
Abstract
The purpose of the study was to perform an immunohistochemical and histological evaluation of samples taken from different bone regeneration procedures in atrophic human mandible. 30 patients (15 men and 15 women, age range of 35–60 years), non-smokers, with good general and oral health were recruited in this study and divided into three groups. The first group included patients who were treated with blood Concentration Growth Factors (bCGF), the second group included patients who were treated with a mixture of bCGF and autologous bone, while the third group of patients was treated with bCGF and tricalcium phosphate/hydroxyapatite (TCP-HA). Six months after the regenerative procedures, all patients undergone implant surgery, and a bone biopsy was carried out in the site of implant insertion. Each sample was histologically and immunohistochemically examined. Histological evaluation showed a complete bone formation for group II, partial ossification for group I, and moderate ossification for group III. Immunohistochemical analysis demonstrated a statistically significant difference between the three groups, and the best clinical result was obtained with a mixture of bCGF and autologous bone.
Introduction
Bone regeneration in the oral cavity is the subject of many studies in the literature because it aims to obtain a new natural bone structure. 1 Implant-supported oral rehabilitations are a high-success-rate treatment with a positive impact on patients’ quality of life. Many studies were conducted in order to develop the most suitable and adaptable material for bone tissue regeneration. However, short- and long-term complications are possible. 2 Growth bone regeneration comprised a well-orchestrated series of biological events of induction and conduction, involving different cell types and intracellular and extracellular molecular-signaling pathways, with a definable temporal and spatial sequence, in an effort to optimize skeletal repair and restore skeletal function. At the time of this writing, an important competition in bone tissue engineering is ongoing. It also concerns large-scale production of biomaterials based on bone extracellular matrix components (collagen, glycosaminoglycans, and calcium phosphate) that use efficient approaches in terms of functionality and costs. Implant failures may be categorized into early failures, which are associated with the surgical stage, 3 and late failures which occur after the prosthetic phase. 4 Peri-implantitis5,6 is one of the most common cause of biological failures, while risk factors such as occlusal overload and the presence of cantilevers, as well as bruxism and clenching para-functional habits are related to mechanical failures. Implant placement requires a sufficient residual bone volume. In case of inadequate bone amount, it may be necessary to perform an augmentation procedure. Some of the biomaterials reported in the literature are the following: PRP (platelet-rich plasma), PRGF (platelet-rich growth factors), PRF (platelet-rich fibrin), and bCGF (blood Concentration Growth Factors), which have the effect to improve hard and soft tissue healing. 7 They are derivatives of a platelet concentrate containing a number of growth factors (GFs): platelet-derived growth factor (PDGF), transforming growth factor beta 1 and 2 (TGF-β1 and TGF-β2), and insulin-like growth factor 1 (IGF-1). These factors have numerous positive characteristics in terms of tissue healing including the effects of mitogenesis, angiogenesis, and local disturbance. All these factors are involved in bone regeneration. The mentioned factors obtained after centrifugation were experimented both “in vitro” and “in vivo” and used alone as well as in association with different mixtures of materials: autologous, allograft, heterologous, and alloplastic. In this research, we performed an immunohistochemical and histological examination of the specimens provided by different bone regeneration procedures in the human mandible.
Materials and methods
A prospective clinical study was conducted between 2014 and 2017 in three different centers: Sapienza University of Rome (Italy), Nicolae Testimiţanu University of Medicine and Pharmacy (Moldova) and Victor Babes University of Medicine and Pharmacy (Romania). The purpose of the study was to perform an immunohistochemical and histological evaluation of regenerated bone in atrophic mandible with three different biomaterials. Patients with inadequate bone volume for implant placement in the mandible and who need bone regeneration for an implant-supported fixed prosthesis were enrolled in the study. Local research ethics committee approved the study protocol, and informed consent was received from all subjects in accordance with the Helsinki World Medical Association Declaration.
30 patients (15 men and 15 women, age range of 35–60 years), non-smokers, with good general and oral health were recruited in this study and divided into three groups. The first group included patients who were treated with bCGF, the second group included patients who were treated with a mixture of bCGF and autologous bone, while the third group of patients was treated with bCGF and tricalcium phosphate/hydroxyapatite (TCP-HA; ossceram nano GmbH & Co.KG). Six months after the regenerative procedures all patients undergone implant surgery and a bone biopsy was carried out in the site of implant insertion.
Group I (bCGF only)
The surgery was followed by local anesthesia (alphacaine SP4% articaine 1:100,000, Dentsply) applied to 10 patients, of which five were men and five were women (age of 55 ± 7.7 years, P
Group II (bCGF + autogenous bone)
To each of the 10 patients (56.8 ± 8.4, P
Group III (with hydroxyapatite, beta tricalcium phosphate + bCGF)
This group included 10 patients (56.8 ± 8.4, P < 0.05), who had a weakly developed bone tissue with partial atrophy and needed a prosthetic implant rehabilitation. Each patient was administered local anesthesia and had a flap extraction, plus a block of bone was ejected using a milling cutter (trephine burr) for biopsy. In the area of biopsy, a mixture of H/A + beta tricalcium phosphate + bCGF was administered after which the flap was sutured with absorbable 3–0 Vicryl thread (Ethicon). After 6 months follow-up, the second biopsy was performed. At the same time, the patients of this group had a mandible implantation.
GFs (bCGF) are naturally occurring regulatory molecules which bind to receptors on the cell surface. They stimulate cell and tissue function through influencing cell differentiation by changing their biochemical activity and cellular growth, and regulating their rate of proliferation.
In our experiment, the biomaterial of bCGF was obtained after centrifugation of the patient’s blood. One tube was filled with 9 mL (in tubes was citrate phosphate dextrose adenine solution for anticoagulation). The spin was performed at 3600 r/min for 11 min dividing the blood into five basic components according to our method: Fr.I (Serum), Fr.II (White clot), Fr.III (GFs), Fr.IV (Red clot), and Fr.V (Red substance). For the regeneration, we cut only a fraction and we used GFs, Red clot, and Red substance. Were used four tubes (tubes had 9 mL) centrifuged for only these patients. These fractions contained a higher concentration of ions (calcium, magnesium phosphate, and sodium) and IgM, IgG which participate in the process of angiogenesis, mitogenesis, and ossification. Magnesium (Mg) wire has been shown to be biodegradable and have anti-inflammatory properties. It can induce Schwann cells to secrete nerve GF, and connective tissue GFs promote the regeneration of nerve axons after central nervous system injury and skeletal connective tissues together with calcium (Ca).
Fixation and embedding
All the biopsies were immediately placed in 10% formalin (formaldehyde) and subsequently immersed into 0.5M ethylenediaminetetraacetic acid (EDTA) tamponade for demineralization. They were dehydrated using 95% ethanol for 6 h after being rinsed with water. The biopsies were, therefore, cleared in xylene for 5 h, soaked with paraffin for 5 h, and finally, embedded in liquid paraffin. Every section was cut with microtome 4 μm thick.
Coloring (hematoxylin/eosin)
Each sample was colored with hematoxylin/eosin (H/E). The sections were examined with a microscope (Nikon Eclipse E600) and a dedicated software for microscopic imaging analysis (Lucia G).
Immunohistochemical examination
The following antibodies were used for immunohistochemical examination of the samples: Anti-RUNX 2, Anti-Alkaline Phosphatase Tissue-Specific, Anti-SPARC, and Ki67.
Histomorphometrics
To quantify histological structures (osteoblasts, osteocytes, and positive immune-staining intensity), Widmer’s hot spot method was used.
Statistical analysis
Descriptive statistic, chi-square, and Student’s t tests were performed, and a P < 0.05 was considered statistically significant. A specific statistical software (IBM SPSS v10 Statistics, IBM) was used to analyze the data.
Results
Six months after the regeneration procedures, all patients were subjected to a bone biopsy with a trephine burr during implant insertion.
Histomorphometric assessment
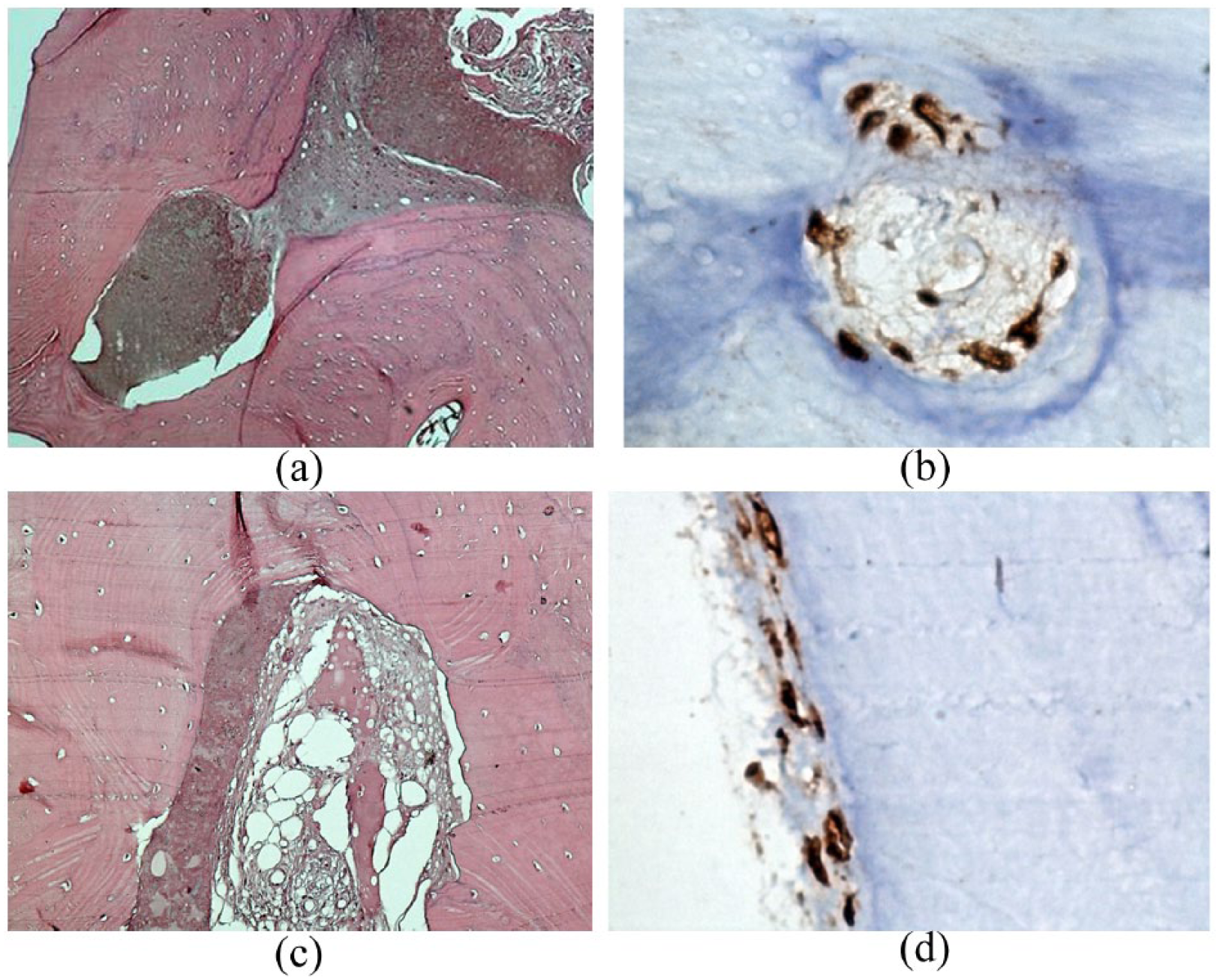
Each sample was colored with H/E for histo-morphological evaluation. In group I, some preparations contained approximately 70% of bone tissue and also immature tissue was observed. The cores of ossification incorporated incomplete cells that were different from the osteoblasts observed in the surrounding immature bone tissue, as well as membranous ossification cores. In other samples, connective tissue with cores of ossification and partially ossified matrix and disseminated osteoid were noticed. There were also many cores of ossification containing central conjunctive tissues surrounded by bone tissues with various degrees of maturation. Apposition of osteoid was ongoing as well. The presence of osteoclasts and a low number of cores found at the level of the osteoclasts suggested that the remodeling process was just starting (Figure 1).

Group I (blood Concentration Growth Factors)—histological and immunohistochemical stain. (a, b) A photomicrograph of group I showed area of spongy areolas connective tissues with extended zones of remodeling with the presence of infused material at the level of areolas and presence of bone tissue islands with vessel-rich areas. Many ossification cores including central conjunctive-like tissues are surrounded by bone lamellar (H/E-40). (c) Runx2: it is positive. There is a very high density of active osteoblasts on the bone surface (Runx-40 DAB). (d) Ki67: it is positive with active osteoblasts (Ki67-40 DAB). (f, g) SPARC and AAP: it is positive on the bone surface in the osteoid areas. High density of osteoblast and osteoclast level shows that remodeling process is just starting (anti-AAP-40 DAB and SPARC-40 DAB, respectively).
In the group II, 90% of bone tissue was observed. It was also noticed spongy bone tissue of the areolar type with numerous vascular-rich areas. On the bone surface there was a low density of active osteoblasts. The examined histological areas were predominated by osteocytes included in the slides of mature bone tissue (Figure 2).
Group II (blood Concentration Growth Factors and bone autogenous)—histological and immunohistochemical stain. (a, b) A photomicrograph of group II showed mature bone tissues, osteoid, connective tissues, and empty gaps without osteocytes (H/E-40). (c, d) A photomicrograph of group II showed expression of anti-SPARC-positive in cells of areolar connective tissues with nuclear expression. Osteoblast can be noticed at the level of the areolar connective tissue and not the bone surface (SPARC-40 DAB).
In group III, 60% of bone tissue was noticed, and conjunctive tissue in areola with areas of osteoid and mature bone tissue was observed. However, in other preparations, areas of connective unordered tissue and bone tissue with bone lamellas and without interconnections were detected (Figure 3).

Group III (blood Concentration Growth Factors hydroxyapatite and tricalcium phosphate)—histological and immunohistochemical stain. (a, b) A photomicrograph of group III showed areas of unordered conjunctive tissues and bone tissue with bone lamellar without interconnection without hematogenous marrow with acidophil material occupying bone areolas (H/E-40). (c) A photomicrograph of group III showed anti-Runx2-positive in the middle of the acidophil material occupying bone areolas attached to the disorganized bone lamellas (RUNX-40 DAB). (d) A photomicrograph of group III showed SPARC-positive in osteocytes and in osteoid (SPARC-40 DAB).
A statistically significant difference between group I, group II, and group III was obtained (P < 0.05).
Immunohistochemistry
Runx2 was expressed in osteoblasts and their precursors, while alkaline phosphatase was identified in osteocytes.8,9 Osteonectin (SPARC) was expressed by the whole line of osteocytes (osteoblasts’ precursors, osteoblasts, and osteocytes), while Ki67 was observed in the osteocyte cells involved in the mitotic cycle.
Group I
The specimens collected from patients of group I contained multiple Runx2-positive cells of a small size located near the surface of immature bone, disorganized bone lamellas, and areas of osteoid (Figure 1). In two cases, Runx2-positive blood vessels were also detected. Alkaline phosphatase was expressed in three samples (Figure 1(f)). In most of the cases, SPARK (Figure 1(g)) was strongly positive, both in cells located in bone lamellas and connective tissue adjacent to osteoid and bone lamellas. Ki67-positive cells were detected mainly in the connective tissue adjacent to the bone lamellas and osteoid areas (Figure 1(d)).
Group II
No Runx2-positive cells were detected in this group. Alkaline phosphatase was expressed by cells in six cases (Figure 2). SPARC was expressed in osteocytes and cells of the areolar connective tissue (Figure 2 (c)–(d)). During bone formation, an osteoblast is left behind and buried in the bone matrix as an “osteoid osteocyte,” which maintains contact with other osteoblasts through extended cellular processes. The processes of angiogenesis and osteocytogenesis are largely unknown, but the following molecules have been shown to play a crucial role in the production of healthy osteocytes. Osteoblasts were detected at the level of areolar connective tissue while nothing else was found on bone surface. Ki67-positive cells were rarely detected, being found in the connective tissue adjacent to the bone lamellas.
Group III
Few Runx2-positive (Figure 3(c)) cells were observed near disorganized bone lamellas. Alkaline phosphatase wasn’t noticed. The expression of SPARC-positive cells (Figure 3(d)) was confined to few cells attached to osteoid and non-mineralized matrix. Ki67-positive cells were rarely detected in the connective tissue surrounding non-mineralized matrix. The data of the immunohistochemical investigation are summarized in Table 1.
Immunoistochemical data.

bCGF: blood Concentration Growth Factors.
Discussion
GFs provide biochemical like mineral (calcium, magnesium phosphate, and sodium) and immunoglobulin cues for stem cell differentiation and are used to develop novel strategies to treat human diseases by investigating cellular processes controlling development, aging, and tissue regeneration. Modulation of GFs at the injury site is one of the strategies to stimulate tissue regeneration.
The research was designed to evaluate different methods for mandibular bone regeneration in three groups: group I (bCGF), group II (bCGF and autologous bone), and group III (bCGF and TCP-HA). Many studies produced good results using bCGF in association with different biomaterials, but the better outcome was obtained when centrifuged blood was mixed with autologous bone. 10 Even in our study, in terms of the new bone formation, better results were observed in the second group. We may explain this phenomenon by the osteoinductive potential of autologous bone which is recognized as an important starting factor for bone regeneration. GFs are naturally occurring regulatory molecules which bind to receptors on the cell surface. They stimulate cell and tissue function through influencing cell differentiation by changing their biochemical activity and cellular growth, and regulating their rate of proliferation, stimulate the adult mesenchymal stem cells which lead to bone formation. Thanks to autologous bone properties, patients of group II had already obtained mature bone after 6 months of healing. Tricalcium phosphate in combination with hydroxyapatite is deposited along the collagen fibrils, and in the proteoglycan ground substance, are widely used as bone scaffold material to increase the osteoconductive process. 11 In the group III of this research, a large amount of hydroxyapatite grains with big volume and very little osteoblast regenerated bone at histological level was found. However, a clinical examination showed adequate bone volume for implant placement. The immunohistochemical examination indicated that group I patients still have tendency to form bone tissue with persisting high concentration of osteoblasts, and few osteocytes after 6 months of healing, process of regeneration continued.
Many authors suggested that centrifuged blood can lead to bone formation both qualitatively and quantitatively. 12 We consider this opinion valid provided that centrifuged blood is administrated a second time after 3 months. Within the limitation of this study, the following conclusions were observed:
Histological evaluation showed a complete bone formation for group II, partial ossification for group I, and moderate ossification with persisting H/A residues of the patients for group III;
Immunohistochemical analysis demonstrated a statistically significant difference between group I, group II, and group III in terms of new bone formation;
The best clinical results were obtained with a mixture of bCGF and autologous bone (group II).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.