
Abstract
A 7-year-old, female, domestic medium-haired cat had a recurrent deep dermal mass in the interscapular region after initial surgical removal 3 months earlier. The cat had received a killed rabies vaccine and a five-in-one vaccine in the same area about 2 months prior to the first surgery. The relapsed mass was diagnosed as vaccine-associated sarcoma. The cat was euthanized 2 months later because of hind limb paralysis. At necropsy, multiple, poorly demarcated, nodular masses were seen in the muscles around the shoulders, neck, and thoracic vertebrae. Pulmonary metastasis and spinal epidural invasion at T1–T3 with regional cord compression and malacia were observed. Microscopically, the masses consisted of interwoven bundles of spindle cells with prominent multinucleated giant cell formation. The neoplastic cells stained strongly positive for myoglobin, and moderately but variably positive for vimentin, desmin, and α- smooth muscle actin. Phosphotungstic acid-hematoxylin staining revealed cytoplasmic striations in scattered tumor cells. The tumor was considered a vaccine-associated rhabdomyosarcoma.
Feline vaccine-associated sarcoma (VAS) was initially recognized in the late 1980s after the enactment of the Pennsylvania state law requiring rabies vaccination of cats in 1987. This type of sarcoma typically is present in vaccination sites, especially the cervical and interscapular regions, where it develops 3 months to 11 years after vaccination. 9 Vaccine-associated sarcoma is most commonly classified as fibrosarcoma, although rhabdomyosarcoma, myxosarcoma, chondrosarcoma, malignant fibrous histiocytoma, and undifferentiated sarcoma also have been rarely reported. 1, 5 These sarcomas are locally invasive and have a high rate of local recurrence. 3, 4 Metastasis is reported more commonly in the lungs, 13 and has also been seen in the pleura, mediastinum, pericardium, kidney, and pelvic canal. 2, 3, 13 To our knowledge, there have been no detailed reports of vaccine-associated rhabdomyosarcoma and spinal epidural invasion. A case of feline vaccine-associated rhabdomyosarcoma with spinal epidural invasion and pulmonary metastasis is described herein.
A 7-year-old, spayed female, domestic medium-haired cat had been on a regular vaccination program since she was young. The cat had received a deep intramuscular injection of a killed rabies vaccine and a killed five-in-one vaccine for feline rhinotracheitis, panleukopenia, calicivirus, pneumonitis, and leukemia in the interscapular region. Two months later, a mass was found at the vaccination site and was removed, but it recurred locally 3 months later. The recurrent mass measured 6.0 × 4.0 × 3.0 cm, was yellow-white, firm with central necrosis, and was tightly attached to the adjacent muscles. The tumor was diagnosed as VAS with incomplete excision. The cat was euthanized 7 months after vaccination because of hind limb paralysis and poor prognosis.
At necropsy, five 0.3- to 1.0-cm, poorly demarcated, red nodules were observed on the fascia of the superficial muscles of both shoulders. A 1.5 × 2.5 × 3.0 cm poorly demarcated, yellow-white mass with central hemorrhage was found in the rhomboid muscle of the right scapula. Two masses, measuring 0.4 × 0.5 × 1.1 cm and 0.8 × 1.2 × 1.4 cm, were found in the distal region of the deltoid muscle near the acromion process of the left scapula. A 0.5-cm-diameter mass was seen at the right side of the longissimus muscle of the neck over the seventh cervical vertebra (C7). A 0.4 × 0.5 × 0.8-cm mass was present in the longissimus muscle of the thorax at the left side of the second thoracic vertebra (T2), and three more 0.8- to 1.2-cm masses were found in the same muscle at the right side of the T1–T3 region. After longitudinal dissection of the vertebrae from the ventral aspect, two pale-white flat masses, approximately 0.7 × 0.4 cm and 0.3 × 0.4 cm, were seen attached to the dorsal aspect of the vertebral canal at the intervertebral region of T1/T2 and T2/T3, respectively (Figs. 1, 2). The locations of the epidural masses corresponded to those masses in the longissimus muscle of the thorax at the right side of T1–T3. The epidural mass at T1/T2 caused compression of the spinal cord, resulting in regional malacia (Fig. 1). In addition, multiple randomly distributed 0.05- to 0.5-cm, white nodular masses were observed in the lungs.
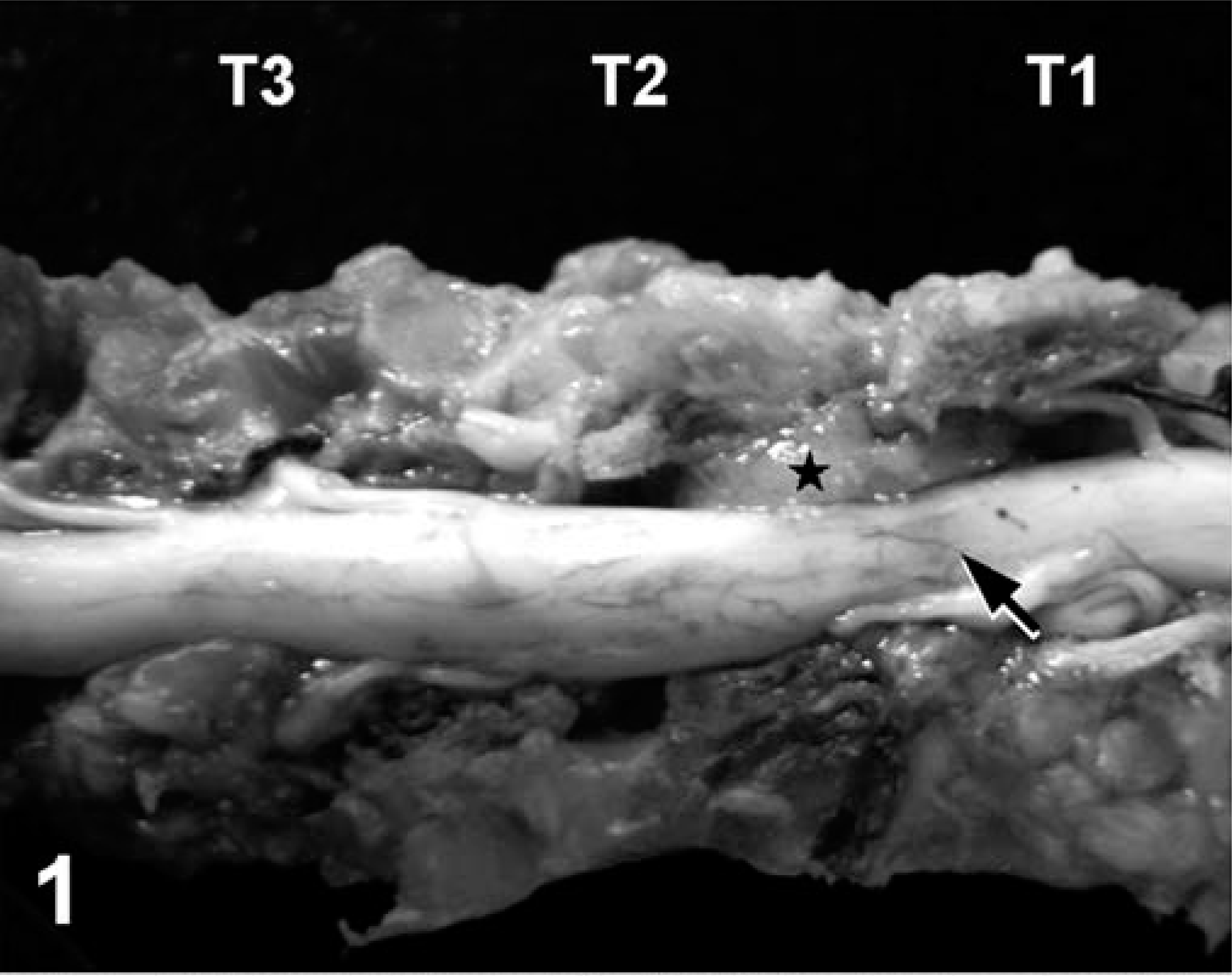
Ventral aspect of the longitudinally opened vertebral canal between T1 and T3; cat. The epidural mass at T1/T2 (∗) causes severe compression to the regional spinal cord (arrow).
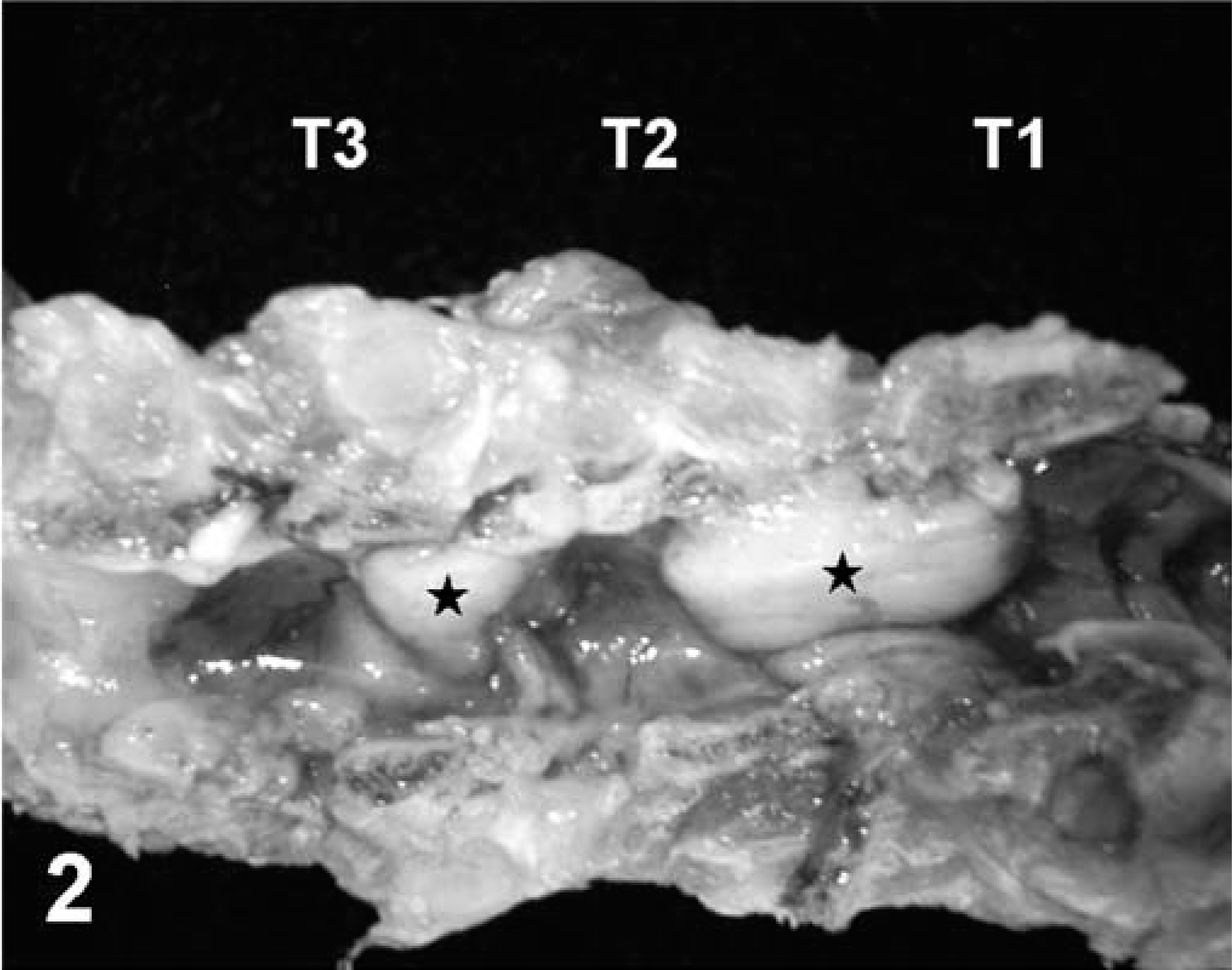
Dorsal aspect of the longitudinally opened vertebral canal between T1 and T3 after spinal cord removal; cat. Notice two pale-white epidural masses (∗) attached to the dorsal area of the vertebral canal at the junctions of T1/T2 and T2/T3.
Grossly, the tumor masses were poorly demarcated from the surrounding muscles by an incomplete fibrous capsule. Microscopically, they consisted of bundles of slender or plump spindle cells that were often arranged in a storiform or interwoven pattern. They also contained many variably sized and shaped giant cells (Fig. 3), with up to 40 nuclei. The tumor cells had oval-to-elongated, polygonal, hyperchromatic, often centrally located nuclei surrounded by abundant, partially distinct, eosinophilic, granular cytoplasm. Mitotic figures were common, ranging from two to eight per high-power field (400×), and atypical- to-bizarre mitoses were frequently observed. Vascular and lymphatic invasions were often seen. Areas of infiltration with neutrophils, lymphocytes, and plasma cells, as well as areas of necrosis, also were present. The epidural and pulmonary metastatic masses also consisted of spindle cells and multinucleated giant cells, similar to those seen in the back and neck. Tumor emboli were observed in some pulmonary arteries and lymphatics. Vertebral invasion by the epidural masses with osteolysis was apparent. Tumor invasion was not seen in the spinal cord. At the site of cord compression at T1/T2, white and gray matters were malacic, evidenced by vacuolization, liquefactive necrosis, and presence of gitter cells.
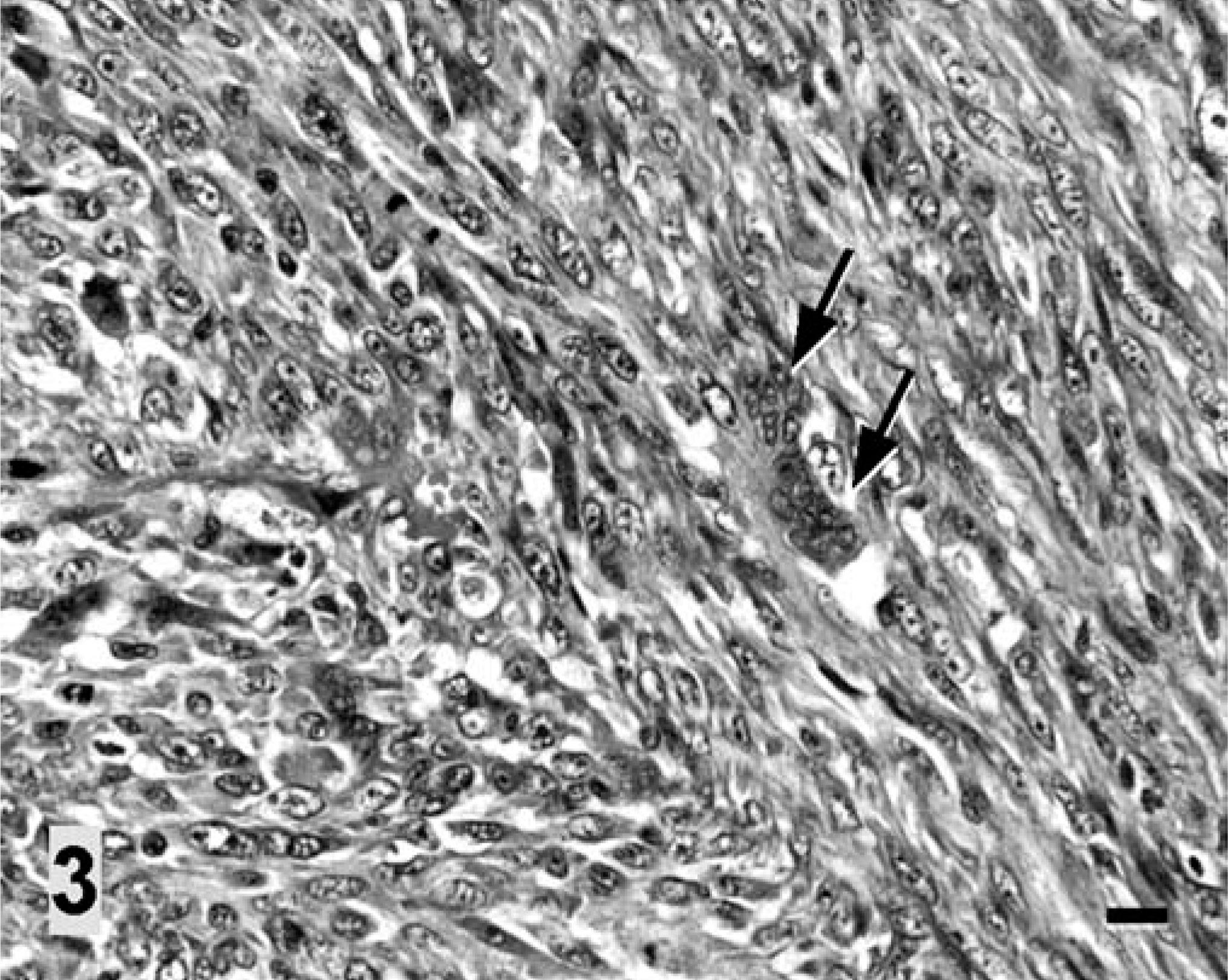
Vaccine-associated rhabdomyosarcoma, interscapular region; cat. The tumor mass contains interwoven bundles of spindle cells with formation of multinucleated giant cells (arrows). HE. Bar = 40 µm.
Immunohistochemical staining, using a 1 : 50 dilution of mouse antiporcine vimentin (Dakocytomation, Glostrup, Denmark), a 1 : 100 dilution of mouse antihuman desmin (Biomeda, Foster City, CA), a 1 : 50 dilution of mouse anti-human myoglobin (Biomeda), a 1 : 100 dilution of mouse antihuman smooth muscle-specific α-actin (α-SMA; Dakocytomation), a 1 : 100 dilution of rabbit antihuman S-100 protein (Dakocytomation), and a 1 : 50 dilution of rabbit antihuman glial fibrillary acid protein (GFAP; Biomeda), was performed on formalin-fixed, paraffin-embedded tissues by use of the avidin-biotin complex method (Vectastain Kit, Vector Laboratories, Burlingame, CA). Diaminobenzidine chromagen (DAB; Sigma Chemical Co., St. Louis, MO) was used as the substrate. Tissue specimens of skeletal muscle, myocardium, uterus, and urinary bladder from the present case and from other cats were used as negative and positive controls for immunostaining. Most neoplastic cells stained strongly positive for myoglobin (Fig. 4), and some stained moderately but variably positive for desmin, α-SMA, and vimentin; however, staining of the tumor cells was completely negative for S-100 and GFAP. Phosphotungstic acid-hematoxylin (PTAH; Muto Pure Chemicals, Tokyo, Japan) staining demonstrated cytoplasmic striations in scattered tumor cells (Fig. 5). These staining results for the tumor cells were strongly suggestive of a skeletal muscle origin.
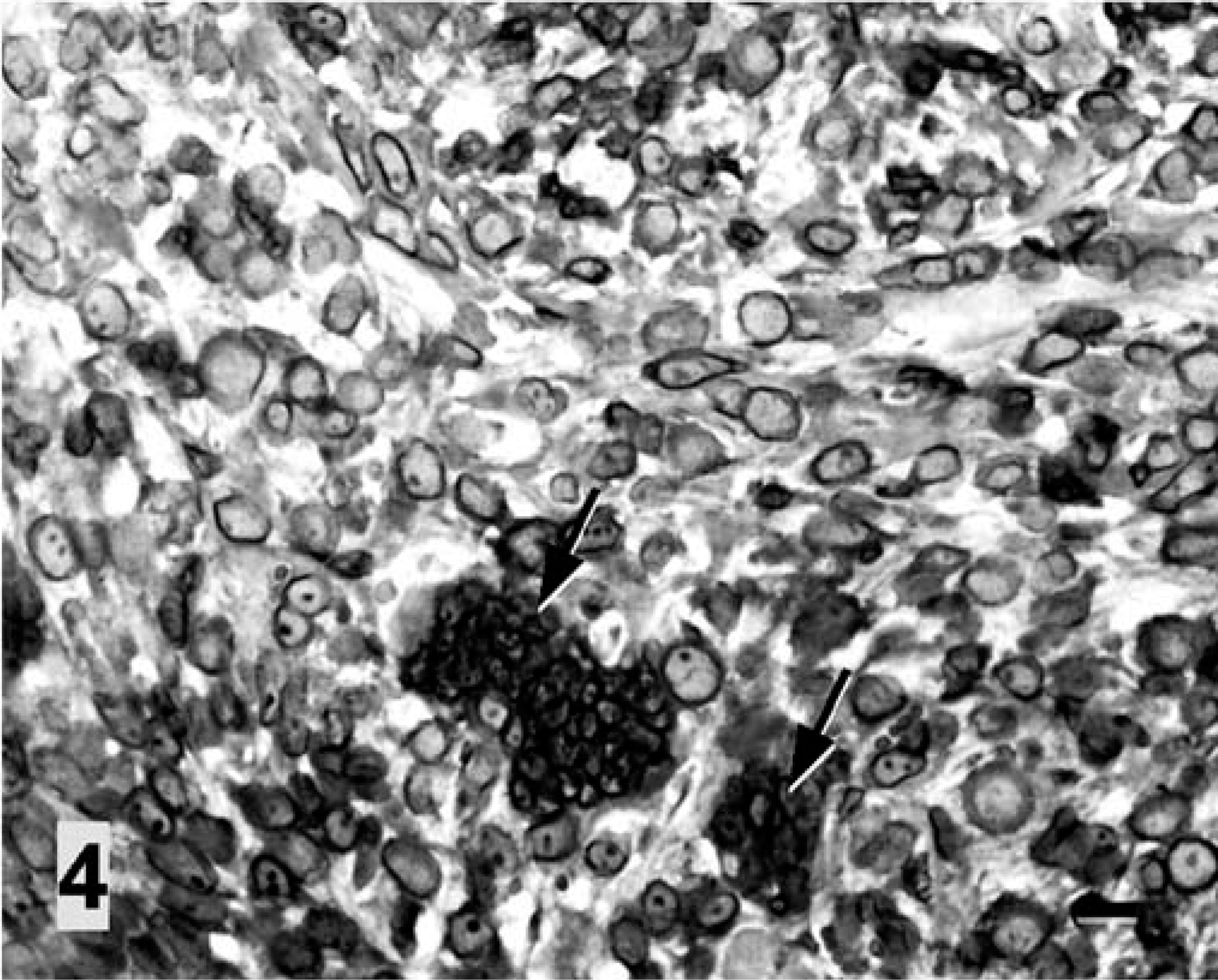
Vaccine-associated rhabdomyosarcoma, interscapular region; cat. Most tumor cells, including multinucleated giant cells (arrows), stain strongly positive for myoglobin. Avidin-biotin complex immunoperoxidase method, with diaminobenzidine as chromogen and hematoxylin as counterstain. Bar = 20 µm.
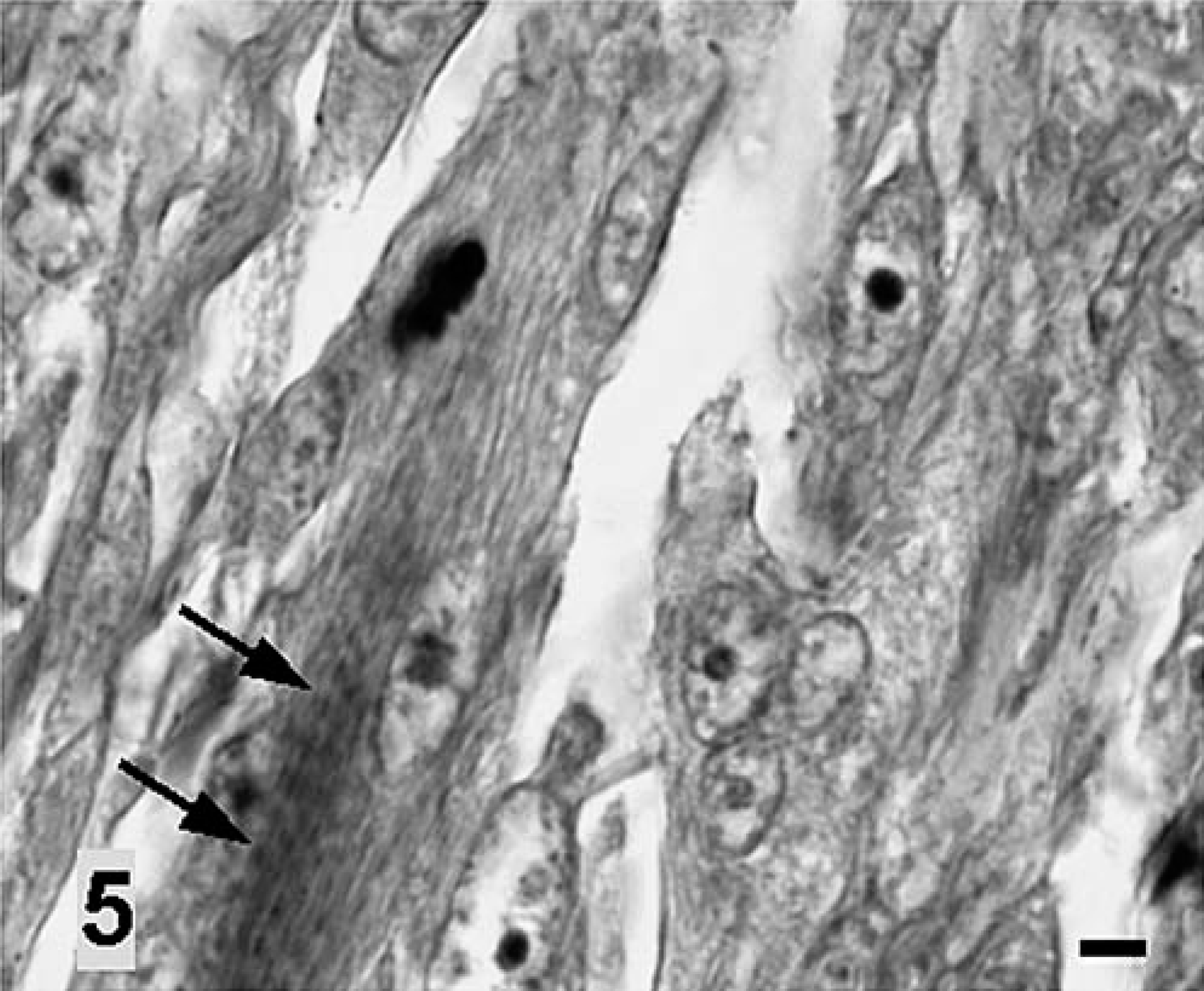
Vaccine-associated rhabdomyosarcoma, interscapular region; cat. Some tumor cells show less well developed cross-striations (arrows) indicative of skeletal muscle differentiation. Phosphotungstic acid-hematoxylin. Bar = 5 µm.
The history of vaccination, location of tumor, and histologic characteristics of the cat of this report were consistent with VAS. Similar to those of previous reports, 1, 10 the immunolabeling and histologic findings of the tumor also were suggestive of a mesenchymal origin. The positive staining results of tumor cells with desmin, vimentin, and α-SMA were consistent with VAS of the myofibroblastic phenotype. 1, 2 However, the strong myoglobin reaction in most tumor cells and documentation of cross-striations in the cytoplasm of highly pleomorphic tumor cells suggested that the tumor could be further classified as a rhabdomyosarcoma. 10
The exact pathogenesis of feline VAS is still uncertain, and likely is multifactorial. From earlier studies, it was suggested that aluminum adjuvant, special antigen types, or particular vaccine brands are associated with VAS in cats. 4, 7, 8 Sarcomas reported in posttraumatic eyes, in uteruses with long-standing pyometra, and in injection sites of medications such as long-acting penicillin and methyl prednisolone acetate, however, also suggested that inflammation might be an important element in the development of VAS in cats. 6, 7 The uniquely high susceptibility to oxidative injury in cats, such as Heinz body anemia and acetaminophen toxicity, also has been suggested as a cause for the induction of VAS. 9 Transforming growth factor alpha (TGF-α) and granulocyte-macrophage colony-stimulating factor produced by activated macrophages are considered to contribute to the malignant transformation of mesenchymal cells into fibroblastic or fibromyoblastic VAS in cats. 1 More recently, it also was suggested that basic fibroblast growth factor, P53 protein, and TGF-α participate in the pathogenesis of VAS. 11
In the cat of this report, multinucleated giant tumor cells were easily found, not only in the recurrent intramuscular tumor masses but also in the epidural and pulmonary metastatic tumor masses. It has been suggested that the recurrence and metastasis of VAS are correlated with the frequency of multinucleated giant cells in the lesion, which is indicative of a poor phenotypic differentiation and poor prognosis. 1
The presence of tumor emboli within the vascular and lymphatic lumina of the lungs is indicative of the cancer's routes of metastasis. On the other hand, the epidural masses likely were derived from local invasion of the masses in the longissimus muscle of the thorax at the right side of T1–T3 via the neural foramen or intervertebral space into the vertebral canal. The gradually enlarging epidural mass compressed the regional spinal cord progressively in a partial circumferential manner, subsequently causing hind limb paralysis in this cat.
This case re-emphasizes the high risk of tumor development in cats following repeated vaccinations in the same region. Current recommendations to avoid VAS include vaccination in the distal portion of the extremities, prevention of further metastasis by radical amputation of tumors, and avoidance of repeated injections in the same region. 12