
Abstract
A primary intimal aortic angiosarcoma was diagnosed in a 4-year-old, spayed female German Shepherd that presented for complications of thromboembolic disease because of infarcts in multiple organs. On gross examination, aneurysmal dilatation of the aorta was associated with a friable, necrotic mass attached to the endothelial surface, which partially occluded the aortic lumen. On histologic examination, plump neoplastic spindle cells formed a plaque-like mass arising from the intima that merged with a large accumulation of fibrin and necrotic debris, and projected into the lumen. Neoplastic cells invaded periaortic vessels and were seen in some infarct-associated thromboemboli. Tumor cells expressed vimentin and CD31, with infrequent, patchy staining with factor VIII-related antigen; tumor cells were negative for cytokeratin and smooth-muscle actin. Aortic angiosarcoma is a rare malignancy in humans. This is the first description of a primary intimal aortic angiosarcoma in a dog, with immunohistochemical evidence of endothelial origin.
Primary sarcomas of the great vessels are reported rarely in humans, with most cases arising in the aorta. 8 Arterial thromboembolism often causes ischemic lesions of abdominal organs and metastatic spread. 7, 9, 10 Immunohistochemistry most commonly reveals evidence of myofibroblastic origin, although only a subset exhibits evidence of endothelial origin, with immunoreactivity for CD31, factor VIII-related antigen, or other endothelial antigens; these tumors are classified as “angiosarcoma.” 2, 5, 7, 8, 10 Primary tumors of the great vessels are rare in dogs, with only a few well-characterized case reports in the literature, including primary aortic chondrosarcoma and pulmonary arterial leiomyosarcoma. 1, 3, 4 To our knowledge, there are no reports of a malignant primary aortic sarcoma of endothelial origin in dogs. This report describes the clinical, histologic, and immunocytochemical features of a primary aortic angiosarcoma in an adult dog.
A 4-year-old, spayed female German Shepherd was presented to the North Carolina State University Veterinary Teaching Hospital for persistent vomiting, nausea, and anorexia. Approximately 3 days before presentation, the dog had been evaluated by the referring veterinarian for complaints of depression, dehydration, anorexia, and vomiting. Visualization of distended, gas-filled loops of intestine on radiographs prompted an exploratory laparotomy. A nonperforated segment of jejunum that contains multiple foci of necrosis and a dark purple hemorrhagic left kidney were resected. After surgery, clinical signs continued. The medical history of the dog included surgical correction of a patent ductus arteriosus as a puppy.
On physical examination, the dog was depressed but in good body condition. Heart rate and respirations were normal. As the case progressed, complete blood count and serum chemistry findings included a packed cell volume of 18% (reference range, 33–58%), and renal azotemia, with blood urea nitrogen of 33 mg/dl (reference range, 8–27 mg/dl) and creatinine of 3.4 mg/dl (reference range 0.5–1.6 mg/dl), and isosthenuria on urinalysis. On an echocardiogram, there was prominent dilatation of the proximal aorta and moderate aortic valve insufficiency. Despite intravenous fluid therapy, antibiotics, antiemetics, and nutritional support over a period of 2 weeks, profuse vomiting continued, terminal seizures developed, and the dog was euthanatized.
A gross necropsy revealed a firm, 3.5 × 3.0 × 1.5 cm, aneurysmal dilatation and mural thickening of the distal aortic arch, just distal to origin of the left subclavian artery. A mass of friable, gray-yellow-green necrotic material partially occluded the aortic lumen and was adherent to the endothelial surface (Fig. 1). The right kidney was distorted by massive subcapsular hemorrhage, up to 3-cm thick, with prominent compression of the subjacent renal parenchyma. Multiple 2- to 4-mm pale foci of necrosis were scattered in the renal cortex, and a 1-cm hemorrhagic focus was located in the ventral parenchyma. Multifocal infarcts involved approximately 40% to 50% of the spleen. Representative tissue samples were fixed in 10% neutral buffered formalin, processed, and embedded in paraffin according to routine histologic techniques. Sections, 5-μm thick, were stained with hematoxylin and eosin for microscopic examination.

Aorta, distal aortic arch, luminal surface; 4-year-old spayed female dog. The aortic lumen is segmentally dilated and partially occluded by an irregular mass (asterisk) of friable, necrotic material adherent to the intimal surface (arrow).
On histologic examination, neoplastic cells varied from round to ovoid to plump spindloid and formed a plaque-like mass that arose from the intima that merged with a large accumulation of fibrin and necrotic debris, and projected into the lumen (Fig. 2). Tumor cells also occasionally infiltrated into the tunica media. Tumor cells contained small amounts of amphophilic cytoplasm and round-to-oval, vesiculate nuclei with 1 to 2 magenta nucleoli. Anisocytosis and anisokaryosis were prominent, and mitoses were moderately frequent. Arteries in multiple systemic sites, including the aortic adventitia, kidney, and lung were occluded by similar pleomorphic cells. Multifocal acute renal infarcts contrasted with chronic changes, including tracts of interstitial fibrosis, degenerative glomerular changes, and foci of mineralization. Thrombosis affected several lymph nodes, gastric submucosal vessels, and a carotid artery. Histology of the right kidney obtained after nephrectomy contained intravascular tumor emboli, and both this kidney and the resected intestine contained multifocal infarcts.
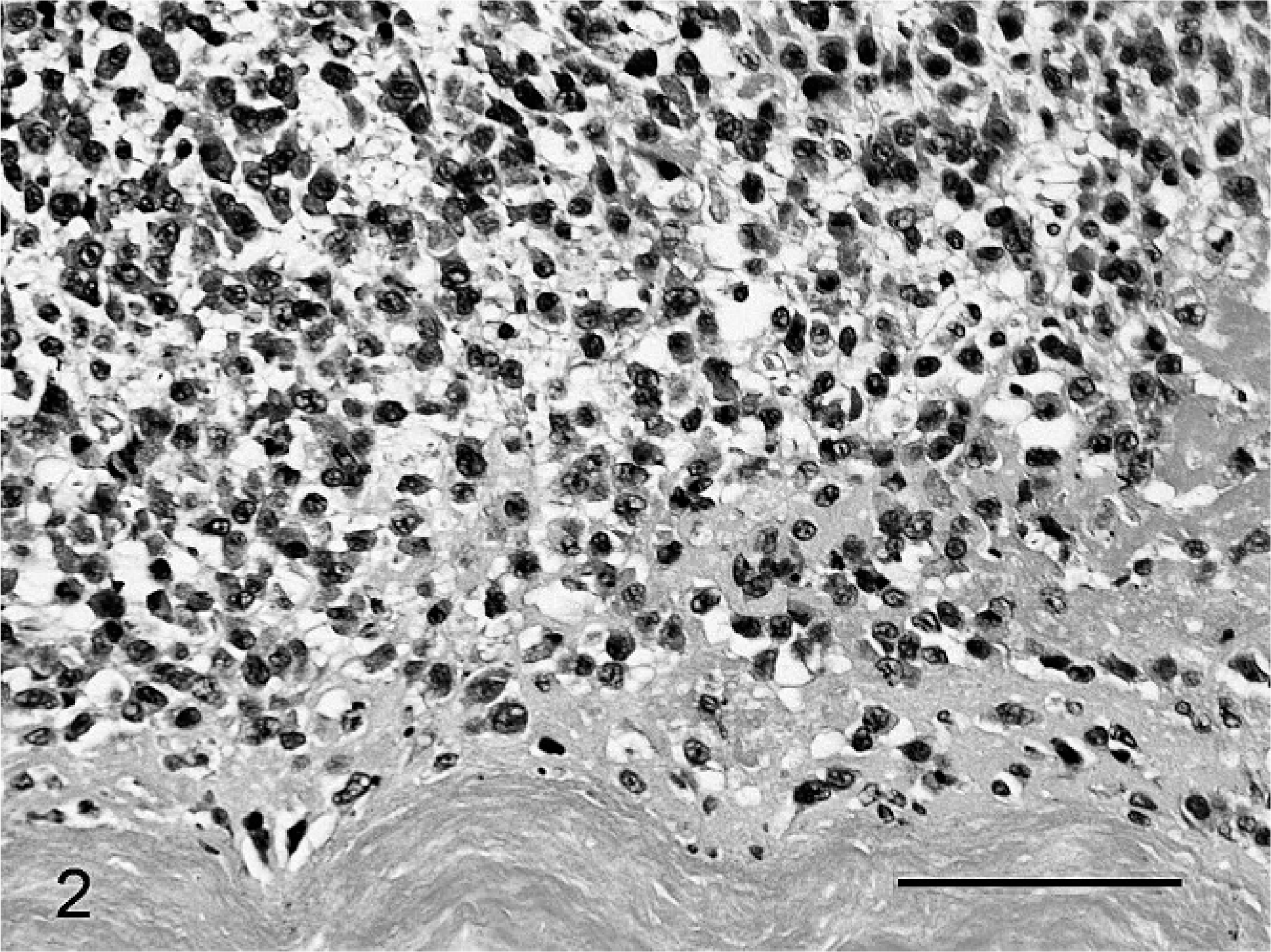
Aortic mass; 4-year-old spayed female dog. The aortic luminal mass was composed of plump round to ovoid, sometimes spindloid neoplastic cells, fibrin, and necrotic debris arising from the tunica intima. HE. Bar = 100 μm.
Unstained, paraffin-embedded sections of the aortic mass were processed routinely for streptavidin-biotin peroxidase immunohistochemical evaluation for cytokeratin and vimentin (Ventana, Tucson, AZ), alpha smooth-muscle actin (Biogenex, San Ramon, CA), and factor VIII and CD31 (Dako, Carpinteria, CA). Tumor cells exhibited strong, diffuse cytoplasmic immunoreactivity for vimentin but failed to exhibit staining for cytokeratin. Approximately 75% to 80% of these cells also had moderate-to-strong membranous immunoreactivity for CD31 (Fig. 3). The majority of tumor cells were negative for factor VIII, with only a few small clusters of cells exhibiting mild positive staining; small vessels that served as internal positive controls exhibited strong immunostaining for factor VIII. Tumor cells were negative for smooth-muscle actin. Intra-arterial aggregates of neoplastic cells within the kidney and aortic adventitial vessels exhibit the same immunohistochemical staining as the aortic mass.
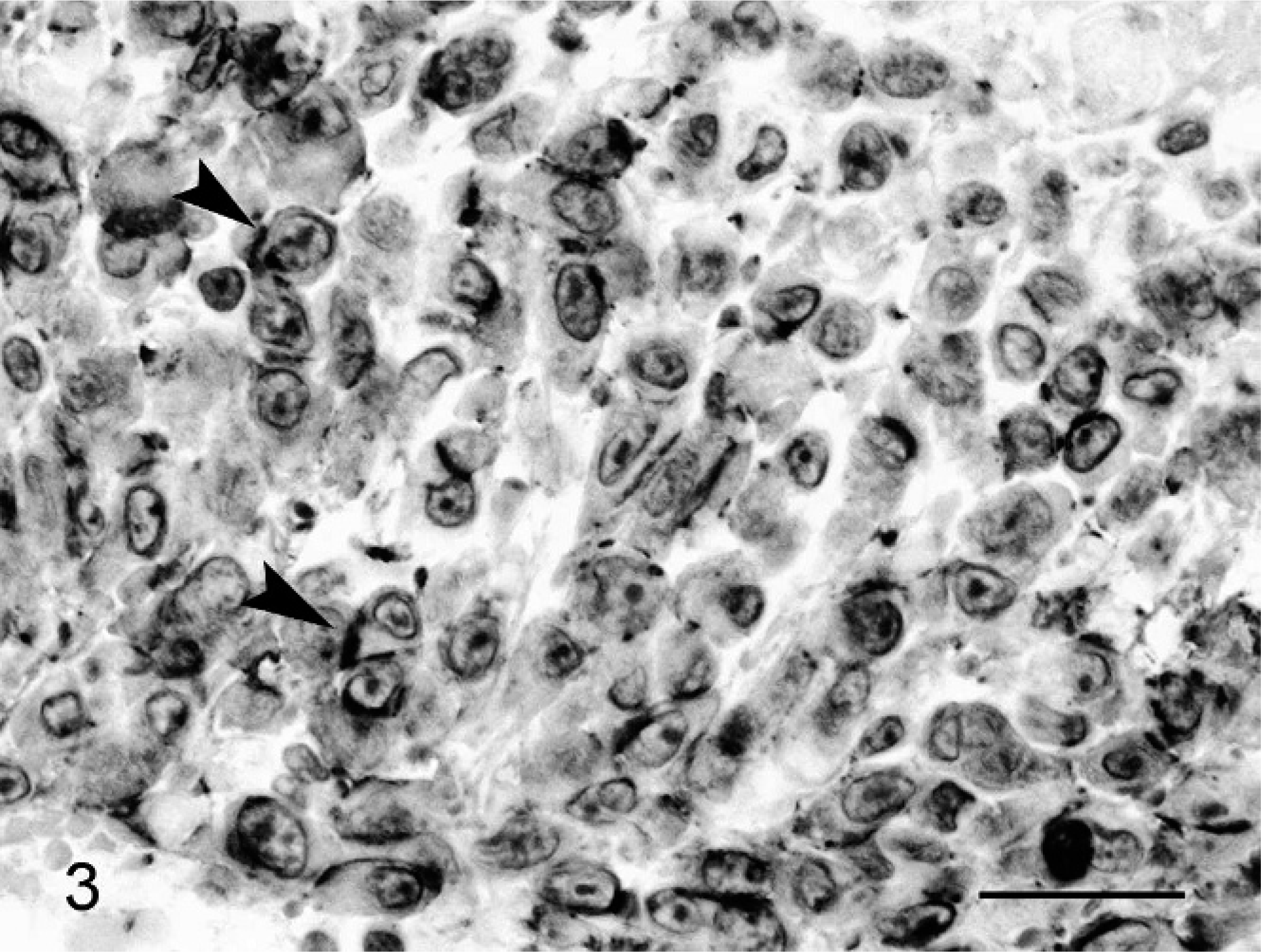
Aortic mass; 4-year-old spayed female dog. Neoplastic cells exhibit membranous immunoreactivity for CD31, often most apparent at cellular junctions (arrowheads). Streptavidin-biotin peroxidase, Mayer's hematoxylin counterstain. Bar = 25 μm.
The present case bears multiple similarities to cases of aortic intimal angiosarcomas described in humans, which are clinically aggressive, frequently poorly differentiated neoplasms that appear as thrombi composed of necrotic debris and tumor cells within the lumen and adherent to the intima, and are characterized by tumor growth along the intimal surface, aneurysmal vascular dilatation, and expression of endothelial markers. 2, 8 Their growth pattern differs from mural sarcomas, which invade the media or adventitia. 2 Although many aortic sarcomas feature evidence of myofibroblastic origin, with immunoreactivity for vimentin and smooth-muscle actin, only aortic angiosarcomas reveal evidence of endothelial origin, such as immunoreactivity for CD31 or factor VIII-related antigen. 2, 5, 7, 8, 10 Clinical findings in humans are variable, reflecting sequela to acute thromboembolic occlusion of visceral or peripheral arteries, such as the multifocal infarcts and widespread metastases. 5, 7, 9, 10 The complications of intestinal and renal infarction present in this dog are similar to several of the reported human cases. In addition to thromboemboli in this dog, there was evidence of intravascular metastasis in the kidney and lung, and extension into periaortic vessels. There was minimal invasion of the aortic tunica media, which is an uncommon feature of human tumors.
In this dog, no other primary tumors were identified on gross or histologic examination, including the predisposed sites for hemangiosarcoma (right atrial appendage, spleen, and liver). The aortic mass and the intra-arterial tumor cell aggregates exhibited strong immunoreactivity for vimentin and CD31, supporting a diagnosis of an endothelial-derived intimal angiosarcoma, as described in the human literature. 5, 7, 8, 10 Although immunopositivity for factor VIII would also be expected in a tumor of endothelial origin, the degree of anaplasia may be contributing to a lack of expression of this antigen. A differential diagnosis considered for the lesion in humans is intravascular metastases of poorly differentiated carcinoma. 5 The lack of a detectable primary carcinoma and the failure to demonstrate immunoreactivity for cytokeratin helped to rule out this possibility.
There are reports in the human literature of primary arterial sarcomas that arise at sites of prosthetic grafts, hypothesized to relate to a foreign-body reaction that lead to endothelial dysplasia and tumor induction. 8 No implant was present in this dog, and the ligation site of the ductus arteriosus lacked gross and histologic changes, including evidence of neoplasia.
Primary tumors of the great vessels in dogs are very rare. Geib 4 described an intraluminal fibrinous thrombus just above the aortic valves in a Boxer, which was classified as a hemangioendothelioma; however, no description of the histopathology was provided. Anderson et al. 1 presented a case of a primary aortic chondrosarcoma in a Lhasa Apso, which partially occluded the aortic lumen, was focally adherent to the tunica media and was composed of well-differentiated cartilaginous cells within a chondroid ground substance. In a recently described case of a leiomyosarcoma that affected the pulmonary artery and pulmonary valve, the tumor expressed vimentin and alpha smooth-muscle actin but was negative for CD 31 and factor VIII. 3 Canine intravascular lymphoma (malignant angioendotheliomatosis) is an angiotropic form of lymphoma reported in dogs, which presents as proliferations of neoplastic lymphocytes, usually within the lumens of small- and medium-sized vessels, rather than the great vessels; this tumor has a predilection for the central nervous system. 6
Given the results of gross necropsy, histology, and immunohistochemistry, we considered the aortic mass to represent a primary endothelial-derived sarcoma of the aortic intima that closely resembles reported cases of aortic intimal angiosarcoma in humans. To the authors' knowledge, this case represents the first documentation of a primary intimal aortic sarcoma with immunohistochemical evidence of endothelial origin in a veterinary species.
Footnotes
Acknowledgements
We thank Sandra Horton, Nathan Whitehurst, and Monica Mattmuller for their technical assistance.