
Abstract
A 6-month-old female German Shepherd Dog died as a result of profuse oral bleeding. At postmortem examination, the oral cavity showed visible roots of the right mandibular fourth premolar and first molar teeth and, in addition, they were very mobile and compressible. Radiographs showed a generalized radiolucency in the body of the right mandible, with evidence of resorption of the affected alveolar bone. Histologically, the lesion of the right mandible was characterized by the lysis of bony structures and a non-malignant proliferation of blood-filled vascular spaces lined by a single layer of well-differentiated endothelial cells. The clinical, radiographic, and histologic presentation of this dog is consistent with that associated with Gorham-Stout disease, a rare bone disorder in humans.
A 6-month-old female German Shepherd Dog initially presented to the Hospital Veterinario Rof Codina for intermittent oral bleeding without a history of significant trauma or discomfort. Physical examination showed the presence of fractured and mobile lower right canine and first premolar deciduous teeth with accompanying gingival hemorrhage. After extraction of the fractured teeth and surgical suture, bleeding apparently stopped. Five weeks after the initial presentation, the dog was returned to the Hospital with acute oral bleeding. The laboratory data showed hematocrit and hemoglobin readings of 8.1% (reference range, 37–55%) and 2.5 g/dl (reference range, 12–18 g/dl), respectively; coagulation parameters were within normal laboratory ranges. Bleeding originated from the gingiva around the teeth of the right mandible, but attempts to arrest it were unsuccessful because the exact source of the hemorrhage could not be identified. In spite of the prescribed treatment and transfusion of whole blood, the dog died.
At postmortem examination, gross pathologic findings were limited to the body of the right half of the mandible. The roots of the fourth premolar and first molar teeth were readily visible because of marked gingival recession accompanied by an enlargement of the bony alveoli (Fig. 1). Both teeth were very mobile, and when compressed, they introduced deeply into the body of the mandible. There was no associated gingivitis. Dissection of the mandible showed a loss of the affected alveolar and adjacent bone and, in addition, an area of absence of cortical bone of 1 cm in diameter in the lateral surface of the right mandibular body, ventral to the third premolar. The affected mandibular bone showed no nodules or enlargement, and no abnormalities were identified at the rostral extremity of the body and ramus of the right mandible or at the left half of the bone. These postmortem findings indicated direct trauma to the inferior alveolar vessels of the right mandibular canal by the mobile teeth as the origin of the hemorrhage.

Right mandible; dog. Marked gingival recession. Visible roots of the fourth premolar and first molar.
The dissected mandible was thereafter subjected to a radiographic study. Radiographs demonstrated a large area of bony lysis involving the body of the right half of the mandible from the canine tooth to the second molar. Bone loss was particularly evident around the fourth premolar and first molar teeth, which showed partial root resorption and enlargement of the bony alveolus (Fig. 2). No bony sequestra or periosteal reaction was present to indicate osteomyelitis. The ramus and rostral portions of the right half of the mandible, as well as those of the left half of the mandible, showed no radiographic changes.

Radiograph of mandibular specimens; dog. The body of the right mandible (top) shows a large area of bony lysis that involves the canine teeth to the second molar. The premolar and molar teeth show partial root resorption (arrows). No radiographic changes are evident in the left half of the mandible (bottom).
After radiographic evaluation, representative samples of both the normal and affected portions of the mandible were fixed in 10% neutral-buffered formalin. Some portions were first decalcified and then embedded in paraffin according to standard laboratory procedures. Other undecalcified portions were embedded in resin (Technovit 7200 VLC; Exakt Technologies, Inc., Oklahoma City, OK) and processed by the cutting-grinding method. 3 Final sections obtained from both procedures were stained with hematoxylin and eosin and Levai Laczko staining techniques. Histologically, the right half of the mandible showed an evident replacement of bone by an extensive network of thin-walled, endothelium-lined vascular channels of varying size, many of them of the cavernous type, which were filled with red blood cells or organizing thrombi Figs. 3, 4). Endothelial cells were flat and typical in appearance, showing no anisocytosis or anisokaryosis, and mitotic figures among them were not observed. The vascular mass lacked foci of solid growth and papillary projections of endothelial cells. Large areas of hemorrhage were also observed in the loose connective tissue that supported the vessels. There was no evidence of inflammation. The remaining cortical and trabecular bone was thin, and numerous osteoclasts were identified at the interface between the vascular tissue and bone (Fig. 4). On the basis of the morphologic and radiographic findings, a diagnosis of hemangiomatosis associated with osteolysis of the right mandibular body was made.
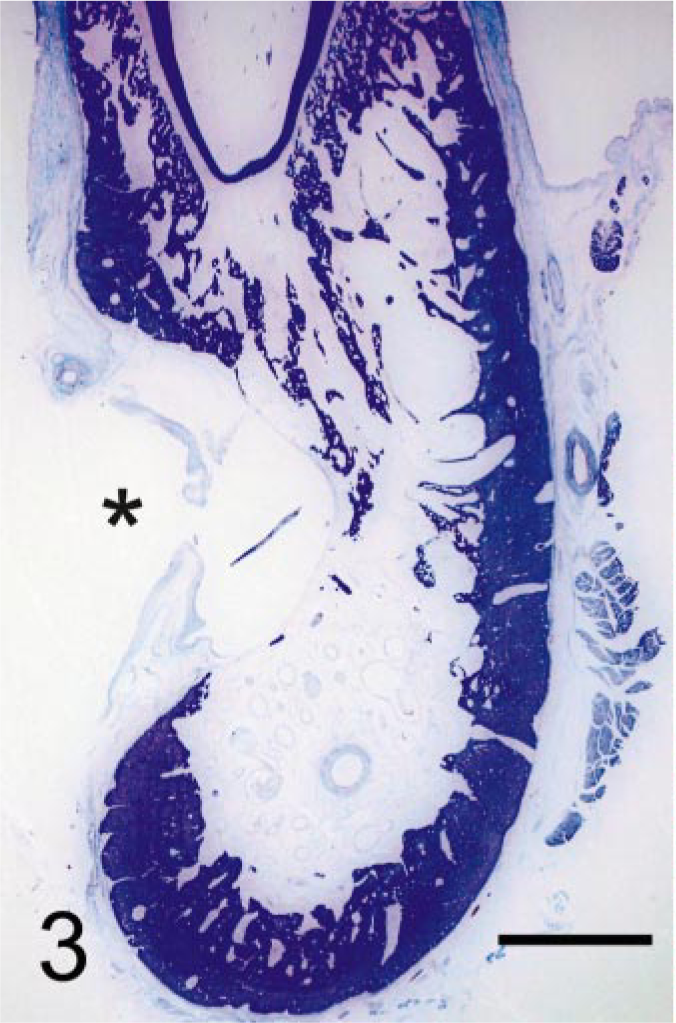
Right mandibular body; dog. Loss of the alveolar and adjacent bone and absence of cortical bone (asterisk) in an area of the lateral surface. Levai Laczko. Bar = 3.5 cm.
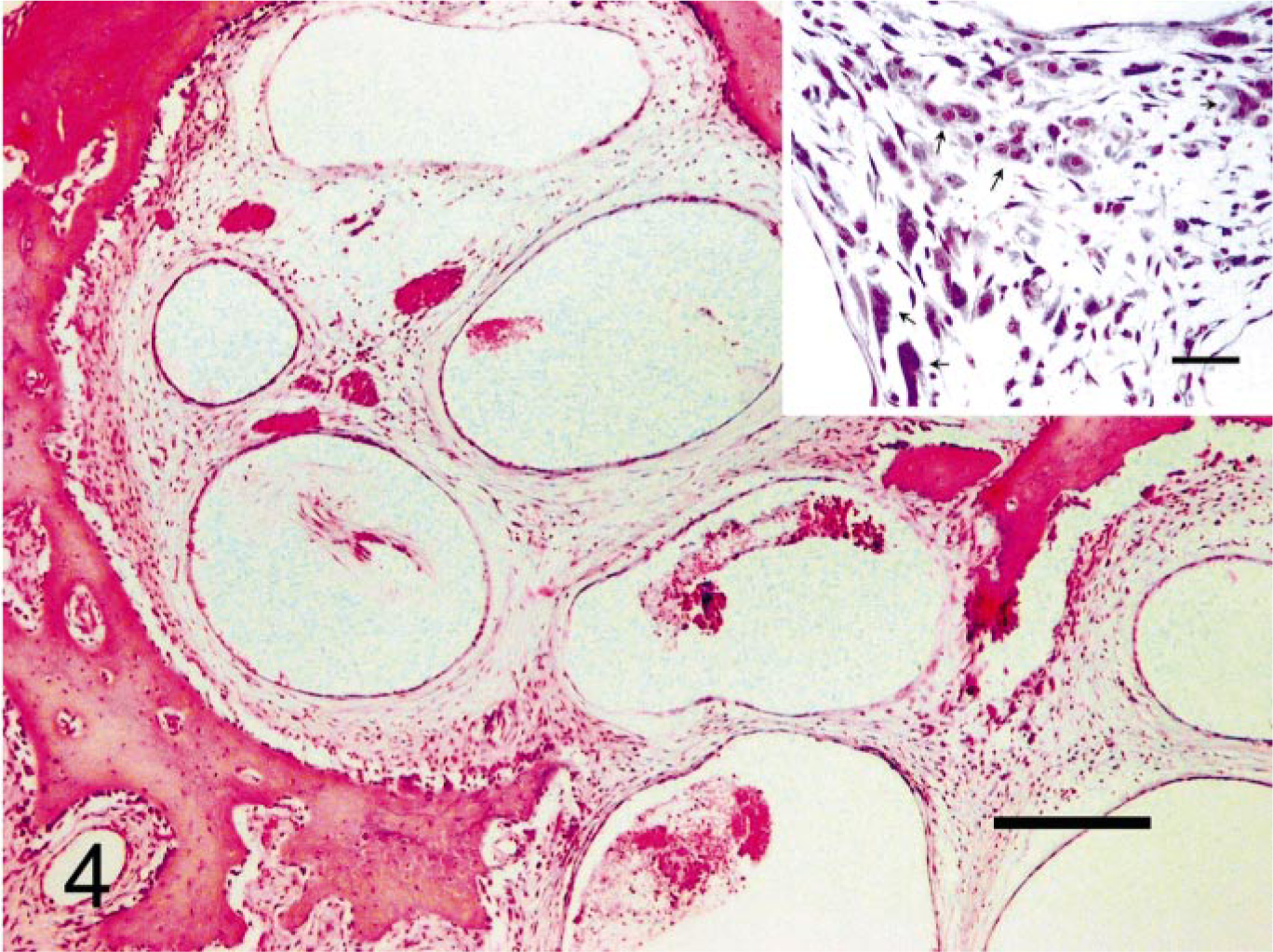
Right mandible; dog. Nonmalignant proliferation of blood-filled vascular spaces lined by a single layer of well-differentiated endothelial cells. HE. Bar = 200 μm. Inset: Numerous osteoclasts (arrows) at the interface between the vascular tissue and bone. HE. Bar = 30 μm.
As a differential diagnosis, primary hemangioma of the bone had to be excluded. Osseous hemangioma is a very rare tumor in domestic animals. A few cases have been found in the skull, mandible, vertebral column, and long bones of young-to-middle-aged dogs and cats and in a colt. 4, 6 This vascular tumor can usually be diagnosed because local swelling is present in the involved bone, lameness is noticed when the tumor is located at the appendicular skeleton, and, although the cortex is usually preserved, sometimes a fracture is observed due to the reduced thickness of the cortical bone. Hemangiomas of the flat bones of the skull tend to produce a reactive periosteal bone formation with a sunburst appearance on radiographs. Microscopically, the tumor has been described as a multilobular expansile mass composed of thick- or thin-walled vascular channels, with a mixed venous and cavernous appearance, which are lined either by typical or by neoplastic endothelial cells, and with a reactive periosteal bone formation. In the dog presented in this study, the affected mandibular bone showed no enlargement or periosteal bone deposition. In addition, the vascular lesion was poorly defined and did not appear to be involved with the destruction of bony structures by an expansile growth; rather, cortical and cancellous bone loss seemed to be associated with an increase in osteoclast activity, since numerous osteoclasts were identified on the surfaces of the remaining bone. Finally, the vascular channels and their supportive connective tissue showed no features of malignancy. Taking into account these considerations, we prefer to maintain the diagnosis of hemangiomatosis associated with osteolysis over that of hemangioma.
The reports of Gorham-Stout disease in humans have many similarities to those in the dog presented in this study. Gorham-Stout disease (synonyms: massive osteolysis, vanishing or disappearing bone disease, and phantom bone disease) is a rare disorder characterized by a nonfamiliar, histologically benign vascular proliferation originating in bone and producing progressive resorption of all or a portion of the bone. 2 This uncommon condition occurs sporadically and is most often observed in children and young adults of either sex. Involvement of almost every bone has been reported, although there is a predilection for bones that develop by intramembranous ossification, with the shoulder girdle and mandible being the most common bones affected. The lesion is typically nonexpansile and nonulcerative and is usually monocentric but locally aggressive, with resorption of the affected bone. The vascular lesion may spread into soft tissue and contiguous bones. 1, 2 The pathogenesis of Gorham-Stout disease remains unknown, although it has been suggested that there is an increase in the sensitivity of osteoclast precursors to humoral factors, which promote osteoclast formation and bone resorption and operate at the level of the bone microenvironment. 5
In summary, this study describes a dog with massive osteolysis of the right mandibular body associated with a non-malignant proliferation of vascular channels, a clinical and morphologic presentation closely resembling Gorham-Stout disease in humans.
Footnotes
Acknowledgements
We thank Dr. Jesús Alba (Histobiomol, S.L., Lugo, Spain) for his helpful suggestions about this dog.