the following primary antibodies: monoclonal mouse anti-human cytokeratin, AE1/AE3 (Dako Corp., Carpinteria, CA), monoclonal mouse anti-vimentin (Dako), polyclonal rabbit anti-human thyroglobulin (Dako), and monoclonal rat anti-human parathyroid hormone (PTH) (Dako). Positive control sections were included for each antibody, whereas a negative control lacked primary antibody.
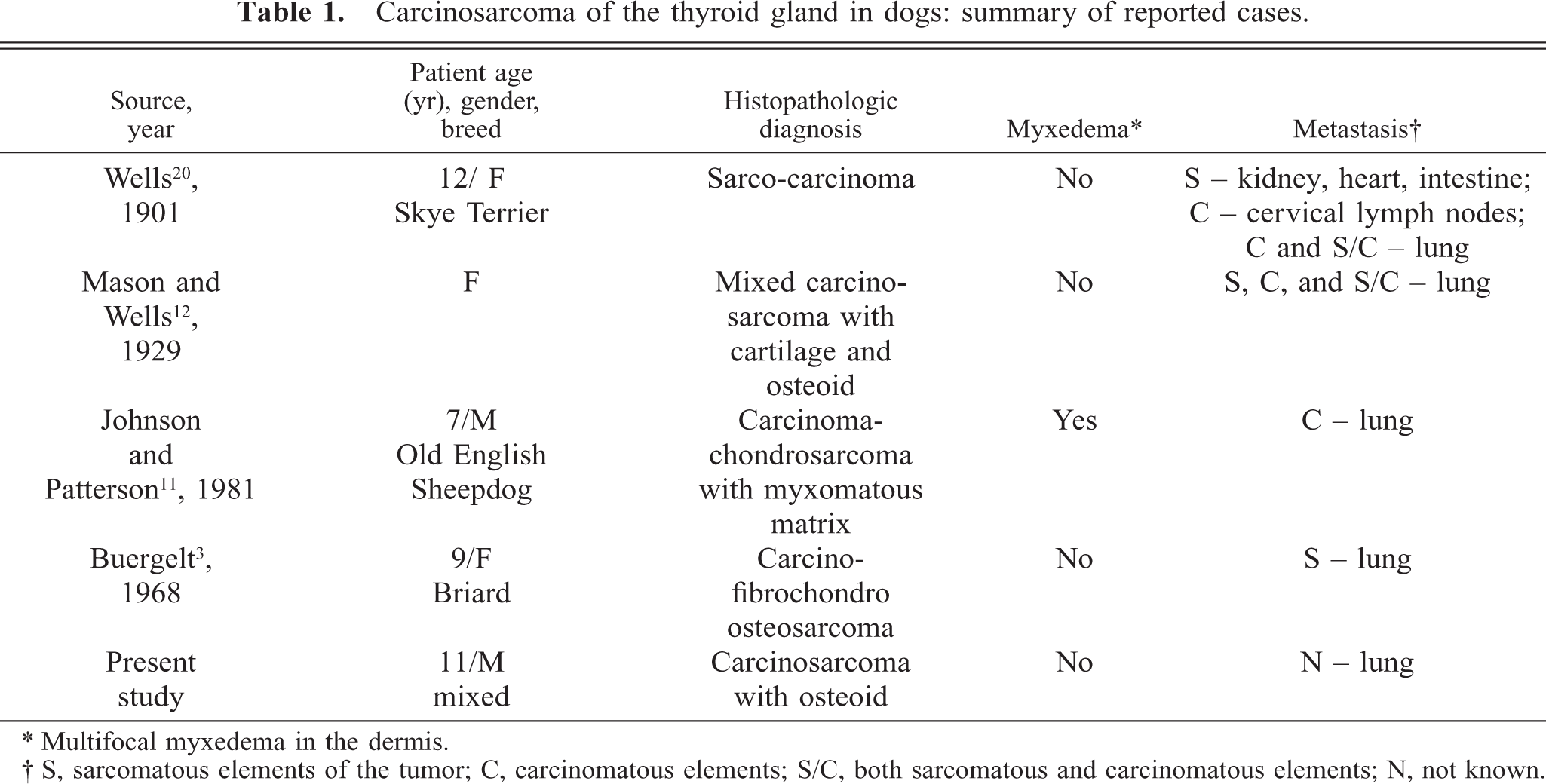
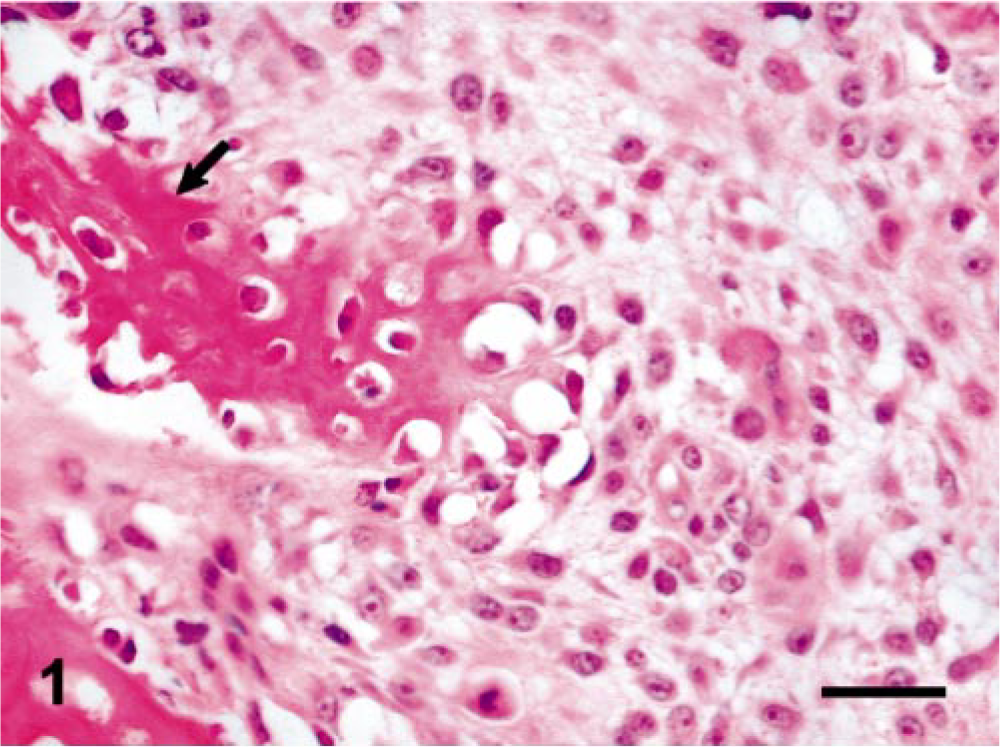
Histopathology showed thyroid gland with partially encapsulated and moderately well-demarcated mass that occupied about 80–90% of the section and compressed thyroid gland parenchyma. The mass was composed of two cell types, the first one being arranged in sheets or intersecting bundles supported by collagenous stroma. In other areas, these neoplastic cells were aligned along small, thin or globular, poorly calcified trabeculae of osteoid (Fig. 1). The cells were oval to spindle shaped, about 25–35 µm in diameter, and had discernable cell boundaries and moderate amount of lightly eosinophilic, fibrillar, and often vacuolated cytoplasm. The nuclei were round to oval, about 15–25 µm in diameter, and had stippled chromatin and one to four prominent nucleoli. There was a high mitotic rate (2–3 mitoses/40× field). The second cell type formed irregular follicular structures or nests, supported by delicate fibrovascular stroma (Fig. 2). These cells were cuboidal to irregular, about 20–25 µm in diameter, and had poorly defined cell borders and finely granulated cytoplasm. The nuclei were round, usually 10–15 µm in diameter, with some of them being bizarre shaped and up to 25 µm in diameter, and had a moderate mitotic rate (approximately 1 mitosis/40 × field). The follicles varied from well differentiated with lightly eosinophilic, homogenous, globular material (colloid) to undifferentiated without discernible lumina. Some of them also contained intraluminal cellular debris, degenerate neutrophils, and macrophages. In addition, there were multiple areas of necrosis, accumulation of seroproteinaceous material, fibrin, blood, golden/brown granular pigment (hemosiderin), and infiltrates of lymphocytes and plasma cells within the mass. Surgical clearance appeared incomplete.
Thyroid gland mass; dog. This portion of the mass is composed of spindle-shaped neoplastic cells lining and interspersed between irregular trabeculae of osteoid (arrow). HE. Bar = 50 µm.
Thyroid gland mass; dog. This area of the mass consists of irregular follicular structures (arrow) supported by delicate fibrovascular stroma. HE. Bar = 50 µm.
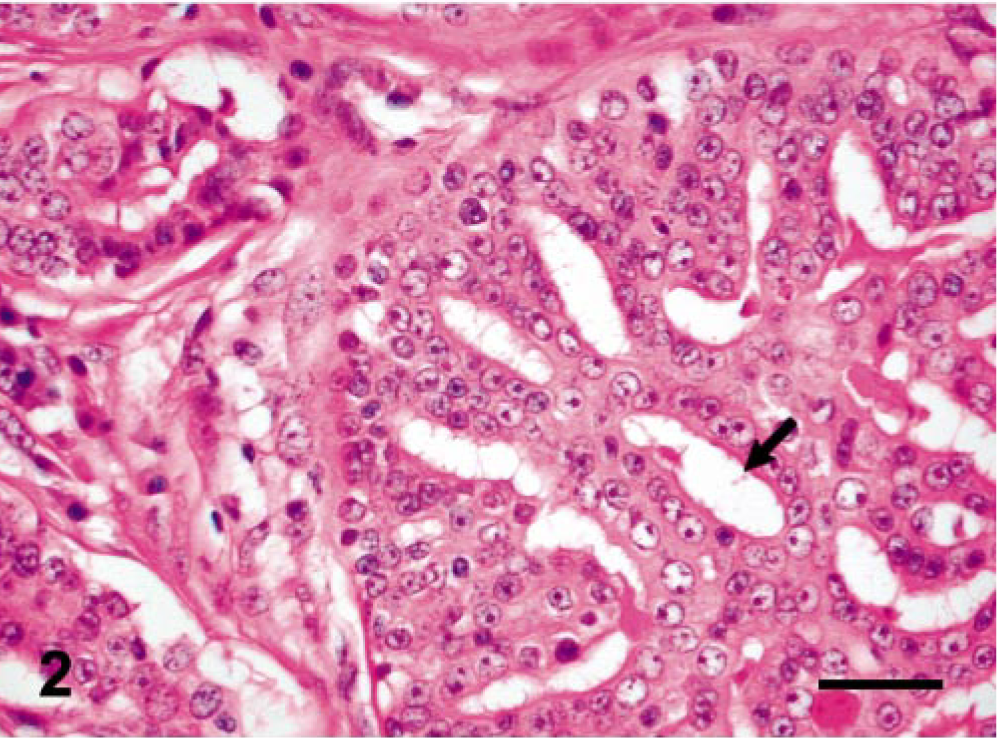
Immunohistochemistry (IHC) results for vimentin and cytokeratin confirmed the presence of two cell types. The mesenchymal cells were strongly positive for vimentin where approximately 50–60% of spindle-shaped neoplastic cells were stained. On the other hand, the majority of neoplastic glandular structures were strongly positive for cytokeratin. The origin of neoplastic cells was revealed by IHC results for thyroglobulin (Fig. 3). Thyroid parenchyma at the periphery of the mass (internal control) and the neoplastic follicular structures within the mass were strongly positive for thyroglobulin. Negative results for PTH helped us rule out the possibility of parathyroid gland origin of the tumor. In addition, alcian blue special stain results were negative showing the absence of glycosaminoglycan-rich ground substance.
Thyroid gland mass; dog. The epithelial cells that form neoplastic follicular structures and material within the lumen stain positive for thyroglobulin (red color). IHC for thyroglobulin with hematoxylin counterstaining. Bar = 50 µm.
At the beginning, the tissue of origin was not clear, and we suspected that it could have been thyroid or parathyroid gland. Salivary gland was another possibility because osteoid production had been reported in the malignant mixed tumor and extraskeletal osteosarcoma of the salivary gland. 16 , 19 The IHC results for thyroglobulin confirmed the presence of neoplastic thyroid follicular cells, which were intermixed with vimentin-positive neoplastic mesenchymal cells. One of the previously reported cases of mixed thyroid tumors in dogs was associated with myxedema, 11 whereas the other three did not have any record on this issue. 3 , 12 , 20 In this dog, similar to human thyroid carcinomas, 7 the tumor did not influence thyroid function and myxedema was not observed (Table 1).
In general, accumulated material or multiple tissue types can be found in the thyroid gland parenchyma during several disease processes. 17 Degeneration of the thyroid gland may be accompanied by the accumulation of corpora amylacea–like bodies, mineralized colloid, lipofuscin, or amyloid that is a part of systemic disease or appears as a localized primary amyloid tumor (“amyloid goiter”). Squamous cells can be found because of presence of thyroglossal duct or branchial pouch–derived structures or because of squamous metaplasia in Hashimoto thyroiditis or papillary carcinoma. Teratomas, which usually occur in infants or children, contain islands of well-differentiated cartilage, whereas undifferentiated carcinomas may exhibit cartilaginous/osseous metaplasia. In addition, extramedullary hematopoiesis has been reported in a case of myelofibrosis.
The thyroid mass found in this dog is a very unusual malignant neoplasm that is composed of both carcinoma and sarcoma with osseous elements, hence the diagnosis of carcinosarcoma. According to a classification system developed by Benjamin et al., the term “carcinosarcoma” is restricted to canine malignant mammary gland tumors with two clearly malignant components, one epithelial or myoepithelial and one mesenchymal, whereas the term “malignant mixed mammary gland tumor” is used for carcinomas or sarcomas in a mixed tumor. 2 The histogenesis of mammary gland carcinosarcoma is still unclear; however, it is believed that carcinosarcoma might arise from a mixed tumor. 2 In addition, the metastatic rate for the true carcinosarcomas, compared with the adenocarcinoma in mixed tumors, is much higher suggesting that this classification may be of prognostic value as well.
The animals with thyroid tumors are usually adult or aged, the mean age of dogs with thyroid carcinoma being 9 years. 5 Thyroid carcinomas often grow rapidly and invade adjacent structures such as the trachea, esophagus, and larynx. 5 Lung is the earliest and most frequent site of metastasis for thyroid carcinomas because these tumors tend to invade branches of the thyroid vein. Similar behavior has been observed for thyroid carcinosarcoma, where pure carcinomatous or sarcomatous or both elements metastasize (Table 1). 3 , 11 , 12 , 20 On the basis of these facts as well as on the presence of metastatic nodules in the lung and other features of malignancy noticed within both epithelial and mesenchymal components of the primary neoplasm, we believe that the long-term prognosis for thyroid carcinosarcoma in dogs is guarded to poor, which is supported by other studies. 3
Footnotes
Acknowledgements
We are grateful to Dr. Mark R. Ackermann for helpful suggestions and Elise L. Huffman for excellent technical assistance.