
Abstract
A 5-year-old female neutered Boxer dog was diagnosed with extensive odontogenic cysts that affected the left and right mandibles. Rostral mandibular swelling was detectable clinically, and bilateral cystic mandibular lesions were identified radiographically. The dog's owners elected for euthanasia. A full postmortem was performed. Cystic cavities were confirmed in the body of each mandible, extending from the incisor teeth to the mid premolar region. Incisor, canine, and premolar tooth roots indented each cavity. Histologic examination of the cystic cavities reflected an inner lining of attenuated stratified squamous epithelium overlying a fibrous layer infiltrated by a mixed, predominantly mononuclear, inflammatory infiltrate.
Clinically significant cysts of the jaw are rare in domestic animals. 6 Odontogenic cysts arise from tissues that give origin to the teeth. Reported odontogenic cysts include radicular cysts, dentigerous cysts, and keratocysts. 4 Radicular cysts are the most common type of oral cyst in humans 7 but have only been reported 3 times in the dog. 2,4,10 The purpose of this paper is to report bilateral odontogenic cysts, in the mandible of a dog, that are difficult to fully characterize within current classification schemes.
A 5-year-old, female, neutered Boxer dog was presented to the University of Bristol after a 3-week history of a mass affecting the rostral mandibular region. An incisional biopsy specimen of the gum adjacent to the site of the right lateral incisor tooth had been obtained by the referring veterinary surgeon 3 weeks previously. This tissue was submitted to another institution and reported as representing either a basal-cell carcinoma (acanthomatous epulis) or part of a true odontogenic cyst, although the sample was too superficial to further characterize. The mass was located between the right mandibular canine tooth and the adjacent incisors. The right lateral incisor tooth was missing from the mandible. No other teeth were missing. Clinical examination was otherwise unremarkable.
Intra-oral radiography was conducted with the dog under general anaesthesia. The right mandible contained an expansile lytic lesion (Fig. 1), within its rostral part, which extended from the rostral tip of the mandible to the third premolar. There was thinning and, in places, a loss of the abaxial cortex but retention of the rostral and axial cortices. The clear loss of the supporting bone of the teeth in the region was observed. A similar, smaller expansile lesion was present within the left mandible, extending as far caudally as the second premolar. The tooth roots of all incisors, both canines, and the first 2 premolar teeth of each mandible indented the cystic spaces. Treatment options, including bilateral rostral mandibulectomy, were considered. The dog's owners elected for euthanasia, on the basis of the extensive nature of the disease process and consequent poor masticatory function anticipated for this procedure in a brachycephalic breed. A postmortem examination was performed.

Mandible; 5-year-old female neutered Boxer dog. Internal dental radiograph showing bilateral cystic cavities affecting the rostral mandible. The right lateral incisor is absent.
On gross examination, significant changes were confined to the jaw and consisted of bilateral rounded swellings of the rostral mandibles, which were approximately 1.5-cm diameter at that point. On sectioning the mandibles, both contained a cystic space filled with clear fluid. Each space was approximately 1 cm in diameter and approximately 2- to 3-cm long and extended to the incisors at their most rostral borders (Fig. 2). At the site sectioned, a tooth root was observed to indent the cystic space. For histologic examination, the mandible was fixed in 10% neutral buffered formalin. A cross section of the right mandible at the level of the first premolar tooth was then decalcified in 10% formic acid and processed routinely. A section was cut at 5 μ, stained with hematoxylin and eosin and examined by light microscopy. On microscopic examination, the cystic spaces were limited by a rim of fibrous tissue and mixed, predominantly mononuclear, inflammatory cells (Fig. 3). The inner lining of the space was formed by attenuated stratified squamous epithelium. The right first premolar tooth root indented the cyst and was covered by the cyst lining. The tooth root was viable. A histologic diagnosis of bilateral odontogenic cysts was made based on the epithelial lining of the lesions and the close association with the tooth roots.
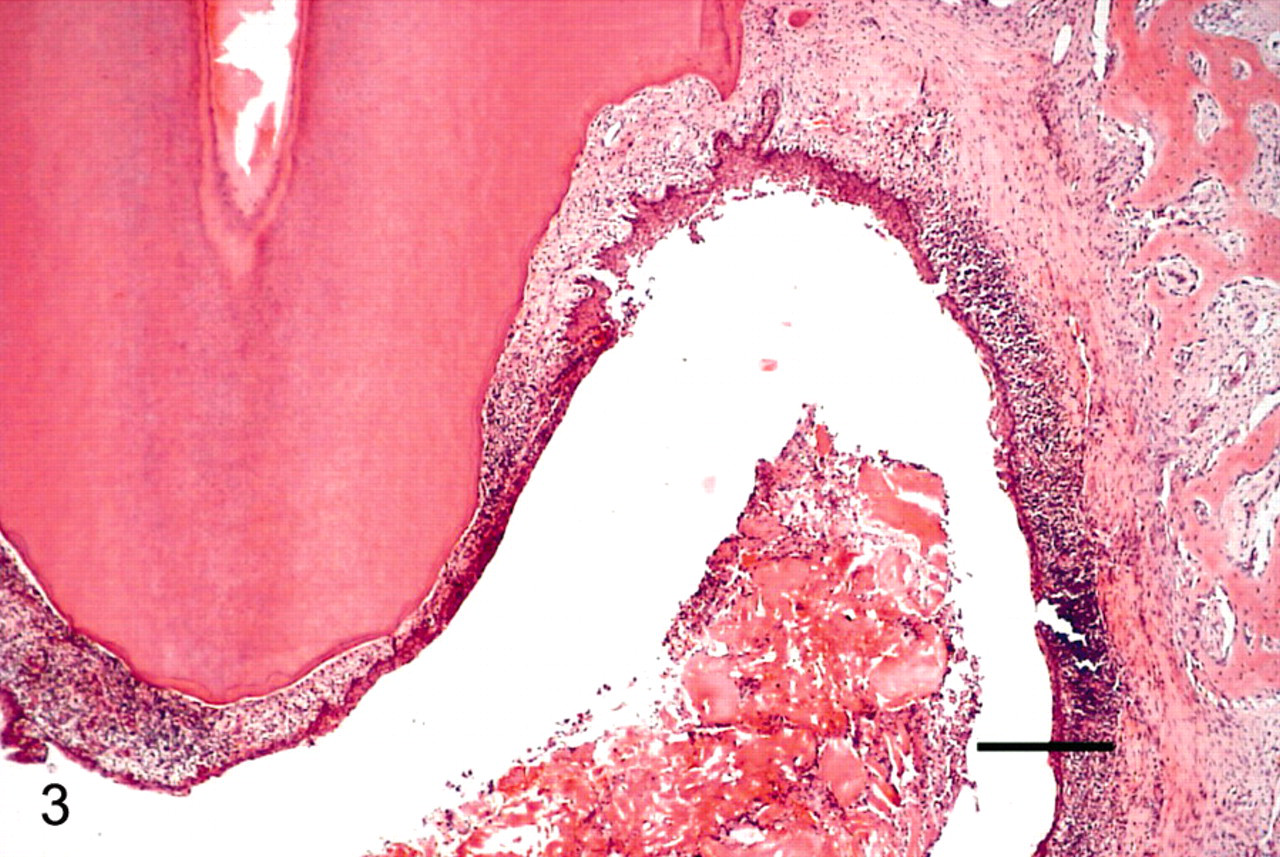
Mandibular cyst lining; 5-year-old female neutered Boxer dog. Photomicrograph image of the transected, right, hemimandible. The tooth root projects into the cyst lumen, which is lined by squamous epithelium. Subepithelial connective tissue is infiltrated with inflammatory cells. Keratin and inflammatory cells can be seen in the cyst lumen. HE. Bar = 300 μ.
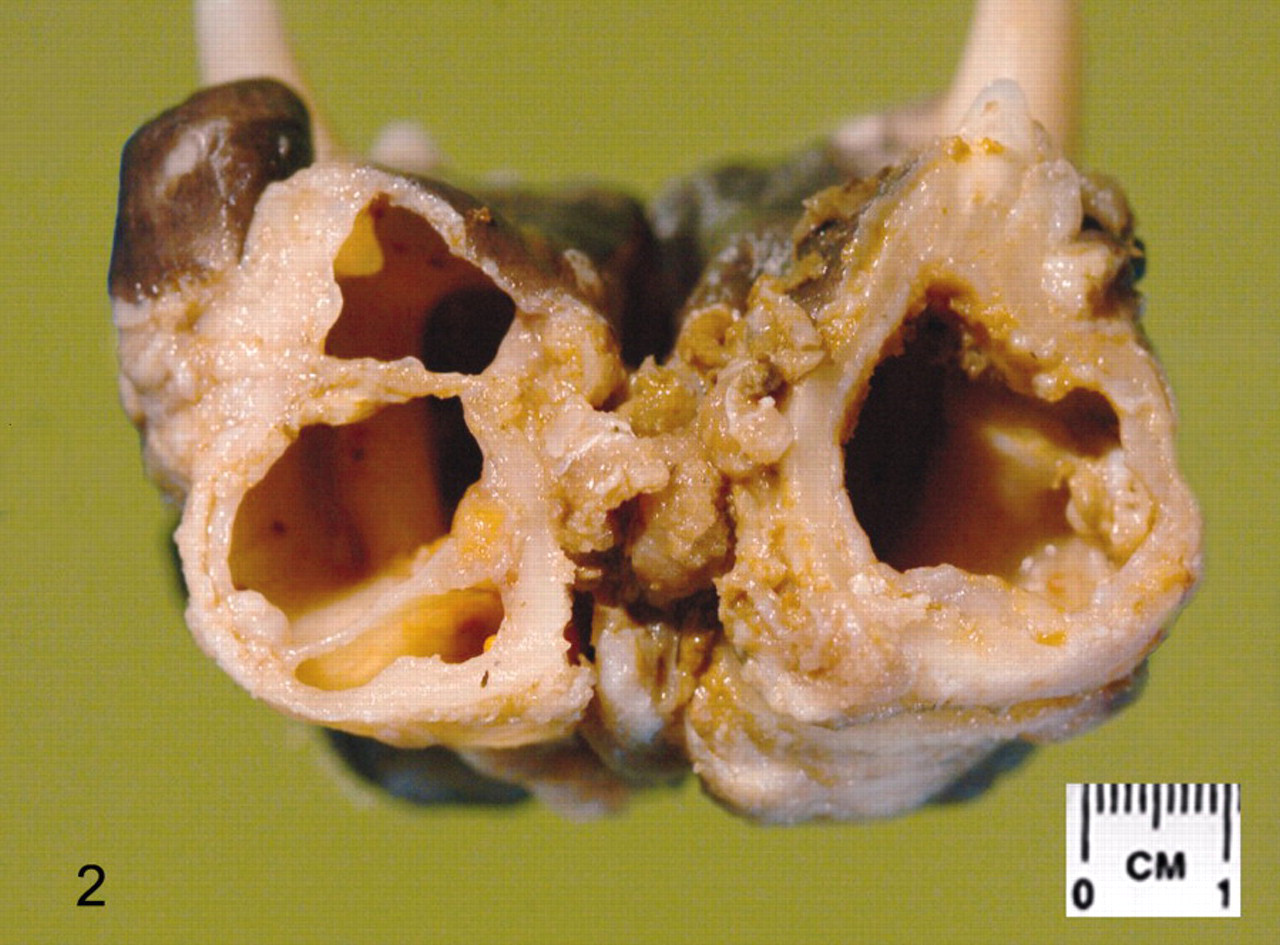
Mandible; 5-year-old female neutered Boxer dog. Photograph of the transected mandible, viewed rostrally, at the level of the first premolar teeth, showing bilateral cysts.
Odontogenic cysts are rare in animals, and some disagreement is associated with their classification. Odontogenic cysts are derived from cell rests of Malassez, cell rests of dental laminae, reduced enamel epithelium, or malformed enamel organs. 1 Types of odontogenic cysts reported in dogs include radicular cysts, dentigerous cysts, and keratocysts. 2,4,8,10,12 In contrast to other odontogenic cysts, radicular cysts are associated with an inflammatory infiltrate. 6 They are also very often found in association with a devitalized tooth. In man, radicular cysts are thought to arise from the cell rests of Malassez, which reside within the periodontal ligament. 11
During embryogenesis, downgrowths from an ectodermal ridge (the “dental lamina”) penetrate the underlying mesenchyme of the embryonic jaw. These ectodermal extensions induce proliferation and differentiation of adjacent mesenchyme, which then develops to form, in conjunction with the ectodermal projections, the dental organs (“tooth buds”). The periodontal ligament is created from mesenchyme-derived fibroblasts. During formation of the periodontal ligament, mesenchymal fibroblasts penetrate an ectodermal membrane called Hertwig's Sheath. This sheath is breached in the apical region of the tooth root and subsequently regresses to leave ectodermal remnants within the newly formed periodontal ligament. These ectodermal remnants are called the epithelial cell rests of Malassez. It is thought that these cell rests are stimulated to form cystic structures in the presence of inflammation and to occur most commonly as a result of chronic apical periodontitis secondary to microbial invasion into the pulp cavity of a tooth. The specific etiology of radicular cysts in the dog remains unclear. Dentigerous cysts are defined as cysts that contain part or all of a tooth, which is often malformed. 1,5 Namely, they occur in association with an unerupted or impacted tooth. 3,9 Among the domestic animals, dentigerous cysts most commonly occur in horses in association with vestigial canine teeth. 1 A characteristic feature of dentigerous cysts is attachment of the epithelium to the tooth remnants at the cemento-enamel junction, with the crown extending into the cyst. 6 Fluid develops between the reduced enamel epithelium and the crown of the tooth. Dentigerous cysts are not associated with an inflammatory infiltrate. Dentigerous cysts do not usually contain keratin, although a keratinizing component may occur as part of a metaplastic process. 9 The cyst lining is reported to be 4 to 6 cell layers thick. 9 Odontogenic keratocysts are also reported to be keratinized, but the epithelial lining, by comparison, is generally 8 to 10 cell layers thick. 9
In the present case, an inflammatory infiltrate was associated with the cyst lining, which is suggestive of a diagnosis of radicular cyst. However, radicular cysts are very frequently associated with a devitalized tooth. 11 No devitalized teeth were identified in this dog. The right lateral mandibular incisor was missing from this patient. It is possible that this tooth was devitalized and represented the origin of a radicular cyst. The cystic lesion of the left mandible does not further clarify the situation because no devitalized or unerupted teeth were identified there. Radicular cysts have not been reported as extensive and bilateral lesions. Therefore, a description of extensive bilateral rostral mandibular odontogenic cysts was applied.
Treatment of odontogenic cysts entails surgical exposure and curettage of the cyst lining. The cavity may then be filled with decalcified freeze-dried bone. Teeth that are loosened or otherwise damaged because of displacement by the cyst, including the pulpless nonvital tooth of cyst origin, are removed if still present. The reported prognosis for odontogenic cysts thus treated is good, with recurrence of the cyst being an uncommon finding. 8 Treatment via curettage was reported in 2 previous cases of radicular cysts in dogs. 2,4 This treatment was judged to be effective, with no disease recurrence found at 6 2 and 14 4 months after surgery. The cysts of the dog in this case report were extensive and bilateral. This posed a considerable risk of mandibular fracture in the peri-operative and postoperative period had simple curettage of the cysts been attempted. Furthermore, the histologic diagnosis, at the time of radiography, was of a potential basal-cell carcinoma, and this is a tumor that requires en bloc resection, with surgical margins to prevent recurrence. 13 In light of this, bilateral rostral mandibulectomy was believed to be the only feasible treatment option; however, the anticipated postoperative appearance and degree of prehensile function of the jaw was not acceptable to the dog's owners.
The present case of severe bilateral cystic lesions of the mandible, in close association with the tooth roots, failed to conform to the conventional criteria of any of the previously described odontogenic cyst types in dogs. In conclusion, odontogenic cysts should be considered in the differential diagnosis of mandibular swellings in dogs, but difficulties remain in their classification.
Footnotes
Acknowledgements
We thank Tracey Dewey and John Conibear for their preparation of the figures printed in this article. We thank Irene McCandlish for her kind cooperation in discussing the initial biopsy findings.