
Abstract
The expression of estrogen receptor-α (ER) and progesterone receptor (PR) in normal, hyperplastic, and neoplastic endometrium in rabbits was evaluated by immunohistochemistry. The tissues evaluated were 27 normal uteri, 19 cases with endometrial hyperplasia, and 42 adenocarcinomas. Sixteen of 27 cases of normal uteri (59.3%) and 13 out of 19 hyperplasias (68.4%) stained positive with both ER-α and PR. Adenocarcinomas were further subdivided into 26 papillary and 16 tubular/solid adenocarcinomas. Papillary adenocarcinoma infiltrated the myometrium late in the disease and caused attenuation of the myometrium. In contrast, tubular/solid adenocarcinoma invaded into the deep myometrium early in the disease without thinning of the myometrium. Twenty-one cases out of 26 (80.8%) cases of papillary adenocarcinoma were both ER-α and PR negative, whereas 15 out of 16 (93.8%) of the tubular/solid adenocarcinomas were positive for ER-α, PR, or both. The total immunoreactive scores of ER-α, PR, and mode of myometrial invasion were significantly different between histopathologic types. This suggests that there may be 2 different developmental pathways for uterine adenocarcinomas in the rabbit.
Introduction
Uterine neoplasms are the most common spontaneous neoplasms in the rabbit and have been studied for more than 100 years. 22 The incidence of uterine adenocarcinoma in rabbits 2 to 3 years of age was 4.2%, whereas in rabbits 5 to 6 years of age the incidence was 79.1%. 7 Most cases of uterine adenocarcinoma metastasize within 12 to 24 months after the onset of clinical abnormalities. 22 Gross and microscopic metastases have been found in all organs of the abdomen and thorax, in the thyroid gland, and in the femoral bone marrow. 12
Green et al. (1948) have shown that there are 2 different early changes associated with progression to uterine adenocarcinoma in the rabbit. The first consisted of proliferation of small acini, which replace the stroma and resembles a fetal thyroid adenoma. The second more common mode is characterized by a papillary endometrial glandular proliferation that may become cystic and with papillary projections within the cystic lumina. Myometrial invasion was not always observed, as biopsy samples rarely contained uterine muscle. 11 However, as the neoplastic lesions progress it is more difficult to distinguish between the acinar and papillary type, and the neoplasm has a less obvious glandular pattern. 11
Rabbits are continuous breeders, and ovulation is induced by copulation and some other stimulations. Ovarian follicles at various stage of development are present at all times in the ovaries. 1 Pseudopregnancy is commonly seen in the mature rabbit and is characterized by prolonged maintenance of the corpora lutea and secretion of progesterone in the absence of conceptus. 16 In mature female rabbits, multiple maturing ovarian follicles and multiple corpora lutea occupy the ovarian parenchyma. This suggests that uterine tissue in rabbits is under the influence of both estrogen and progesterone, and that they may promote the neoplastic proliferation of the endometrial epithelium.
It is now well-recognized that hormones play a major role in the development of abnormal proliferative lesion of the endometrium, 20 and in women with uterine adenocarcinomas several studies have shown that the presence and quantity of steroid receptors are correlated with histologic differentiation and survival. 18, 20 In women the expression of steroid receptors by the neoplastic cells is regarded as an important prognostic factor in some reports, because positive cases often show a good response to hormonal therapy. 20, 21
Uterine adenocarcinoma in the rabbit is regarded as an animal model of uterine adenocarcinoma in women 3 and is thought to have a relationship with hormonal stimuli, especially estrogen stimulation. 4 However, to date no work has been carried out on the expressions of estrogen and progesterone receptors in uterine adenocarcinomas in pet rabbits.
Cystic endometrial hyperplasia (CEH) may frequently be found in the uterine tissue of rabbits, but there does not appear to be any consistent view among investigators whether there is progression from CEH to uterine adenocarcinoma. 2, 3, 7, 8– 13, 22 One pathologist showed uterine adenocarcinoma preceded by CEH in all cases by monthly sequential endometrial biopsy via laparotomy. 7, 22 In contrast, another study did not support CEH as a preneoplastic lesion. 3, 22 In women it is uncommon to find simple cystic endometrial hyperplasia progressing to uterine adenocarcinoma. However, in those cases of hyperplasia that are more severe and exhibit more extensive nuclear and cellular atypia, there can be progression to carcinoma. 17, 20
The aims of this study are to evaluate the expression of estrogen receptor-α and progesterone receptors in normal uteri, uteri with endometrial hyperplasia and adenocarcinoma, and to verify the possibility of progression from CEH to adenocarcinoma by finding the site of transition from CEH to adenocarcinoma in the same section.
Materials and Methods
Samples
The source of the uterine samples of rabbits for this study was 1) 60 cases, either biopsy or necropsy samples submitted to the Laboratory of Veterinary Pathology, School of Veterinary Medicine, Azabu University, between 1990 and 2005, and included 23 young rabbits euthanatized for other study; and 2) 32 biopsy samples submitted to the surgical pathology service of the Laboratory of Pathology and Toxicology, University of Pennsylvania, School of Veterinary Medicine, between 1991 and 2004.
Four cases were excluded because of other tumors; therefore, the total number of cases was 88.
Clinical data
Data on the age and breed were obtained from the medical records. Follow-up physical and radiologic examinations were continued at regular intervals by local veterinarians.
Histopathology
The tissues were fixed in 10% neutral buffered formalin and embedded in paraffin. Sections were cut at 4 to 5 μm and stained with hematoxylin and eosin (HE) for histopathologic examination. Additionally, a periodic acid–Schiff stain and reticulin silver stain were performed in some cases of adenocarcinoma to identify the basement membrane zone. The diameters of the tumors on the slides were measured.
Classification of the uterine lesions
The cases were classified as normal uterus, 22 endometrial hyperplasia, 15, 20 or uterine adenocarcinoma. 15, 20 Those cases containing both hyperplastic and adenocarcinomatous areas were classified as adenocarcinomas.
The normal uterus was characterized by the following features: 1) good differentiation between surface and glandular epithelium, 2) regularly distributed glands without evidence of hypersecretion, 3) no cellular or architectural abnormalities, 4) a moderate amount and well-developed stroma, 5) no substantial inflammation, 6) no papillary and polypoid changes in the superficial epithelium, and 7) the presence of both ciliated and nonciliated cells.
Hyperplasia was characterized by the following features: 1) focal or diffuse proliferation of the glands, 2) no stromal invasion, 3) no expansive growth against adjacent mucosa, and 4) occasional adenomyosis (glands in the myometrium).
Cystic endometrial hyperplasia was recognized grossly as the surface was covered by multiple cysts that contained clear fluid. Cysts were covered with ciliated and nonciliated cells. Papillary and glandular hyperplasias were characterized by overgrowth of the superficial epithelium with or without papillary projections with numerous ciliated cells found on histopathology.
Adenocarcinomas were characterized by the following features: 1) focal or diffuse glandular proliferation with cellular or glandular atypia, 2) enlarged nuclei with anisokaryosis and 1 or more prominent nucleoli, 3) frequent mitotic figures, 4) glandular confluences with incomplete basement membranes, and 5) stromal and/or myometrial invasion.
Myometrial invasion
The depth of the myometrial invasion was classified into 4 groups (without invasion of the myometrium, score 0; invasion within the inner circular muscle layer, score 1; invasion within the outer longitudinal muscle layer, score 2; and invasion through the serosa, score 3).
The mode of myometrial invasion was classified into 2 modes. In the expansive mode (type), the neoplastic glands grow either into the lumina or toward the myometrium. With the growth of the neoplasm, the diameter of the uterus increases, and the myometrium is stretched thin. Neoplastic glands infiltrate into the attenuated myometrium. In the invasive mode (type), the neoplastic glands are present in the deep myometrium as a single nest or small clusters of nests, but the thickness of the myometrium remains relatively normal.
Mitotic figures
The number of mitotic figures was counted per 10 high power (HP) fields (×10 ocular, ×40 objective).
Immunohistochemistry
Immunohistochemistry protocol
One to 2 paraffin blocks containing either normal uterus or representative lesions of hyperplastic and/or adenocarcinomas were selected from each case, and serial sections were cut at 4 μm. Indirect high polymer immunostaining was performed using primary mouse monoclonal antibodies to estrogen receptor-α [ER-α, CC4-5, 1 : 200] (Novocastra, UK), and progesterone receptor [PR, MAB462, 1:10,000] (Chemicon International, Temecula, CA). Antigen retrieval was performed at 90°C for 9 minutes in citrate buffer using the microwave method. The tissues were incubated overnight at 4°C with the primary antibodies. The secondary antibody (peroxidase labeled high polymer anti-mouse IgG, Histofine mouse stain kit, Nichirei, Japan) was incubated for 30 minutes at room temperature. 3′3-diaminobenzidine was used to visualize the reaction products. The slides were counterstained with methylgreen.
Positive and negative controls were added in all tests. Normal canine mammary tissues and rabbits' uterine tissues were added as positive controls for ER-α, and normal uterus of rabbits was added as a positive control for PR. All negative controls were incubated with 1% bovine serum albumin-phosphate buffered saline instead of the primary antibody.
Evaluation of immunohistochemical reactions
Classification of staining data was undertaken semiquantitatively by using an immunoreactive score. The percentage of positive nuclei was estimated based on a 4-tiered scale, as a proportional score (PS), (<5% = 0, 6–20% = 1, 21–60% = 2, >60% = 3). A 4-tiered scale was also used for scoring the staining intensity, as an intensity score, (IS) (negative = 0, weak = 1, moderate = 2, strong = 3). The staining intensity was estimated based on the predominant staining intensity in the slides. The PS and IS are added to obtain a total score (TS) (range 0–6). ER-α and PR were considered positive when TS ≥ 3. 19
Statistical analysis
A Kruskal–Wallis test was used for the analysis of the association between age and histopathologic diagnoses. A chi-square test was used to assess the differences of concomitance (with or without) hyperplasia and the mode of myometrial invasion (expansive or invasive growth) between papillary adenocarcinoma and tubular/solid adenocarcinoma.
An unpaired t-test was used to assess the relationship between the 2 types of adenocarcinoma, the TS of ER-α and PR, the mitotic index, and the depth of myometrial invasion. A P value of < .05 was considered to be significant.
Results
Clinical data
Age
Mean age of the cases with normal endometrium was 1.1 years (range 0.5–4.6 year of age), those cases with endometrial hyperplasia was 3.74 years (range 1.25–5.3 years of age), and those cases with adenocarcinoma was 5.3 years (range 1.5–10 years of age). Nineteen out of 20 (95%) cases of normal endometrium were less than 3 years of age, and 33 of 36 (91.7%) of adenocarcinoma were more than 4 years of age. The age of the rabbits with cystic endometrial hyperplasia was significantly higher than the normal rabbits and that of uterine adenocarcinomas was significantly higher than that of the cases of endometrial hyperplasia. The mean age of the rabbits with tubular/solid adenocarcinomas was 4.8 years (range 1.5–7 years) and that of papillary adenocarcinoma was 5.6 years (range 3–10 years of age), but this difference was not statistically significant.
Breed
Information about breeds was available for 61 out of the 88 rabbits. The rabbits with a normal endometrium consisted of 23 mixed breeds and 1 dwarf breed; the rabbits with endometrial hyperplasia consisted of 10 mixed breeds, 1 lop-ear and 1 Dutch; and the rabbits with adenocarcinomas consisted of 15 mixed breeds, 4 dwarfs, 3 lop-ears, 1 Dutch, 1 lion, and 1 rex.
Follow-up information was available on 17 rabbits, with a diagnosis of uterine adenocarcinoma. Seven rabbits died within 6 months following ovariohysterectomy, 6 rabbits survived in good clinical conditions for more than 6 months, and 4 rabbits were euthanatized.
One rabbit showed wide-spread metastasis (carcinomatosis), and 1 rabbit had pulmonary metastasis.
Tumor size
The median tumor size was 1.5 cm diameter (range 0.1–3.2 cm). Three microscopic adenocarcinomas were identified that did not have any grossly detectable lesions. The difference in the size of the tumor between papillary adenocarcinoma and tubular/solid adenocarcinoma was not statistically significant.
Histopathology
A total of 88 cases were included, 27 normal uteri (Fig. 1), 19 hyperplasias, and 42 adenocarcinomas. Three leiomyomas and 1 malignant mixed müllerian tumor 6 were also identified but excluded from the analysis.
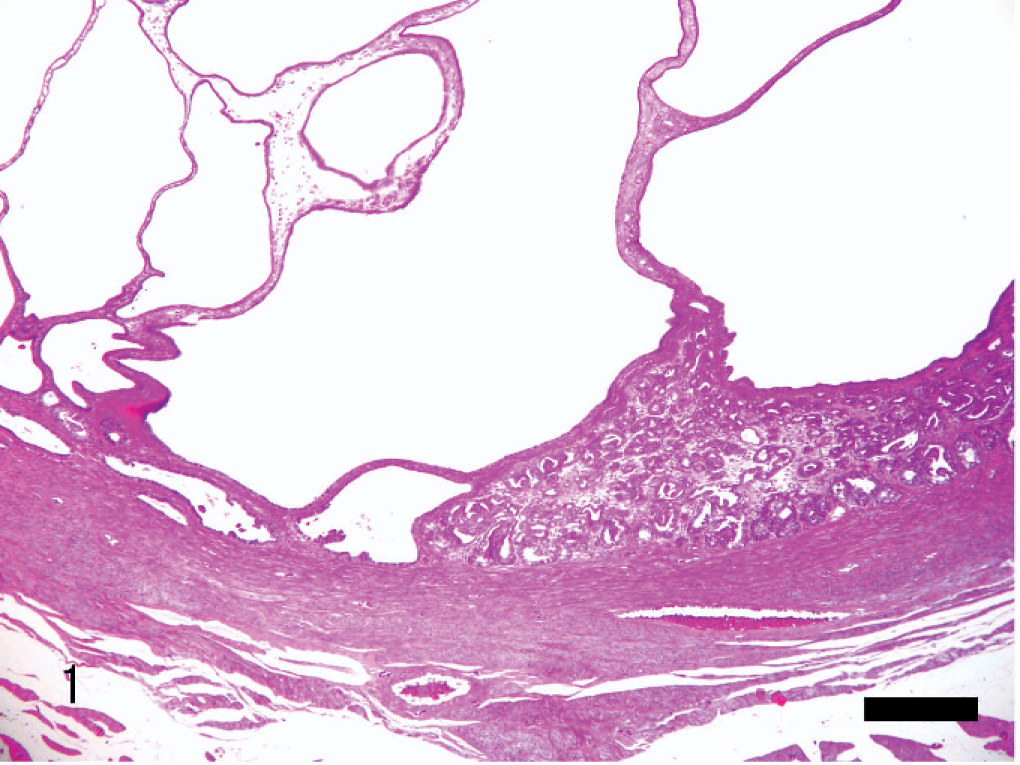
Uterus; rabbit. The early stage of the papillary adenocarcinoma. Cystic endometrial hyperplasia is seen in adjacent mucosa, but the transformation from hyperplastic cells to neoplastic cells is not obvious. HE. Bar = 360 μm.
Adenocarcinomas included 1 case with squamous differentiation and 2 cases with chondoroid metaplasia (Figs. 5, 6).
Two types of adenocarcinoma were present: papillary and tubular/solid type. Adenocarcinomas were further subdivided into 26 papillary and 16 tubular/solid adenocarcinomas.
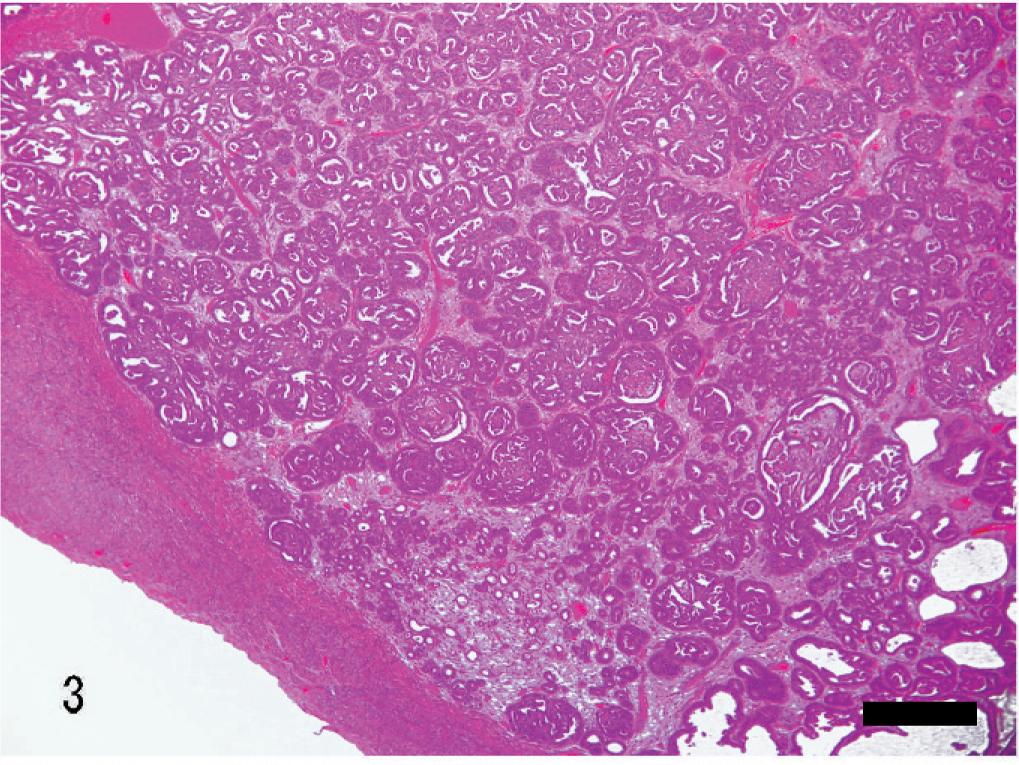
The papillary adenocarcinoma showed a papillary to cribriform expansive growth of the glands (Figs. 1–3). There was myometrial attenuation even in the early stages of tumor development, and with advanced disease there was invasion through the serosa. In the late stage, the papillary architecture was retained, and a cribriform architecture was observed in some cases. When the neoplastic cells showed papillary projection into glandular lumina, they were cuboidal to columnar in their morphology and usually retained their polarity.
The smallest lesion of papillary adenocarcinoma was 1 mm in diameter, without any observed gross changes. In this focal lesion, there were several papillary projections within the glandular lumina and loss of much of the surrounding stroma (Figs. 1, 2). Confluences of glands with an incomplete basement membrane were frequent. Myometrial invasion was lacking. Although marked cystic endometrial hyperplasia was observed in the adjacent mucosa, no transition from hyperplasia to adenocarcinoma was evident (Fig. 1). The mean number of mitoses were 5 per 10 HP fields (×400).
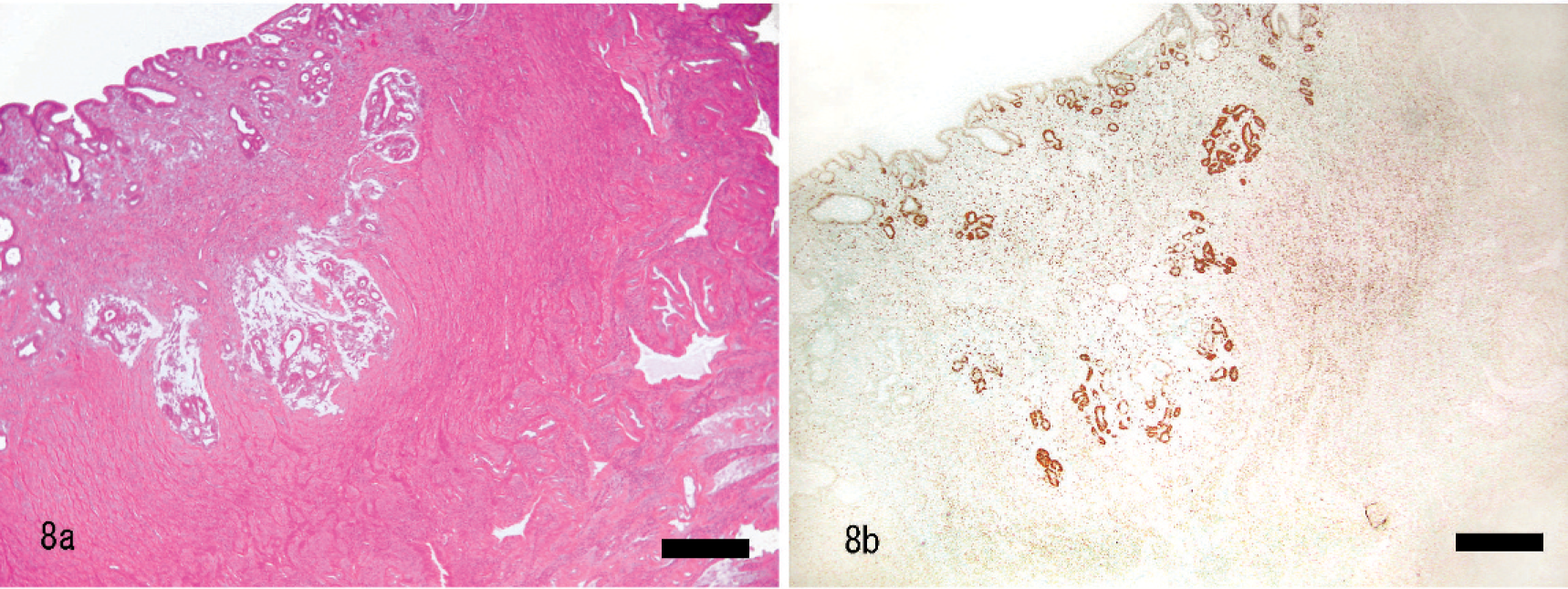
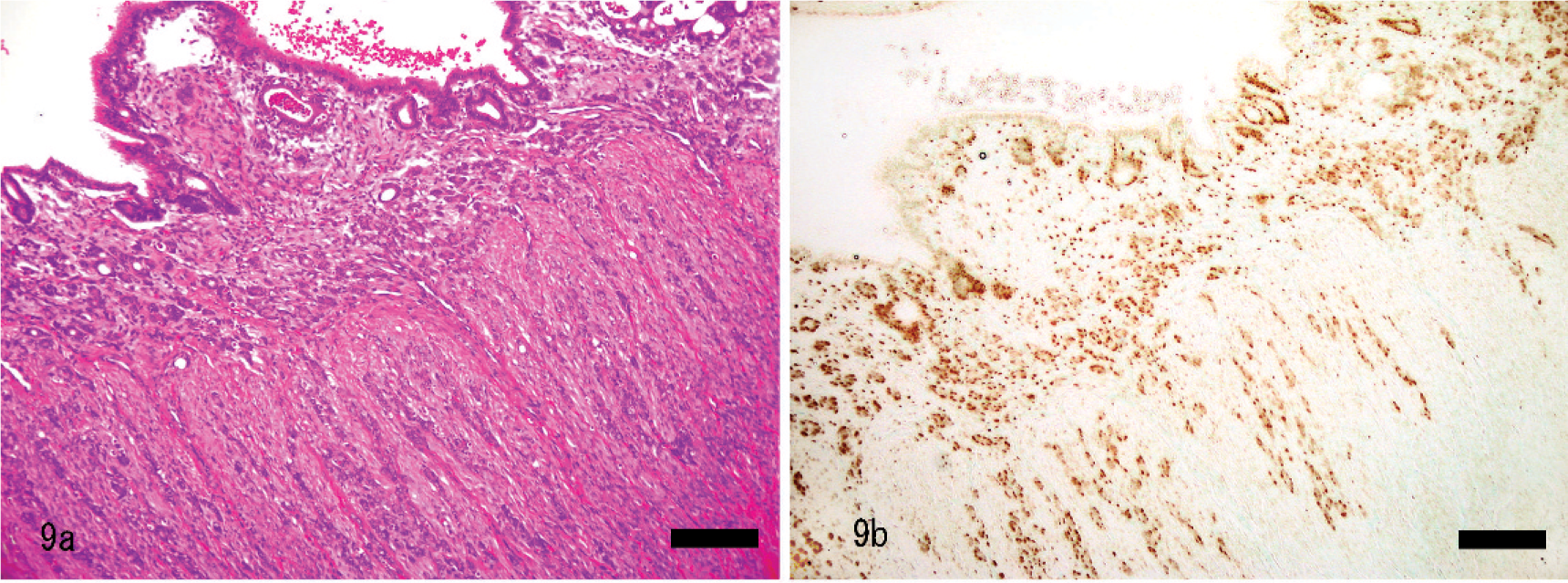
The tubular/solid type of adenocarcinoma was characterized by proliferation of nests of neoplastic cells (Figs. 4, 8–10). Neoplastic cells often formed tubular structures in which the lumina were lined by a single layer of epithelial cells, but no papillary glandular proliferation was observed. Myometrial attenuation was uncommon with this type of adenocarcinoma. The neoplastic tissue often infiltrated into the deep myometrium as a single nest or small nests of neoplastic epithelial cells that were pleomorphic and varied from cuboidal to more fusiform in their morphology. Neoplastic cells had round to ovoid nuclei with small nucleoli and scant eosinophilic cytoplasm. The nuclear to cytoplasmic ratio was high. The mean numbers of mitoses were 6 mitoses per 10 HP fields (×400). In early lesions the neoplasm was not observed grossly, but on histopathology there was invasion into the myometrium without myometrial attenuation (Figs. 8, 9.
Twenty-two out of 42 cases of uterine adenocarcinoma had concurrent cystic endometrial hyperplasia in the adjacent mucosa, but the transition from hyperplasia to adenocarcinoma was not evident in the same sections evaluated. Fourteen out of 26 papillary adenocarcinomas and 8 of 16 tubular/solid adenocarcinomas were associated with adjacent areas of cystic endometrial hyperplasia. The difference between papillary adenocarcinoma and tubular/solid adenocarcinoma with or without cystic endometrial hyperplasia was not statistically significant (P = .81).
Cystic hyperplasia and papillary hyperplasia were 13 and 6 out of 19 hyperplasias, respectively.
Myometrial invasion
Myometrial invasion was seen in 21 out of 26 papillary adenocarcinomas, and 15 out of 16 tubular/solid adenocarcinomas. Two modes of invasion, expansive and invasive, were observed. Most of the papillary adenocarcinomas (19/21, 90.5%) showed an expansive mode. In contrast, most of the tubular/solid adenocarcinomas (14/15, 93.3%) showed an invasive mode.
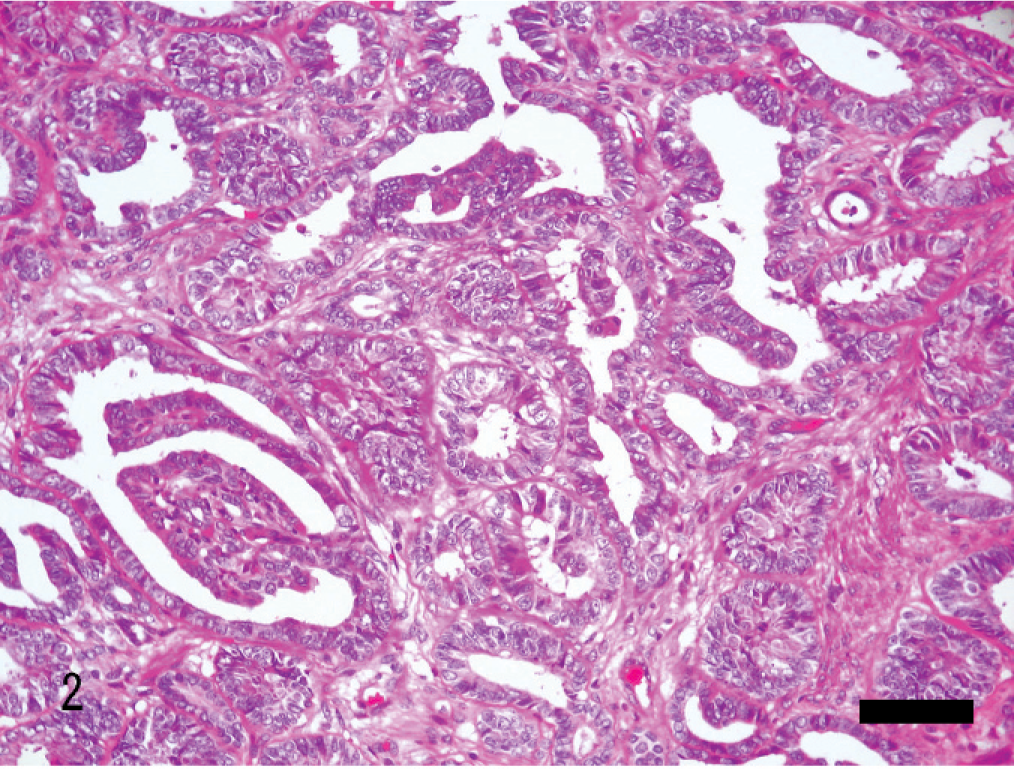
The difference in the mode of myometrial invasion between these 2 types of adenocarcinomas was statistically significant (P < .01). Although the depth of myometrial invasion in tubular/solid adenocarcinomas tended to be deeper than papillary adenocarcinomas, the difference was not statistically significant.
Mitotic figures
Mitotic figures were 1 to 31 per 10 HP fields among adenocarcinomas. There was an average of 7.1 mitoses/10 HP fields in tubular/solid adenocarcinomas (range 3–21) and 12.7 mitoses/10 HP fields in papillary adenocarcinomas (range 1–31). Mitotic figures in the papillary adenocarcinoma were significantly more frequent than in tubular/solid adenocarcinoma (P = .012).
Hormonal receptors
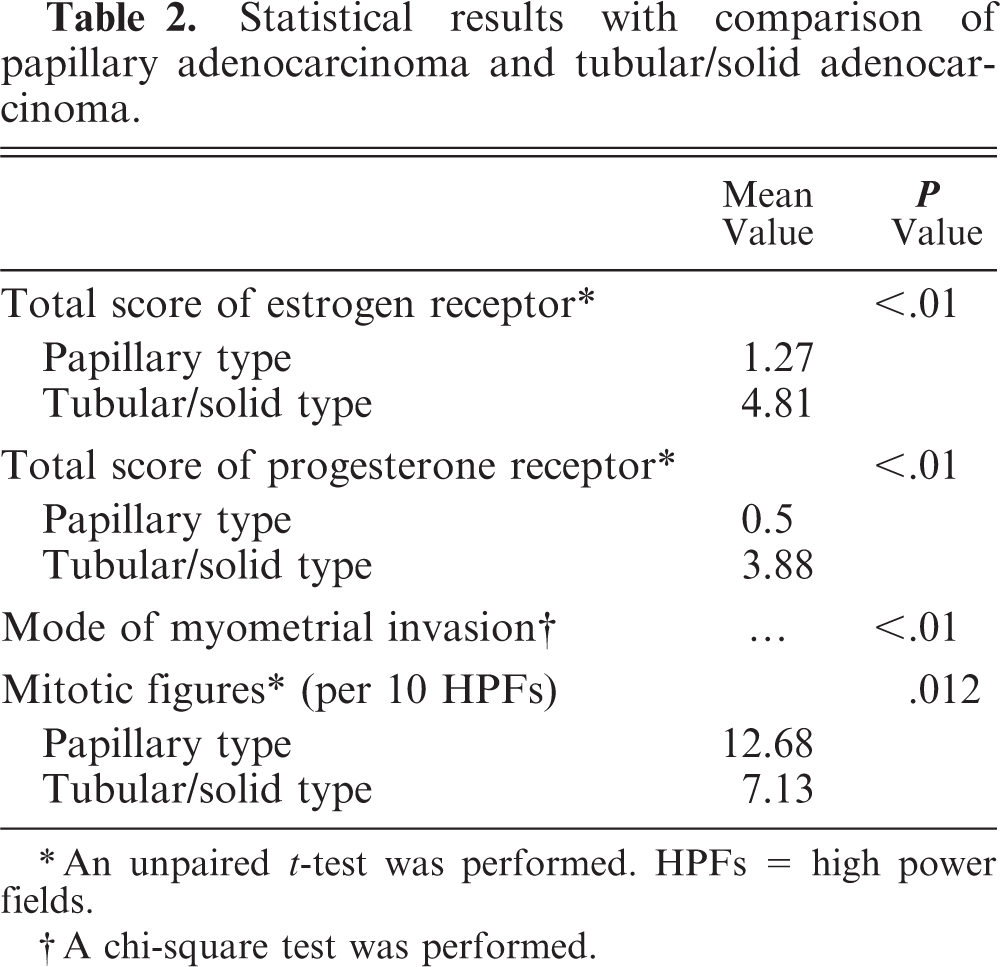
In the normal rabbit uterus the nuclei of epithelial cells, stromal cells, and smooth muscle cells of the myometrium were positive for ER-α and PR, whereas endothelial cells were negative (Fig. 7b). The expression of ER-α and PR receptors by normal, hyperplastic, and uterine adenocarcinomas is shown in Table 1. In the papillary adenocarcinoma group 21/26 (80.8%) were both ER-α and PR negative, whereas in the tubular/solid adenocarcinoma group 14/16 (87.5%) were positive for ER-α, and 13/16 (81.3%) were positive for PR and 12/16 (75.0%) were positive for both. The total immunoreactive scores of ER-α and PR were significantly different between the 2 histopathologic types (P < .01) (Table 2). The case that was negative for both ER-α and PR in the tubular/solid adenocarcinoma group showed squamous differentiation and chondoroid metaplasia (Figs. 5, 6).
Immunohistochemical results of ER and PR in normal uteri, endometrial hyperplasia, and uterine adenocarcinoma in rabbits.
Statistical results with comparison of papillary adenocarcinoma and tubular/solid adenocarcinoma.
An unpaired t-test was performed. HPFs = high power fields.
A chi-square test was performed.
TS for ER-α and PR were significantly lower in adenocarcinomas than those of hyperplasias and the normal group (ER-α: P < .05, PR: P < .01), but there was no significant difference between the normal group and the hyperplastic lesions. PR-positive adenocarcinomas had significantly fewer mitoses than PR-negative adenocarcinomas (P < .05). There was no significant relation between ER-α status and the number of mitotic figures. There was also no relation between depth of myometrial invasion and ER-α and PR positivity.
Discussion
Uterine adenocarcinomas in rabbits were classified into 2 types, papillary and tubular/solid type, based on the prominent architecture of the neoplastic tissue. These 2 types of adenocarcinomas were considered to be synonymous with the 2 types, which were identified as having papillary and acinar patterns in the previous report. 11
Histopathologic and immunohistochemical findings suggested 2 developmental pathways of uterine cancer in this species. Papillary adenocarcinoma lose the expression of ER-α and PR in the early stages of their development, and a cluster of neoplastic glands grows expansively with attenuation of the myometrium and with invasion into the myometrium in the late stages of the glands' development. In contrast, tubular/solid adenocarcinomas maintain their ER-α and PR expression and infiltrate into the myometrium from an early stage, without attenuation of the myometrium (Figs. 8b–10b).
This study showed that the histopathologic pattern correlates with the expression of ER-α and PR in uterine adenocarcinoma in rabbits. In humans, it has been reported that the expression of hormone receptors also correlates with histologic differentiation in uterine adenocarcinoma. Well-differentiated adenocarcinomas express many receptors, whereas poorly differentiated adenocarcinomas express few receptors. 5, 17, 18
This report showed no evidence of any progression from cystic endometrial hyperplasia to adenocarcinoma in the same section. Cystic endometrial hyperplasias were seen in the adjacent mucosa in approximately half of the papillary and tubular/solid adenocarcinomas and were not present in the remainder of the adenocarcinomas.
This study indicated that adenocarcinomas may occur without hyperplasia, but further study by other method is needed to clarify if cystic endometrial hyperplasia ever progresses to adenocarcinoma.
In a previous report, it was suggested that it may be difficult to differentiate between the papillary and acinar types of adenocarcinoma. 11 However, although there were foci where the neoplasm had areas with a cribriform morphology, most of the tumor retained a prominent papillary pattern. We therefore believe that the 2 tumor types can be differentiated even in the late stages of the disease.
In this study, there was an increase in the average age as the rabbits developed endometrial hyperplasia and adenocarcinomas. This result is similar to that found in previous studies. 4, 5, 8– 11, 13, 14, 22
The major breed in this study was the mixed breed, which suggests this is the most common breed of pet rabbit in Japan and the USA. The number of other breeds was too small to identify any breed predisposition.
The mean size of tumor was 1.5 cm diameter in this study. However, further study using serial sections of whole uteri may reveal a smaller median size, since some microscopic adenocarcinomas were incidentally identified though limited sections that were evaluated in this study.
One case of adenocarcinoma with squamous differentiation and 2 cases with chondoroid metaplasia were observed (Figs. 5, 6). In humans, the frequency of endometrial carcinoma with squamous differentiation is unknown, ranging from 5 to 41% of endometrial carcinoma. 20 These are further classified into adenoacanthoma (benign-appearing with favorable prognosis) and adenosquamous carcinoma (malignant-appearing and worse prognosis). 17, 20 To the authors' knowledge, no previous literature has mentioned either squamous differentiation or chondroid metaplasia of uterine adenocarcinomas in rabbits. Further study is needed to clarify its biological behavior in this species.
Four of the 27 normal endometria were negative for both ER and PR receptors. However, smooth muscle cells and stromal cells in the same sections stained positive for ER-α or PR in 2 of the 4 cases. This result indicates that ER-α and PR of the endometrium in the rabbit may only be expressed at a low level, insufficient to be visualized with this immunohistochemical method on formalin-fixed, paraffin-embedded tissue. Further study by more sensitive methods or with frozen tissues may be able to visualized ER-α and PR in all cases with normal endometria.
Over 80% of the cases of cystic endometrial hyperplasias were ER-α positive, which implies that cystic endometrial hyperplasias in rabbits may occur as a result of estrogen stimulation, similar to the findings in women. 20
In this study, the result of the immunohistochemistry did not provide any evidence of any correlation between being ER-α and PR positive and the prognosis. This indicates the prognosis of adenocarcinoma in rabbits is independent of the expression of sex steroid hormone receptors.
In conclusion, our study provides evidence that uterine adenocarcinoma in rabbits develops along 2 pathways. The 2 types of adenocarcinoma have different expression of ER-α and PR receptors and differences in the mode of myometrial invasion. Further studies are needed to determine whether the expression of ER-α and PR may be useful when determining the appropriateness of hormonal therapy in the treatment of this neoplasm.
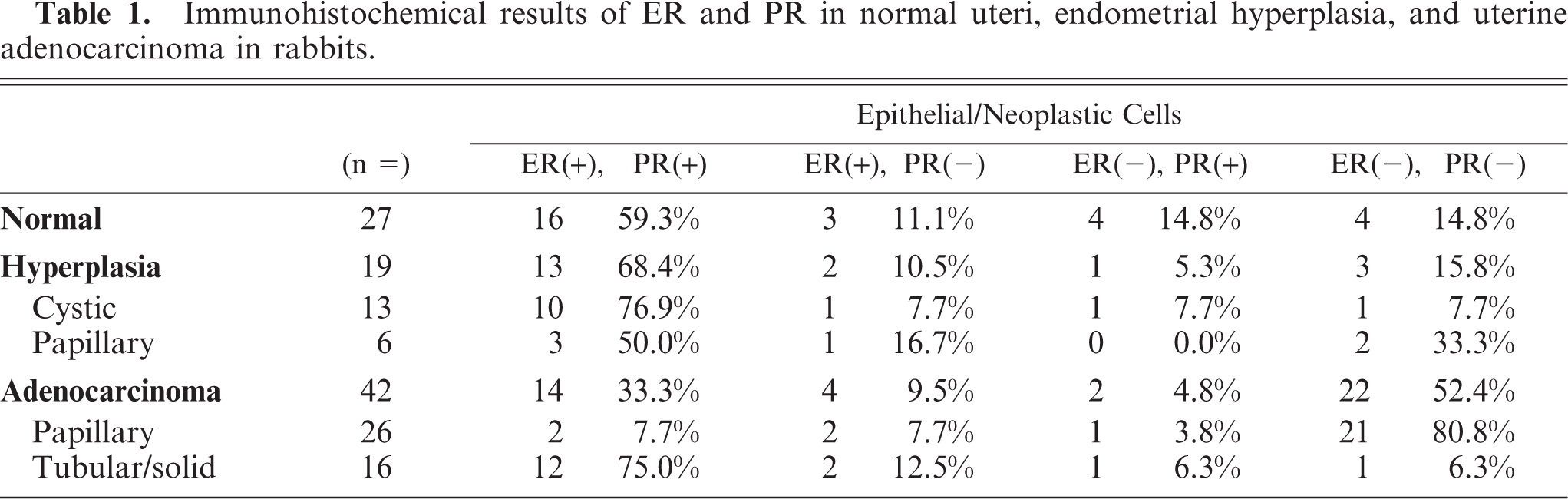
Uterus; rabbit. Papillary adenocarcinoma. Neoplastic cells commonly show protrusion into the lumina of the neoplastic glands. HE. Bar = 80 μm.
Uterus; rabbit. Papillary adenocarcinoma. Clusters of neoplastic glands proliferate expansively against the myometrium with thinning of myometrium. HE. Bar = 360 μm.
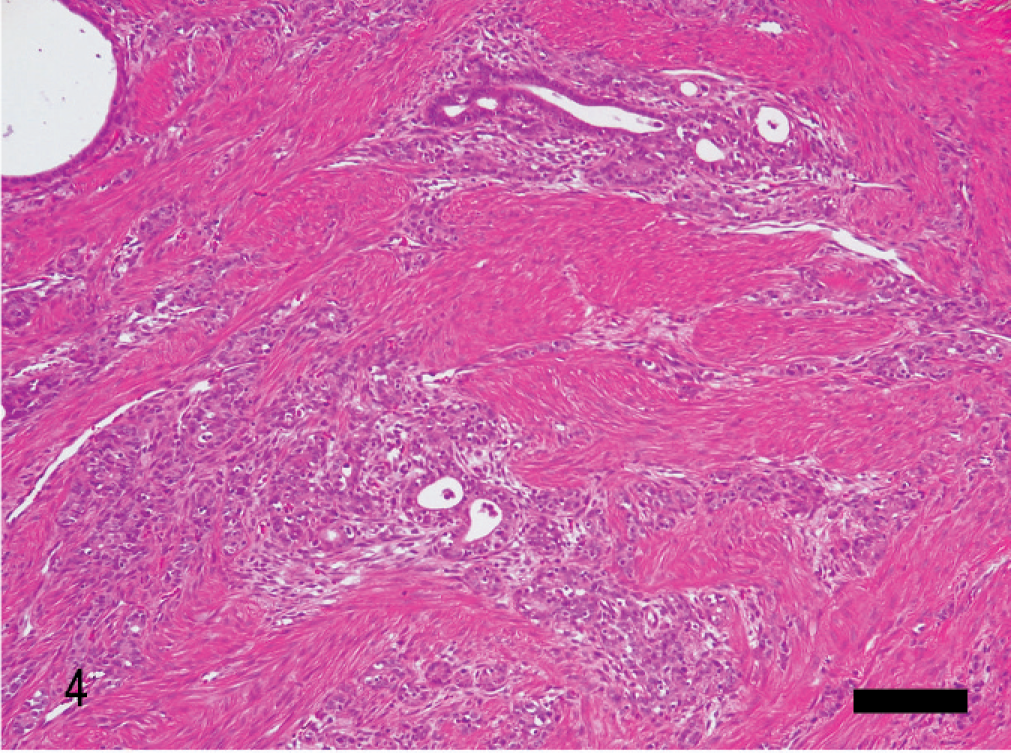
Uterus; rabbit. Tubular/solid adenocarcinoma. Neoplastic glands infiltrate into myometrium without thinning of myometrium. HE. Bar = 360 μm.
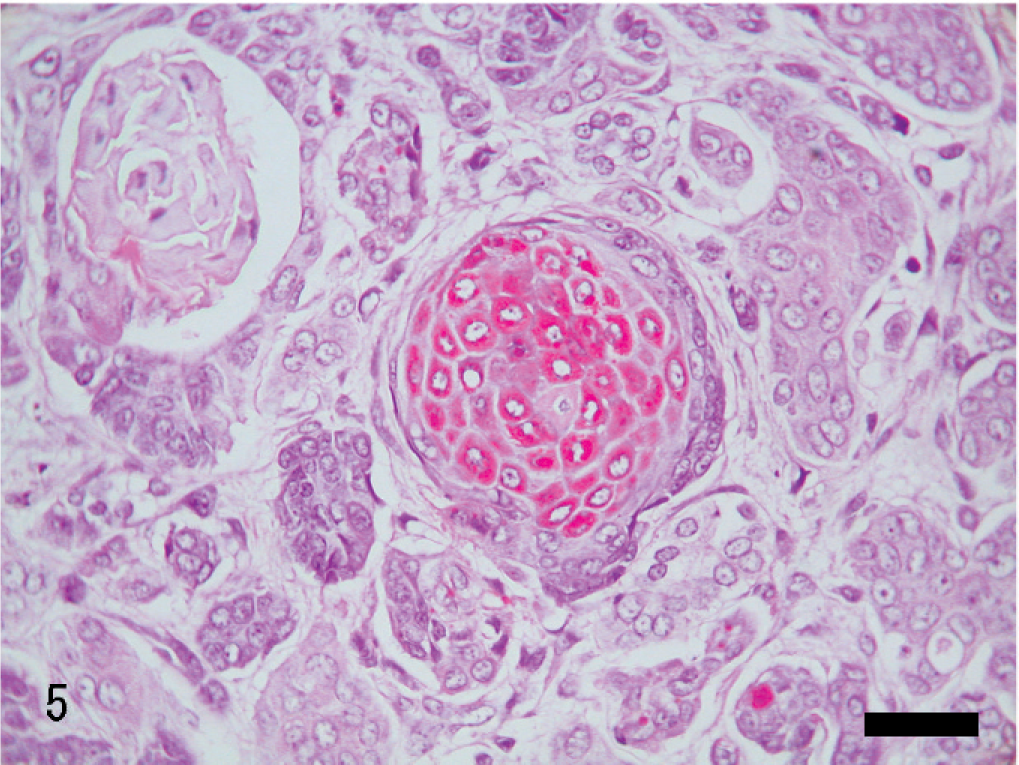
Uterus; rabbit. Tubular/solid adenocarcinoma with squamous differentiation. HE. Bar = 36 μm.
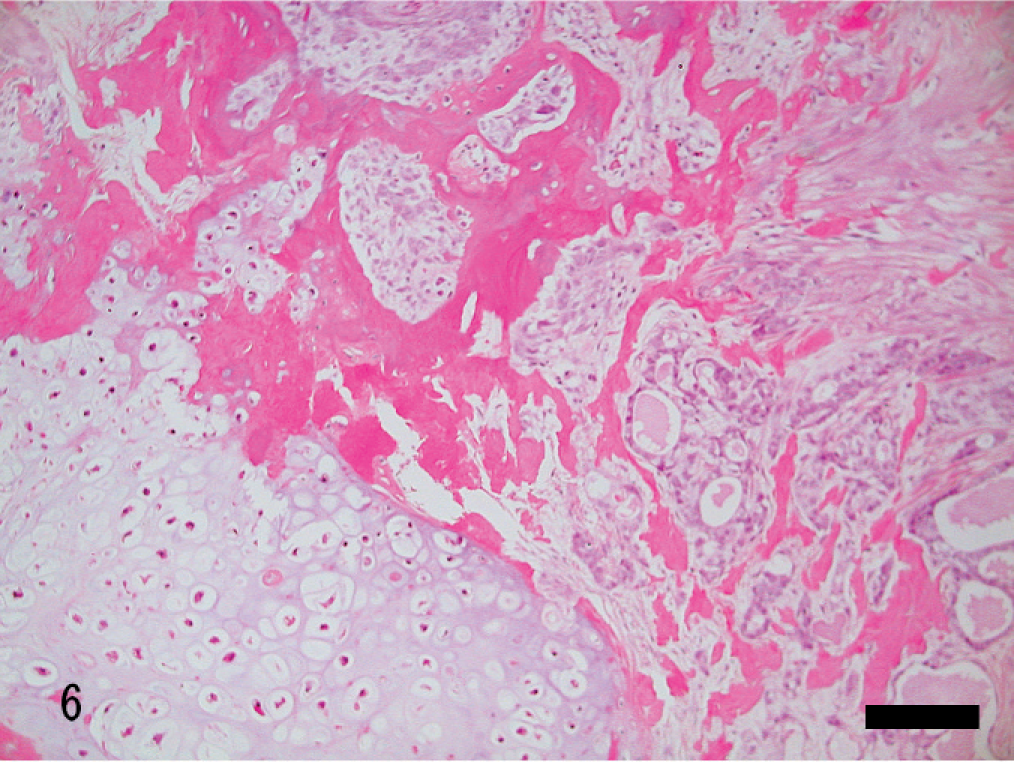
Uterus; rabbit. Tubular/solid adenocarcinoma with chondoroid metaplasia. HE. Bar = 140 μm.
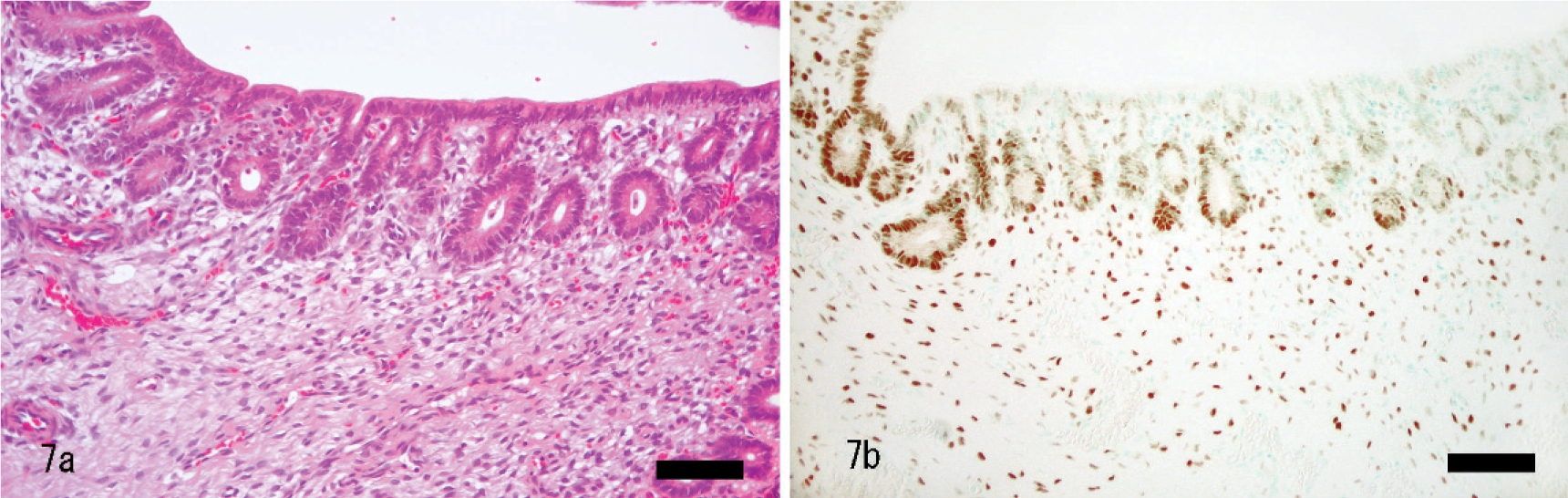
Normal endometrium. Epithelial cells and stromal cells are stained positive with monoclonal mouse anti-human estrogen receptor-α antibody.
Uterus; rabbit. In the early stage of tubular/solid adenocarcinoma. Neoplastic tubular glands invade into myometrium without thinning of myometrium. HE.
Uterus; rabbit. In the early stage of tubular/solid adenocarcinoma. Small nest of neoplastic cells invade into deep myometrium without attenuation of myometrium. HE.
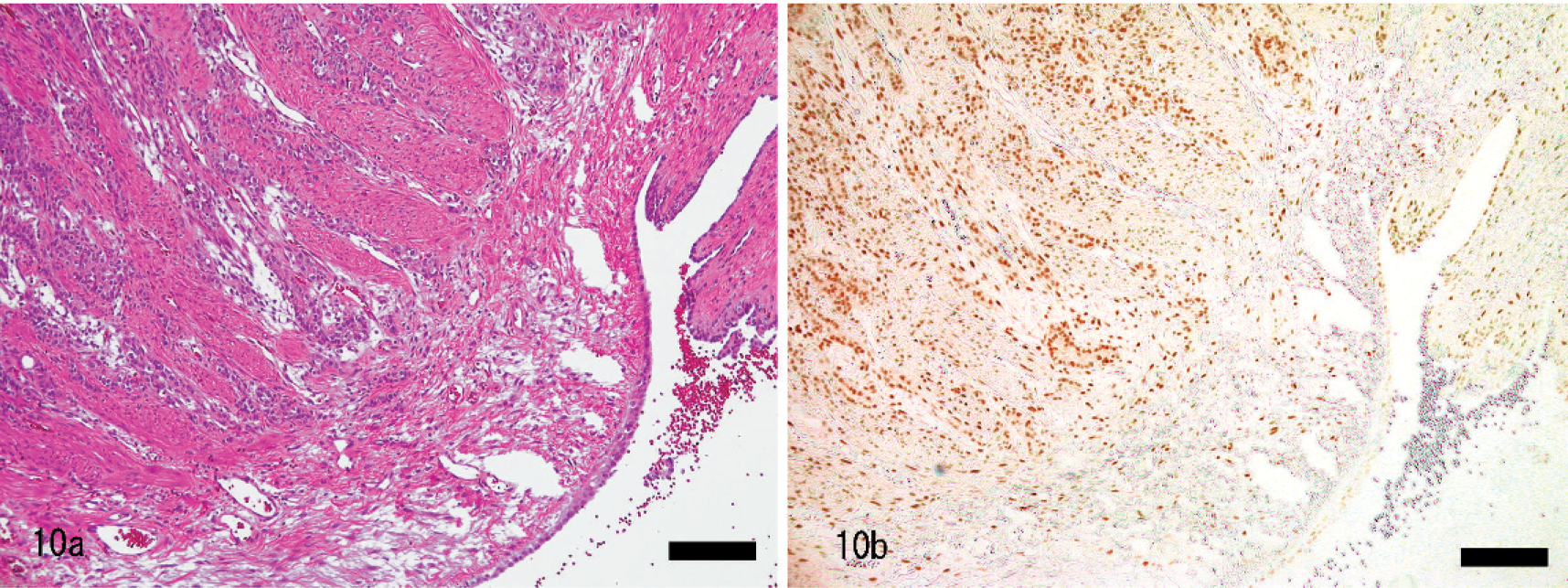
Uterus; rabbit. In the late stage of tubular/solid adenocarcinoma. Neoplastic glands invade deeply into myometrium without thinning of the myometrium. HE.
Footnotes
Acknowledgements
We thank Dr. Hagiwara and Dr. Ito for the helpful discussion and Dr. Okuda, Dr. Kamishima, Dr. Shindo, and Dr. Hashimoto for provision of the samples.