
Abstract
A disfiguring and debilitating neoplastic condition known as devil facial tumor disease (DFTD) has been discovered in wild Tasmanian Devils (Sarcophilus harrisii) across 51% of its natural range, with population declines of up to 80% in some areas (C. Hawkins, personal communication). Between 2001 and 2004, 91 cases were examined. The tumors presented as large, solid, soft tissue masses usually with flattened, centrally ulcerated, and exudative surfaces. They were typically multicentric, appearing first in the oral, face, or neck regions. Histologically, the tumors were composed of circumscribed to infiltrative nodular aggregates of round to spindle-shaped cells, often within a pseudocapsule and divided into lobules by delicate fibrous septae. They were locally aggressive and metastasized in 65% of cases. There was minimal cytologic differentiation among the tumor cell population under light and electron microscopic examination. The results indicate DFTD to be an undifferentiated soft tissue neoplasm.
Tasmanian Devils (Sarcophilus harrisii) are the world's largest carnivorous marsupial and are native to the island state of Tasmania in Australia. They inhabit coastal scrub and sclerophyll forest 5 where they are primarily nocturnal solitary animals scavenging on dead or dying animals. 5
Until recently S. harrisii were relatively common throughout their natural range. However, fears for the survival of the species were raised in June 2002 when a disease named devil facial tumor disease (DFTD) was associated with an unprecedented decline in their population at Freycinet Peninsula on Tasmania's east coast. DFTD is now recognized as occurring in the north, central, east, and south areas of Tasmania. Other records of population declines of S. harrisii in Tasmania were reported around 1863 and in 1908–1920, 5 but no explanations were given for these occurrences.
The purpose of this article is to describe the gross, microscopic, and ultrastructural features of DFTD to better understand the neoplasm's histogenesis and biological behavior.
Materials and Methods
Samples were collected from wild populations of S. harrisii from different geographic locations throughout Tasmania at the location where they were caught, or the animals were taken to the Tasmanian Animal Health Laboratory (TAHL) for necropsy. Archived materials held at museums in the form of pelts, bones, taxidermal specimens, and formalin-fixed materials were also examined.
Animals and gross pathology
The gross appearance and anatomical distribution of lesions in 91 S. harrisii suspected of DFTD were described. These cases came from live and deceased animals from June 2001 to December 2004 from a variety of geographic locations throughout Tasmania. Live S. harrisii were sedated either with a combination of detomidine (50 μg/kg of Domitor) and butorphanol (0.4 mg/kg of Torbugesic) or anesthetized with Isoflurane at an induction concentration of 5% for 3–5 minutes and then maintained at 1–3%. Animals selected for full postmortem examination were euthanized by an overdose of intravenous sodium pentobarbitone (Lethobarb, Virbac [Australia] Pty Ltd.). Tissues examined at necropsy and sampled for histology included the neoplasms, facial skin, brain, pituitary gland, trigeminal nerve, tonsils, salivary gland, submandibular lymph node, brachial plexus, lung, liver, spleen, stomach, small intestine, large intestine, kidney, adrenal gland, bladder, ovary, testes, mammary gland, and bone marrow.
Collections of pelts (n = 33), taxidermal specimens (n = 8), wet formalinized whole S. harrisii (n = 8), and skulls (n = 125) at the Queen Victoria Museum, Launceston, and the Tasmanian Museum and Art Gallery, Hobart, were examined.
Historic laboratory submissions of S. harrisii tissues to the TAHL (n = 87) for the period 1982–2000 were re-examined. Histologic sections of DFTD were sent to the Australian Registry of Wildlife Health (ARWH) and San Diego Zoo for comparison with archived materials at their respective locations. The records at ARWH spanned from 1970 to 1997 and the records at San Diego Zoo from 1958 to 2003.
Cytology
Cytologic examinations of primary skin neoplasms were conducted on 13 DFTD cases by light microscopy of fine needle aspirates or impression smears. Slides were air dried, fixed with methyl alcohol, and stained with Diff Quick (Lab Aids Pty Ltd).
Histology
All tissue samples were collected as either surgical punch or excisional biopsies and fixed in 10% neutral buffered formalin for up to 7 days and then routinely processed into paraffin blocks, from which 3-μm sections were cut and stained with hematoxylin and eosin (HE) and examined using routine light microscopy. Alcian blue (acid mucins), aldehyde fuchsin (insulin), Masson's–Fontana (melanin), Gordon and Sweet (reticulin), Masson's trichrome (collagen), methyl green pyronin (ribonucleic acid), periodic acid–Schiff (carbohydrates), toluidine blue (mast cell granules), Van Gieson (collagen), and Verhoeff's (elastin) stains were conducted on selected cases. 1
As a preliminary definition, any S. harrisii with a neoplasm composed of round to spindle-shaped cells arising in the dermis or subcutaneous tissue was considered within the spectrum of DFTD. Those neoplasms that did not fit this criteria were classified according to Meuten. 7
Transmission electron microscopy
DFTD neoplasms for transmission electron microscopy (TEM) examination were obtained by direct glutaraldehyde fixation, postformalin fixation, or from formalin-fixed paraffin-embedded (FFPE) tissues. Fresh samples were collected directly into Karnovsky's fixative. FFPE tissues were deparaffinized and rehydrated. All fixed samples were then washed in 0.1-M cacodylate buffer (pH 7.2) before being postfixed in 1% osmium tetroxide for 1 hour. The samples were washed in distilled water before being stained en bloc with 5% uranyl acetate for 30 minutes and then dehydrated through graded alcohol (50–100%), cleared in propylene oxide, infiltrated and embedded into epon resin, and polymerized at 60°C.
Survey sections (1 μm) were cut on a LKB 2088 Ultratome V and stained with toluidine blue, and the area of interest identified for ultrathin sectioning (70–90 mm) was cut with a Diatome diamond knife. Sections were placed into copper electron microscopy 200 hexagonal mesh grids and stained with uranyl acetate and lead citrate before examination with a Philips CM100 transmission electron microscope. The nuclear and cytoplasmic sizes from 100 random cells were measured, and the mean and standard deviation were determined using a Microsoft Excel spreadsheet.
Results
Gross results
Tumors were well circumscribed in 87% (61/70) of DFTD cases (Fig. 1). They were typically firm soft tissue masses, usually with flattened, centrally ulcerated, and exudative surfaces. The cut surface of the DFTD lesions were firm, pale to slightly translucent, and multinodular, with visible fibrous septae and sometimes with a necrotic core (Fig. 2). Tumors typically affected the oral mucosa or facial skin and 68% (58/85) of cases were multicentric (Fig. 1). In 74% (52/70) of the cases, the DFTD lesions were larger than 3 cm and ulcerated. The distribution of all nonmulticentric tumors was examined; 62% (16/26) occurred on the oral mucosa, and 38% (10/26) on the haired part of the face.

Tasmanian Devil. Multicentric distribution of DFTD around the head with characteristic large firm tumors with a flat ulcerative surface. Bar = 100 mm.
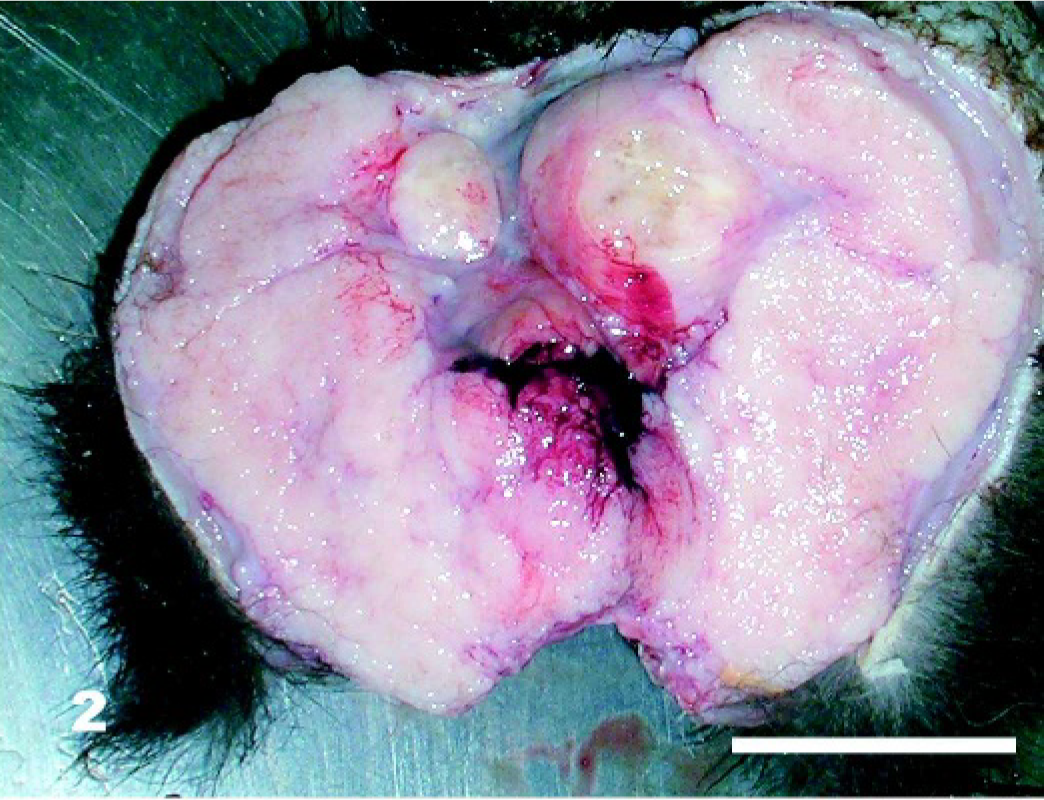
DFTD neoplasm; Tasmanian Devil. The cut surface shows a multifocal coalescing solid mass of glistening pale tissue, often with central necrosis. Bar = 40 mm.
Fifty-three percent (45/85) of affected animals were females and 47% (40/85) males. Of those diagnosed with DFTD with known ages, 17% (13/77) were 2 years old, 52% (40/77) were 3 years old, 26% (20/77) were 4 years old, and 5% (4/77) were more than 4 years old.
The pelts (n = 33), taxidermal specimens (n = 8), wet formalinized whole animals (n = 8), and skulls (n = 125) collected from 1941–1989 showed no signs of DFTD.
Cytology results
In those cases where cytologic sampling was performed there was good recovery of poorly differentiated round cells. Many cells occurred singly but had a tendency to cluster in some regions (Fig. 3). The cells featured cytologic atypia including anisocytosis, anisokaryosis, and a high nuclear to cytoplasmic ratio (1°1.2). They had single, large, round, eccentrically located basophilic nuclei with a granular chromatin pattern and a hazy pale blue cytoplasm. No nucleoli were present. Mitotic cells were rare. There were also low numbers of erythrocytes and neutrophils in preparations.
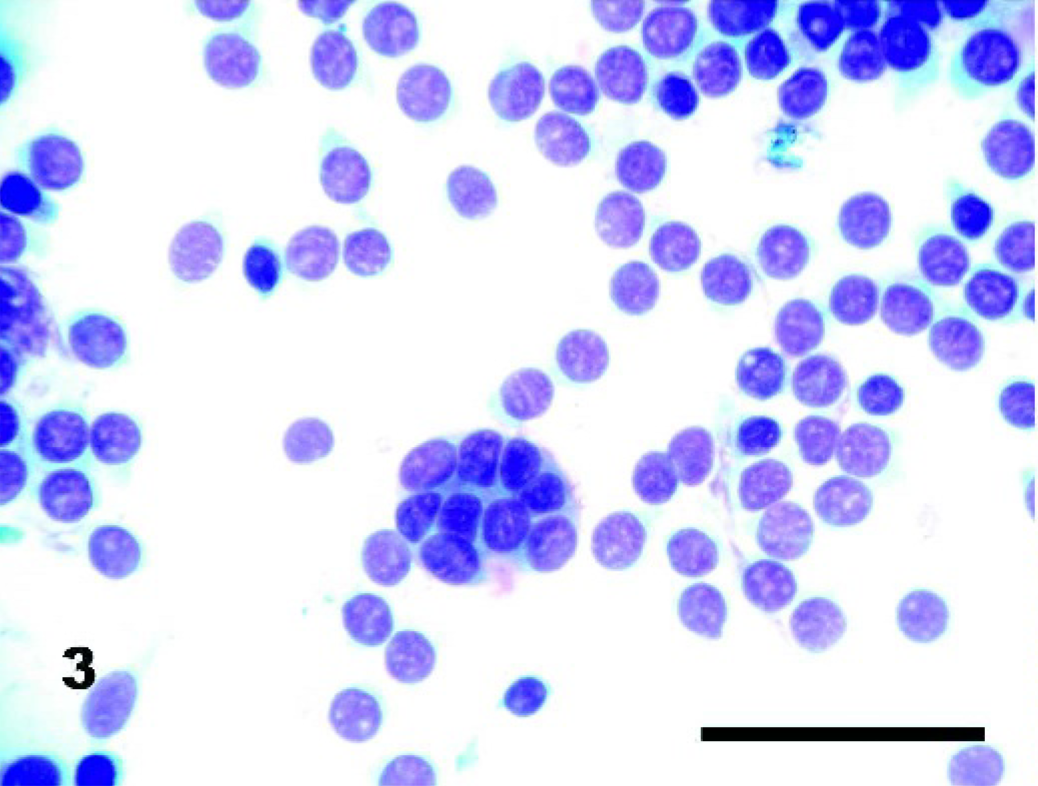
DFTD neoplasm; Tasmanian Devil. They are characterized by large round cells with a uniform round nucleus, high nuclear to cytoplasmic ratio, and bluish cytoplasm. A tendency for the cells to aggregate is also shown. Fine needle aspirate. Diff quick. Bar = 50 μm.
Histopathology results
All DFTD neoplasms examined appeared microscopically similar. The neoplasms were located and appeared to originate within the dermis (Fig. 4) or the submucosal connective tissue in the oral cavity. The neoplasms were composed predominantly of multinodular compact proliferations of pleomorphic round cells with a high nuclear to cytoplasmic ratio; fibrillar, eosinophilic cytoplasm; and often indistinct cell borders. The neoplasms formed well vascularized densely cellular, circumscribed to minimally infiltrative, large nodular aggregates, often within a thin fibrous pseudocapsule. In some cases the cells were arranged in bundles, cords, or streams; in others, there were palisades, packets, nests, or sheets. All neoplastic cells contained a single round nucleus that was usually centrally located and lacked visible nucleoli. Nuclear patterns were predominantly granular or vesicular. The number of mitoses per high power field ranged from 0–12, with 34% having more than 3 per field (400× magnification). Necrosis was a major feature in 73% of cases. No inflammatory cells were observed in 68% of cases; 26% of cases featured a mild peripheral infiltration with neutrophils and 7% contained evidence of lymphocytic infiltration in HE sections. Vascular invasion was observed in 4% of cases, with 1 case presenting with obvious emboli in the coronary and renal arteries. Evidence of hemorrhage was variable.
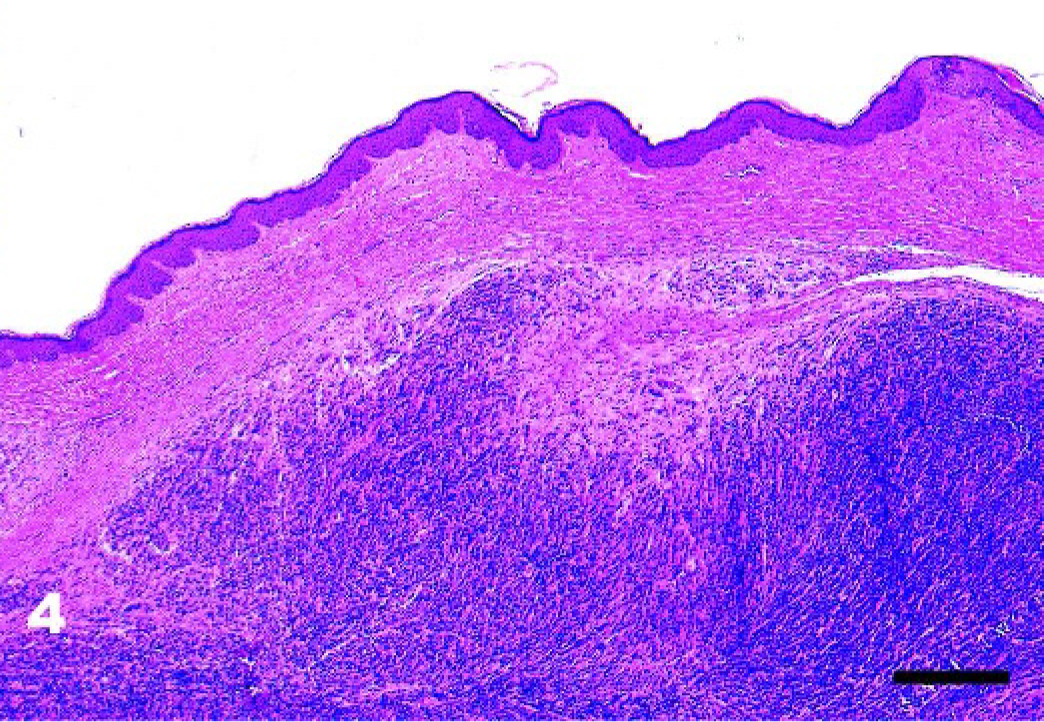
Facial skin; Tasmanian Devil. The neoplasm occurs in the dermis and present as well circumscribed masses, compressing the surrounding connective tissue. HE. Bar = 500 μm.
Metastases occurred in 65% of cases with 57% having regional lymph node involvement and 41% involved distant metastases. Of these, 47% had metastasized to the lungs (Fig. 5); 12% to the spleen; 6% to the heart (Fig. 6), ovary, and serosal surface of the rib; and 5% each to the kidney, mammary, adrenal (Fig. 7), and pituitary glands (Fig. 8).
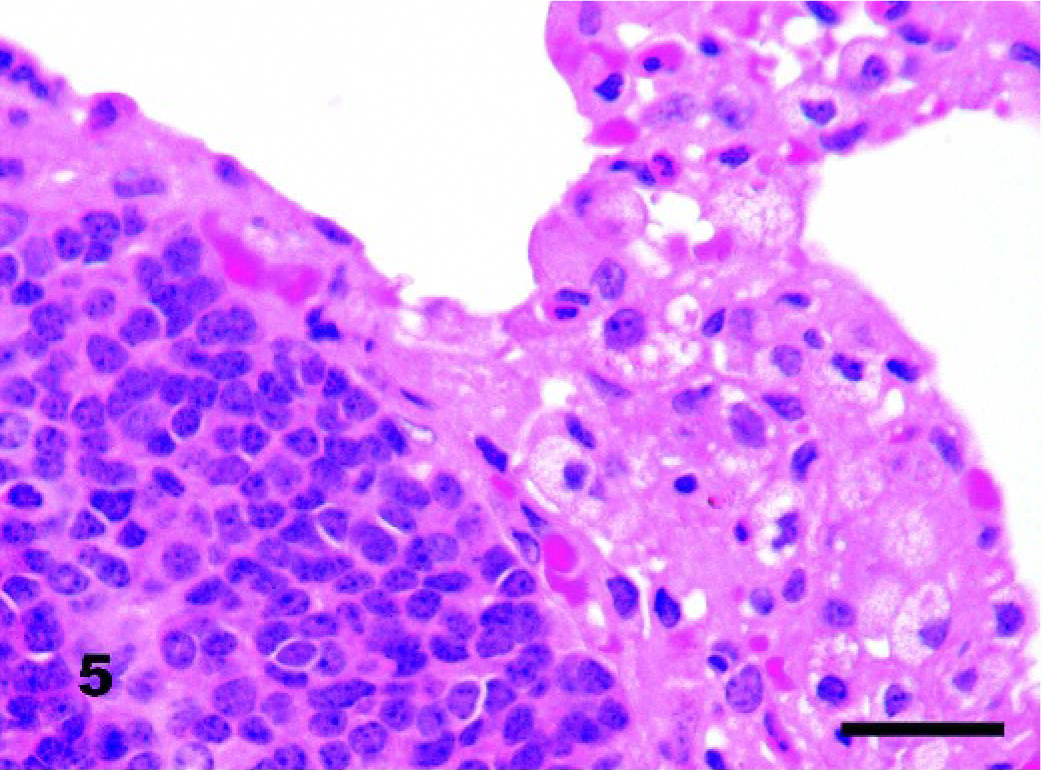
Lung; Tasmanian Devil. Metastases to the lungs occurred in 32% of cases. HE. Bar = 30 μm.
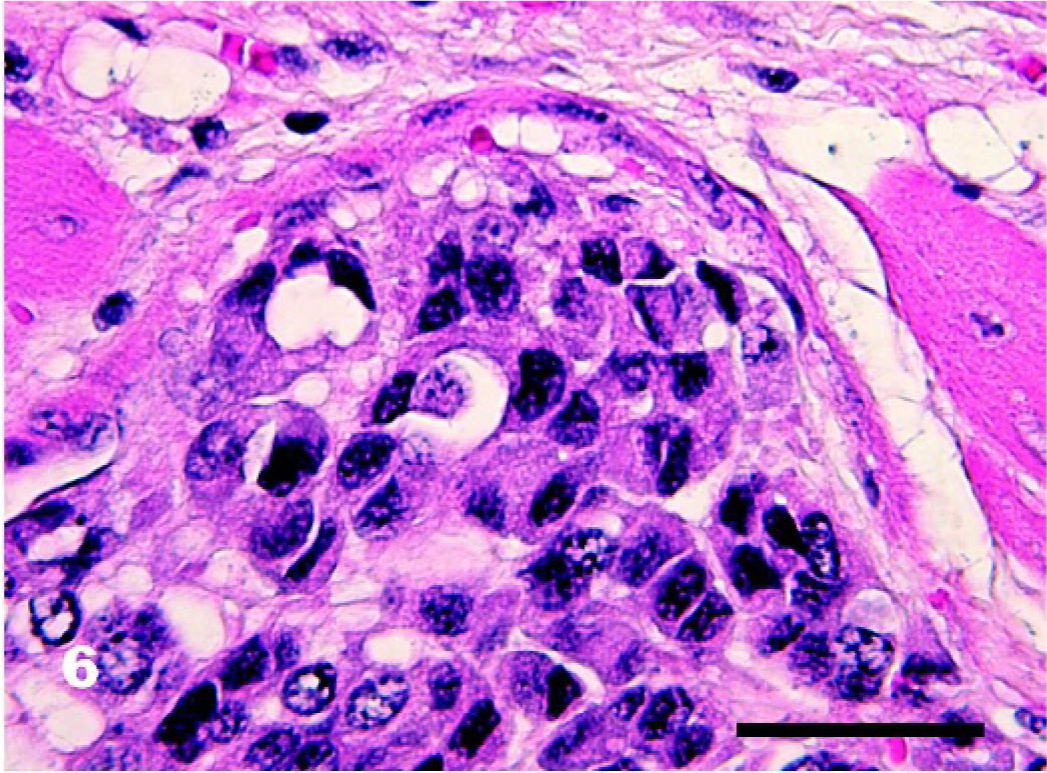
Heart; Tasmanian Devil. Tumor embolus within a coronary artery. HE. Bar = 25 μm.
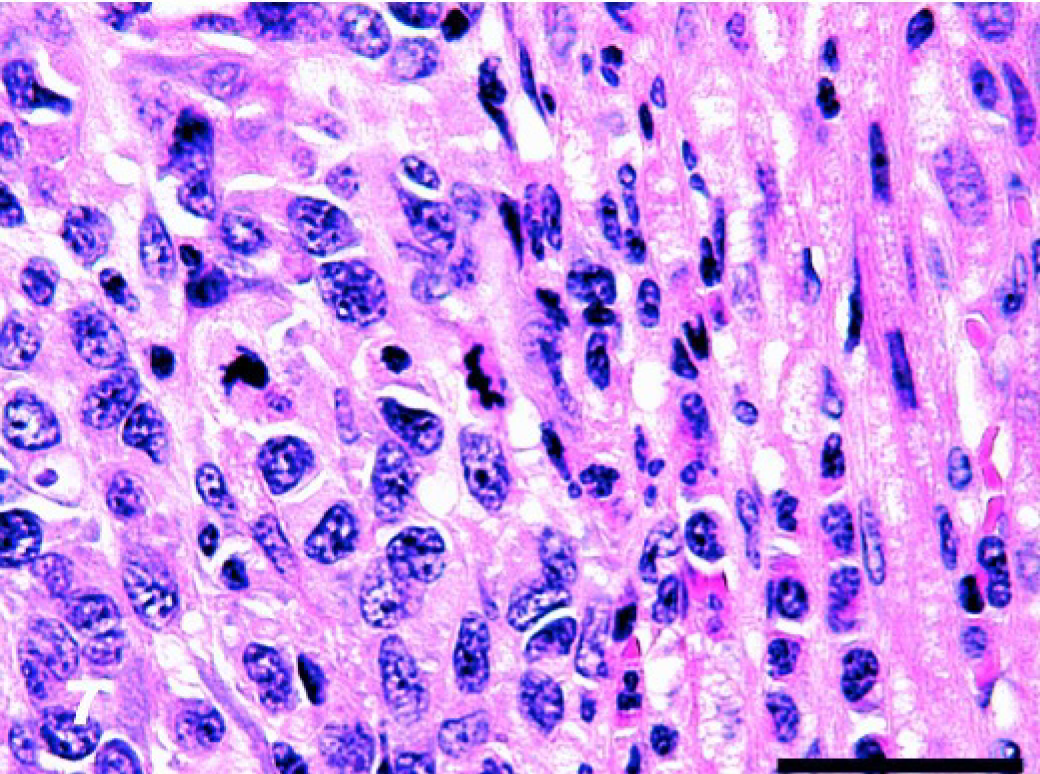
Adrenal gland; Tasmanian Devil. DFTD metastasis in the cortex of the adrenal gland. HE. Bar = 25 μm.
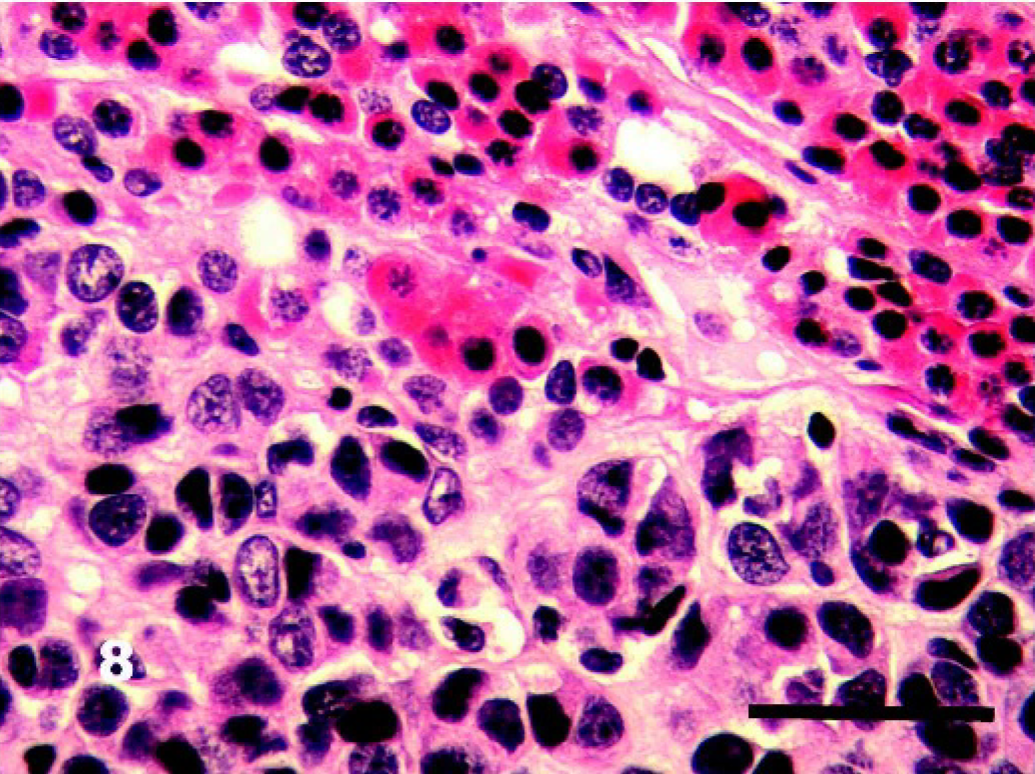
Pituitary gland; Tasmanian Devil. DFTD metastasis in the pituitary gland. The mass is well circumscribed. HE. Bar = 25 μm.
Special stains applied to DFTD cells failed to demonstrate the presence of acid mucins, insulin, melanin, reticulin, glycogen, metachromatic granules, or elastin. Some DFTD cells demonstrated faintly staining accumulations of ribonucleic acid. Small amounts of delicate collagen were interspersed between clumps of DFTD cells.
A database search for cases of S. harrisii submissions to TAHL between 1982 to 2000 indicated that the first case of DFTD occurred in 1997, when 1 case of DFTD was seen. Archived materials at ARWH and San Diego Zoo showed no lesions resembling DFTD (K. Rose and B. Rideout, personal communication).
TEM results
DFTD cells were round and measured 8.08 ± 1.43 μm in diameter (Fig. 9). Cells occurred in clusters of 4–6 with neighboring clusters in close proximity, separated by scant collagen fibers. DFTD cells had single, round, centrally located nuclei (5.75 ± 1.02 μm in diameter) that contained scattered condensed chromatin. Nuclear membrane profiles were undulated. The density of organelles was low and included rough endoplasmic reticulum, free ribosomes, and polyribosomes. Cytoskeletal filaments were observed, but were not dominant. There were large vesicular mitochondria (Fig. 9), some ribosome-lamella complexes (Fig. 9a), secretory granules (Fig. 9b), endocytotic vesicles, well developed golgi apparatus, centrioles, and myelin bodies (Fig. 9c). Low numbers of small desmosome-like elements at apposed plasma membranes were observed (Fig. 9d). Mitotic figures were variable. Occasionally, plasma cells, lymphocytes, and fibroblasts were mingled within the framework of the tissue.
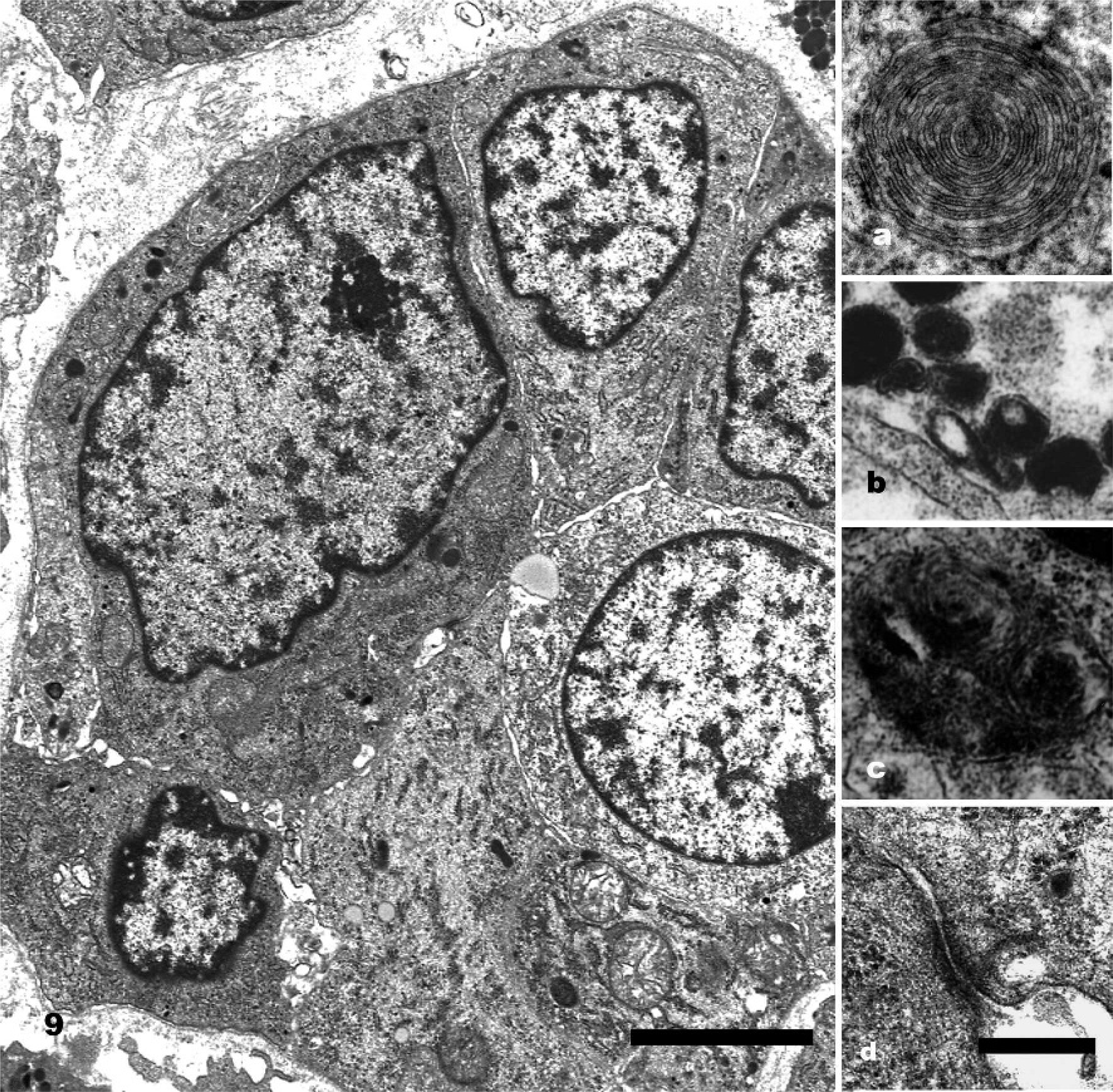
DFTD cells; Tasmanian Devil. Transmission electron micrographs showed large round cells closely apposed. They have single, large, round nuclei with a scattering of clumped chromatin. Bar = 4 μm.
Discussion
Microscopic analysis confirmed DFTD tumors to be an aggressive, poorly differentiated malignant round cell neoplasm primarily affecting the facial regions of the body with frequent metastatic spread to regional lymph nodes and visceral organs. The presence of a pseudocapsule in tumors within the skin is probably caused by rapid growth compressing surrounding connective tissue rather than neoplasm-induced fibroplasia. 2 The consistency of predilection sites as well as similar microscopic and ultrastructural features from many cases led to the conclusion that DFTD neoplasms are derived from one cell type.
DFTD cells appeared too anaplastic to have any specialized functional activity. Most cells had few specialized cellular organelles. Ultrastructural features that were present in a small number of cases were ribosome-lamellar complexes (Fig. 9a) and secretory granules (Fig. 9b). Myelin bodies (Fig. 9c) were also present in a small percentage of cells from some tumors. The presence of desmosome-like structures (Fig. 9d) provide evidence refuting the initial diagnosis of lymphoma. 6 This explained the tendency for cells to clump in cytologic preparations (Fig. 3) and for their characteristic histologic architecture (Fig. 4). However, the scarcity and primitive appearance of the desmosomes were not enough evidence to classify DFTD as a carcinoma.
The propensity for DFTD to arise in the lips, oral mucosa, or the face of Tasmanian Devils and the frequent “jaw wrestling” 10 leads to the hypothesis that DFTD may be spread by fighting or biting. This “allograft theory” may explain many features of the outbreak because it appears highly improbable that the same tumor type could originate spontaneously in multiple geographic locations. Transmissibility of the tumor cells per se must be assessed to ascertain whether it satisfies Koch's postulates.
Griner 3 stated that neoplasia was one of the most common diseases found in S. harrisii at San Diego Zoo, with neoplasms occurring in as many as 50% (9/18) of submissions compared to a much lower prevalence of 2% (7/350) in other marsupials. 3 However, all the neoplasms described by Griner 3 were of epithelial origin, with the exception of one case each of leiomyoma and lymphosarcoma. 3
The first case of DFTD, which occurred near Bredport in the northeast in 1997, was initially diagnosed as a round cell tumor. The neoplasm was sampled from the commissure of the lips and the histomorphology was within the spectrum seen in DFTD. Another 2 cases were examined in 2001, 3 cases in 2002, 18 cases in 2003, and 68 cases in 2004.
Generally, neoplasia is more prevalent in aged animals, 3, 4, 8, 9 and a review of archived materials did recover other forms of neoplasia in S. harrisii, but these occurred in animals older than 4 years. In contrast, more than 95% of DFTD cases were diagnosed in animals between 2 and 4 years of age. In Griner's study, 3 there was a greater proportion of females affected than males, however, there was no gender bias with DFTD.
For unknown reasons, S. harrisii were anecdotally less numerous around 1863 and in 1908–1920. 5 Whatever the reason for their decline, the species recovered, peaking in numbers by 1960, 5 and articles were even published on control methods for these “apparent vermin.” 5 No evidence has been found of DFTD-like disease in past literature or in the archived materials. The absence may be because of the collection criteria for specimens of this period. No viral particles have been identified in tissues from 12 cases (29 sites) of DFTD (A. Hyatt, personal communication). However, it is still too soon to dismiss a viral etiology.
This study has demonstrated, based upon morphology, the classification of DFTD as an undifferentiated soft tissue neoplasm. Further classification of the neoplasm using molecular and/or immunohistochemistry techniques will help to further differentiate the cell of origin.
Footnotes
Acknowledgements
This work has been supported by the Tasmanian State Government and the Australian Wildlife Health Network. The collection of samples throughout the project was heavily supported by colleagues at the Resource Management Branch and private veterinary clinicians at veterinary clinics in Launceston, Montrose, Kingston, Smithton, Penguin, Devonport, and Longford as well as wildlife parks. Testing was performed at Mt Pleasant Laboratory and Royal Hobart Hospital, Tasmania; Murdoch University, Western Australia; University of Sydney, New South Wales; and the Australian Animal Health Laboratory, Victoria. We would like to thank Catherine Marshall, Alex Hyatt, Jamie Chapman, Andrew Parker, Gerard Spoelstra, Michael Slaven, and Peter Fallon for assistance with histologic and electron microscopic examination and interpretations. We are also grateful to the staff at the Queen Victoria Museum and the Tasmanian Museum and Art Gallery for allowing us to examine archived materials. We are indebted to Phil Ladds, Brad Chadwick, Roy Mason, Ray Lowenthal, Bruce Jackson, David Obendorf, and Susan Hemsley for providing data and feedback on the results. We also wish to extend our gratitude to Phillip Clark for advice on the cytology section.