
Abstract
An aged mongrel dog was admitted for hemimandibulectomy as treatment for a mandibular mass that had been diagnosed as osteosarcoma. The fibro-osseous mass that surrounded the first molar tooth and replaced alveolar and cortical bone was reclassified as ossifying fibroma on the basis of anatomic location and histologic features. The tumor was composed of isomorphic fusiform cells with few mitotic figures. Tumoral stroma contained trabeculae of woven bone that were bordered by a single layer of osteoblasts. Excision was deemed complete with no evidence of extension or metastasis by computed tomography of the skull or thoracic and abdominal radiography. The dog was reportedly healthy 6 months after initial presentation. Though far less common than osteosarcoma as a primary canine bone tumor, ossifying fibroma should be included in the differential diagnosis for fibro-osseous proliferations, especially those of the jaw. Although benign, en bloc excision may be necessary for surgical cure.
A 15-year-old castrated male mongrel dog developed a mass in the left hemimandible around the first molar tooth. The owner reported that the dog pawed at its mouth, which suggested that the mass was painful. Two 1 cm × 2 cm incisional biopsy specimens from the buccal and lingual aspects of the mass were processed en toto for histologic examination by a reference laboratory; the diagnosis was osteosarcoma. One month later, the dog was admitted to the Purdue University Veterinary Teaching Hospital for total left hemimandibulectomy.
No abnormalities were detected in the available lateral radiographic view of the skull because of superimposition of the hemimandibles. However, in the computed tomographic (CT) scan (Fig. 1), an expansile and lytic lesion, about 1.8 cm in width and 2 cm from rostral to caudal borders, was evident in the dorsal aspect of the left hemimandible, surrounding the neck and roots of the first molar tooth. The mass destroyed alveolar and cortical bone, but had well-defined borders with a short transition zone. There was slight swelling, but no postcontrast enhancement of adjacent soft tissues. Thoracic and abdominal radiographs were within normal limits and free of evidence of metastatic neoplasia.
A left hemimandibular surgical specimen containing the entire mass had its margins painted prior to immersion in 10% neutral buffered formalin and submission to the Purdue University Animal Disease Diagnostic Laboratory (ADDL), where the specimen was transferred to a formic acid decalcifying solution. A firm to hard fibrous and bony mandibular mass surrounded the neck and roots of the first molar tooth and measured about 2.5 cm from rostral to caudal margins and 2 cm from medial to lateral aspects (Fig. 1, inset). Sections from the lingual and buccal aspects of the mass were prepared after 3 days of decalcification and processed routinely for histologic evaluation. Paraffin sections were stained with hematoxylin and eosin (HE) and Masson's trichrome.
The tumor consisted of a spindle-cell proliferation resembling periodontal stroma that appeared to be centered midway between the neck of the tooth and its apex. At its apparent site of origin, the tumor had provoked osteoclastic destruction of alveolar bone, adjacent cortical compacta, periodontal ligament, and bone of the alveolar crest. Symmetric growth of the mass expanded the lingual and buccal borders of the hemimandible, again by stimulating osteoclastic removal of the cortical compacta at a rate that allowed development of a thin, incomplete shell of periosteal new bone that partially contained the tumor. At the gingival sulcus (Fig. 2), the incomplete and partially resorbed periosteal shell of reactive bone nearly abutted the junctional gingival epithelium. Upward expansion of the tumor into gingival lamina propria led to ulceration and granulation tissue formation. On the buccal surface, the tumor was also partially bound by a thin periosteal shell of reactive bone that ended at the former level of the alveolar crest, which had been replaced by neoplastic tissue (Fig. 3). Here, the tumor extended above the level of the periosteal reaction into the gingiva. Neoplastic tissue (Fig. 4) was composed of fusiform cells in scanty fibrous stroma with light but diffuse infiltration by neutrophils. The fusiform cells had an elongated oval nucleus, small nucleolus, no mitotic figures in 15 high-power fields, and scanty pale eosinophilic cytoplasm with indistinct cell borders. The stroma was moderately vascular with numerous irregular trabeculae of osteoid and partially mineralized woven bone. Bony trabeculae were bordered by one layer of osteoblasts. A few osteoclasts were adjacent to bony spicules. There was little fibrous collagen in tumoral stroma; most of the Masson's trichrome–stained collagen was in the bony trabeculae.
A preliminary diagnosis of ossifying fibroma was reported with the final diagnosis to follow examination of remaining (central) tissue. The hemimandibular specimen was cross-sectioned through the first molar tooth after 4 days decalcification and returned to the formic acid decalcification solution. Macroscopically, the mass on cross-section consisted mostly of hard, white tissue that infiltrated alveolar and cortical bone and adjacent soft tissue (Fig. 1, inset). After another 5 days of decalcification, the hemimandible was transferred to hydrochloric acid/ethylenediamine tetraacetic acid decalcifying solution; mandibular cross-sections through and caudal to the mass were prepared for histologic processing. Sections of the fully decalcified central portion of the tumor were histologically similar to the initial peripheral sections, except that 1 to 3 mitotic figures were found per 10 high-power fields. Neoplastic tissue was not found in soft tissue ventral to the hemimandible or in mandibular or soft tissue caudal to the mass. Histologic impression was complete excision of an ossifying fibroma. The dog recovered well from hemimandibulectomy and was considered healthy with no clinical evidence of recurrence of the tumor 6 months after excision; radiography was not repeated.
In dogs, most primary bone tumors are sarcomas, especially osteosarcoma; benign tumors of bone are much less common. 5, 12, 14 Ossifying fibroma is a benign tumor of bone with predilection for the mandible. 14 In veterinary medicine, it has been reported most commonly in the rostral aspect of the mandible of young horses, where it is classified as juvenile mandibular ossifying fibroma. 8 In dogs, ossifying fibroma accounted for only 4 of 394 tumors or tumorlike lesions of bone in a retrospective study; 2 tumors were maxillary, and 2 were mandibular. 5 In the same study, there were 183 osteosarcomas, of which only 7.6% were in bones of the skull. 5 An ossifying fibroma was reported in the os penis of a dog with urethral obstruction. 7 Ossifying fibroma has also been reported in the cat, 16 greater kudu, 1 goat, 9 sheep, 11 llama, 6 and rabbit. 17
In human surgical pathology, ossifying fibroma is classified as a benign fibro-osseous lesion of the mandible or maxilla and considered by some to be a variant of fibrous dysplasia that is distinguished by the border of osteoblasts around its bony trabeculae and, because it tends to be circumscribed, is more amenable to surgical excision. 12 In a recent comparison of ossifying fibroma and fibrous dysplasia of the human jaw, the immunoreactivity of most osteogenic markers was similar; however, osteocalcin was strongly reactive in calcified regions of fibrous dysplasia but only weakly so in ossifying fibroma. 15 This finding suggests that the stromal cells of these 2 entities have different derivation. Radiographically, ossifying fibroma of the human jaw results in a well-defined osteolytic lesion with varying degrees of calcification and cortical thinning; the osteogenic cells presumably arise from stroma of the periodontal ligament. 2 The CT appearance of human juvenile ossifying fibroma has been described as expansile, with well-defined borders and a thin sclerotic shell; the tumor is locally aggressive with cortical disruption and involvement of adjacent tissues. 4
Benign fibro-osseous proliferations of bone in veterinary species include ossifying fibroma, osteoma, and fibrous dysplasia. 13, 14 Osteomas are typically solitary osteosclerotic lesions that arise from the surface of bones of the jaw or skull; trabeculae of woven bone constitute the bulk of the tumor, are rimmed by 1 layer of well-differentiated osteoblasts and, in many cases, are oriented perpendicular to the surface of the tumor. 14 Fibrous dysplasia 14 is a tumorlike lesion that can involve 1 or multiple bones, often in young animals. It arises within the bone, rather than from the periosteal surface, and its ample fibrous stroma contains only thin, curved trabeculae of woven bone. The bony trabeculae are generally not rimmed by osteoblasts, which distinguishes it from ossifying fibroma or osteoma, and are regularly spaced but without orientation relative to the periosteal surface.
Ossifying fibroma has histologic features that are intermediate between those of osteoma and fibrous dysplasia, although there can be overlap among the 3 entities. 13 Ossifying fibroma is an expansile, lytic, and invasive mass that develops within the bone, particularly the mandible. Its bony trabeculae are rimmed by osteoblasts as in osteoma but are arranged haphazardly and contribute relatively less to the fibro-osseous stroma.
Importantly, from a prognostic perspective, ossifying fibroma must be differentiated from malignant tumors, such as osteosarcoma. That distinction can be based on the lower cellularity, bland cytologic features, and low mitotic index of ossifying fibroma. Furthermore, bony trabeculae of ossifying fibroma tend to be better developed than in osteosarcoma and are bordered by a single layer of osteoblasts that are distinct from the tumor cells. However, histologic examination of excisional biopsy specimens and knowledge of the anatomic location of the tumor may be necessary for accurate diagnosis. To the authors' knowledge, the CT appearance of canine ossifying fibroma has not been reported previously. In an imaging study of oral masses in 19 dogs, 3 osteosarcoma was the most common malignant tumor and the most common lesion to involve bone. With CT, 6 osteosarcomas appeared as expansile maxillary or mandibular masses with bone destruction and poorly defined tumor margins. 3 In contrast, the mandibular ossifying fibroma in the dog of the current report was expansile with bone destruction but had well-defined margins. Ossifying fibroma does not metastasize and is not expected to recur after hemimandibulectomy, but recurrence has been reported in horses after incomplete excision. 10 Ossifying fibroma is readily distinguished from multilobular tumor of bone, a potentially malignant neoplasm that may arise in the jaw, by its predominant spindle cell component, lack of a lobular pattern, and lack of cartilage formation.
Too few cases have been reported to permit complete characterization of canine ossifying fibroma, yet the tumor is encountered by veterinary pathologists and may be confused with other benign or malignant bone tumors. A search of archived records of the Animal Disease Diagnostic Lab revealed no other cases of ossifying fibroma in dogs during the past 7 years, during which time 46 cases of canine osteosarcoma were diagnosed. Only 1 of 46 osteosarcomas was mandibular, and histologic features (nuclear atypia, higher cellularity, high mitotic index, direct production of osteoid by tumor cells, and production of cartilage) distinguished that tumor from ossifying fibroma. The present case demonstrates the importance of including ossifying fibroma in the differential diagnosis for an expansile, destructive and locally invasive, but histologically bland, fibro-osseous mass in the canine mandible.
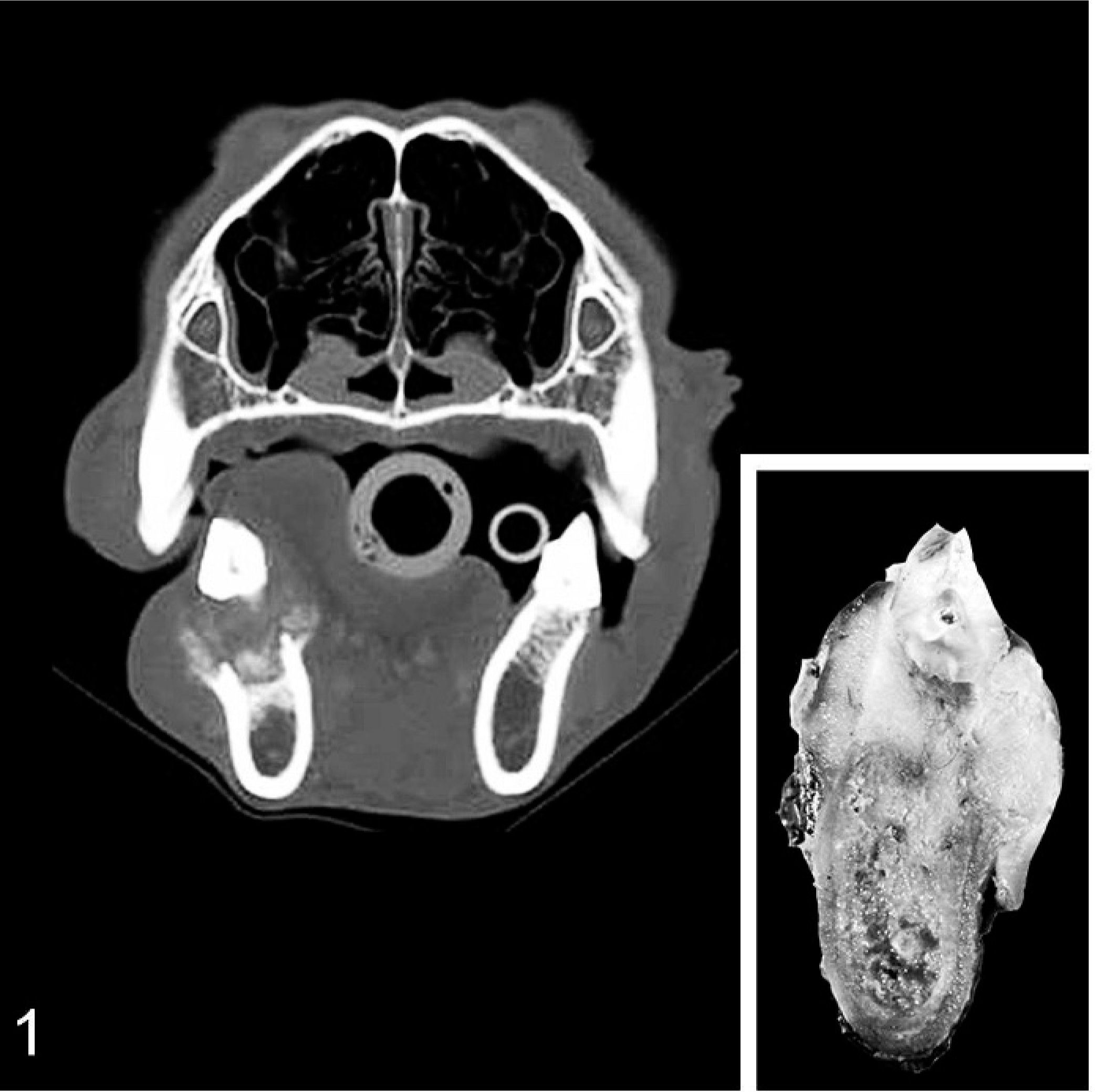
Computed tomographic scan; skull; dog. An expansile mass destroys alveolar and cortical bone in the dorsal aspect of the left hemimandible and extends into gingival tissue along the buccal and lingual aspects of the first molar tooth. Inset: Cross-section of the left hemimandibulectomy specimen through first molar tooth.
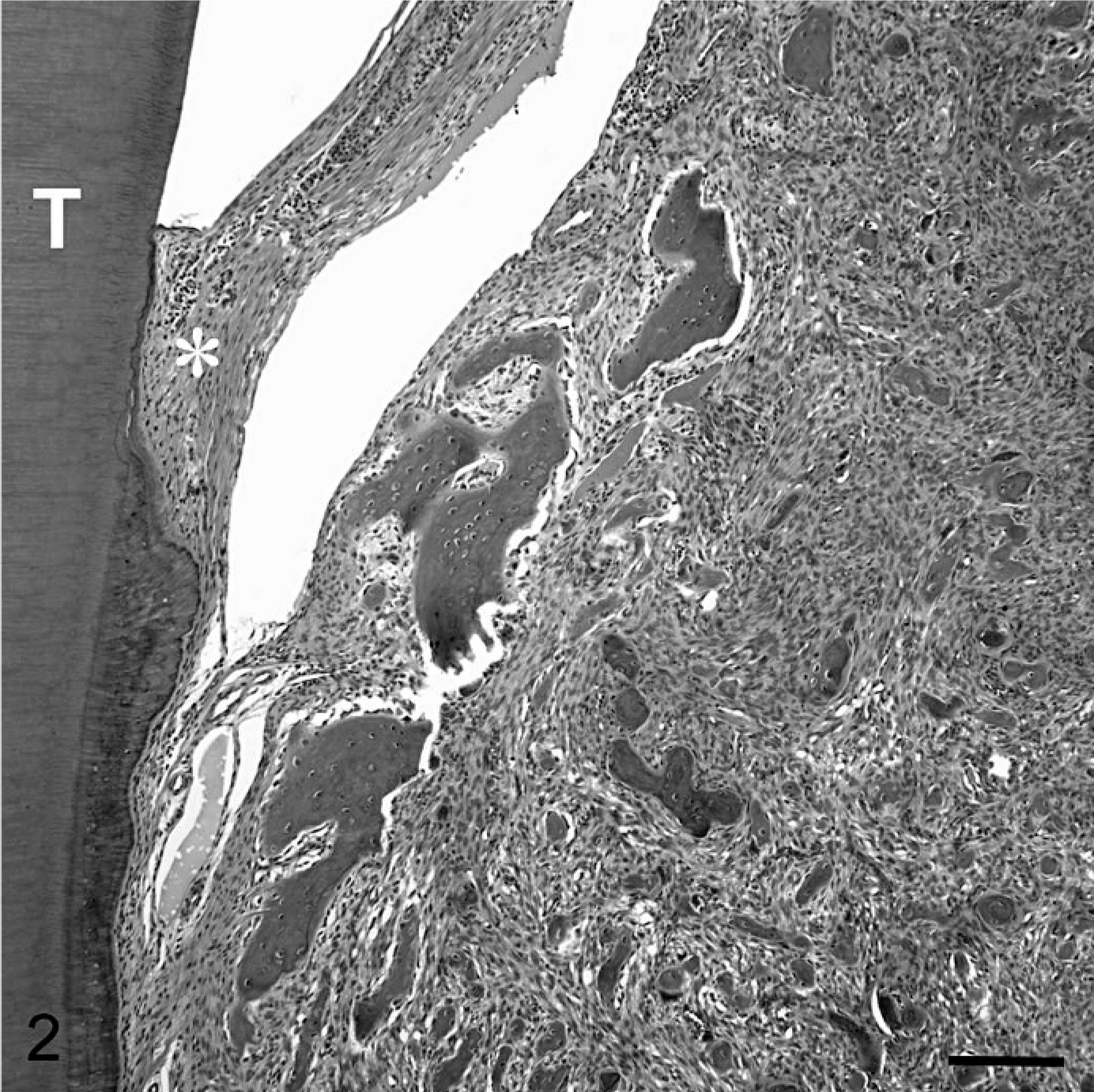
Ossifying fibroma; mandible; dog. The first molar tooth (T) has intact gingival attachment (∗), but cortical and alveolar bone and periodontal ligament are destroyed and replaced by a benign fibro-osseous proliferation with randomly distributed, irregular spicules of crude woven bone, leaving only an incomplete shell of reactive bone near the alveolar crest. HE. Bar = 150 μm.
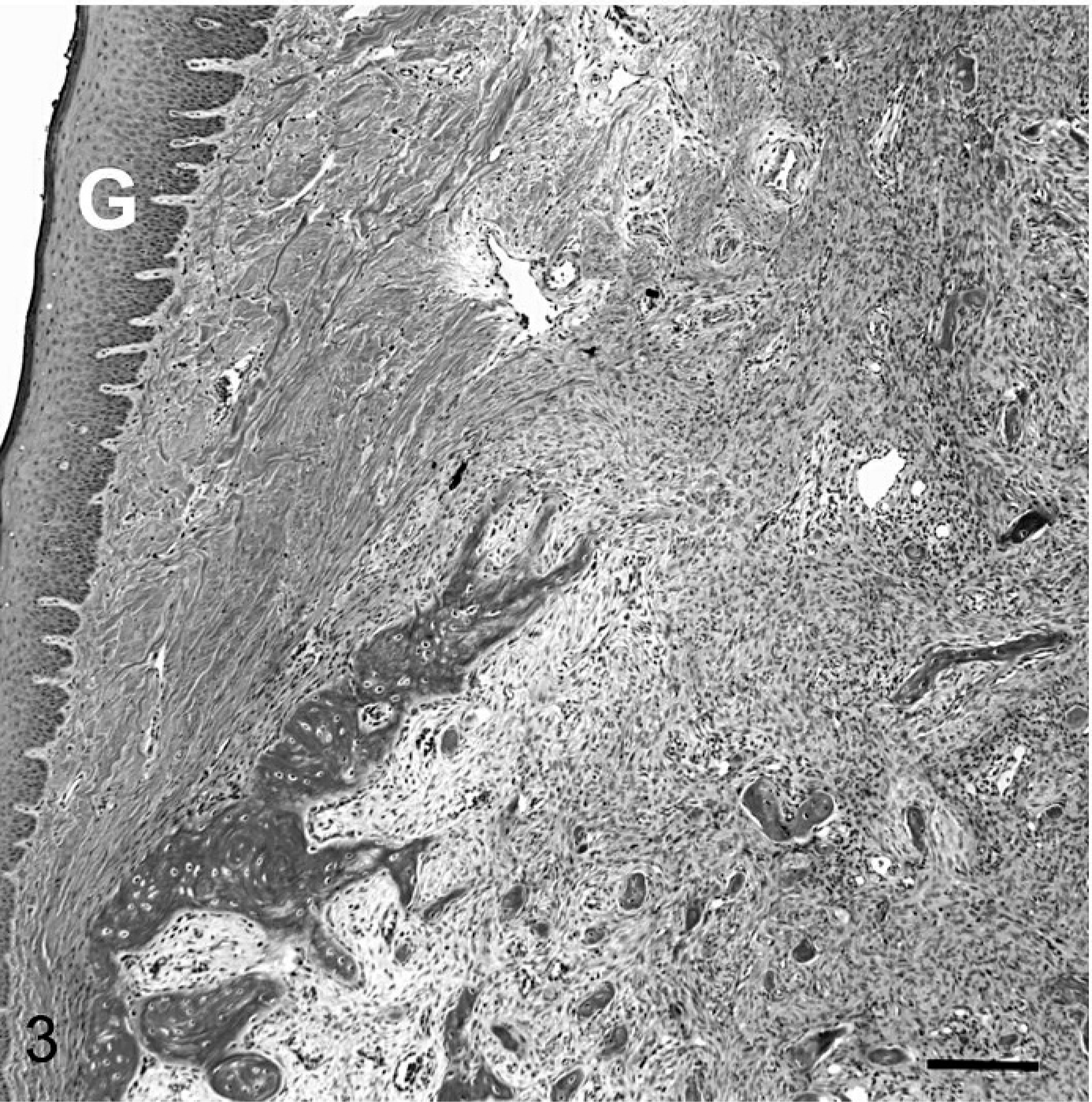
Ossifying fibroma; mandible; dog. Nonneoplastic fibrous connective tissue separates gingival epithelium (G) from the mandibular tumor, which is bound by a thin periosteal shell of reactive bone except at the level of the alveolar crest where neoplastic tissue erodes through the bone into overlying gingival soft tissue. Masson's trichrome stain. Bar = 150 μm.
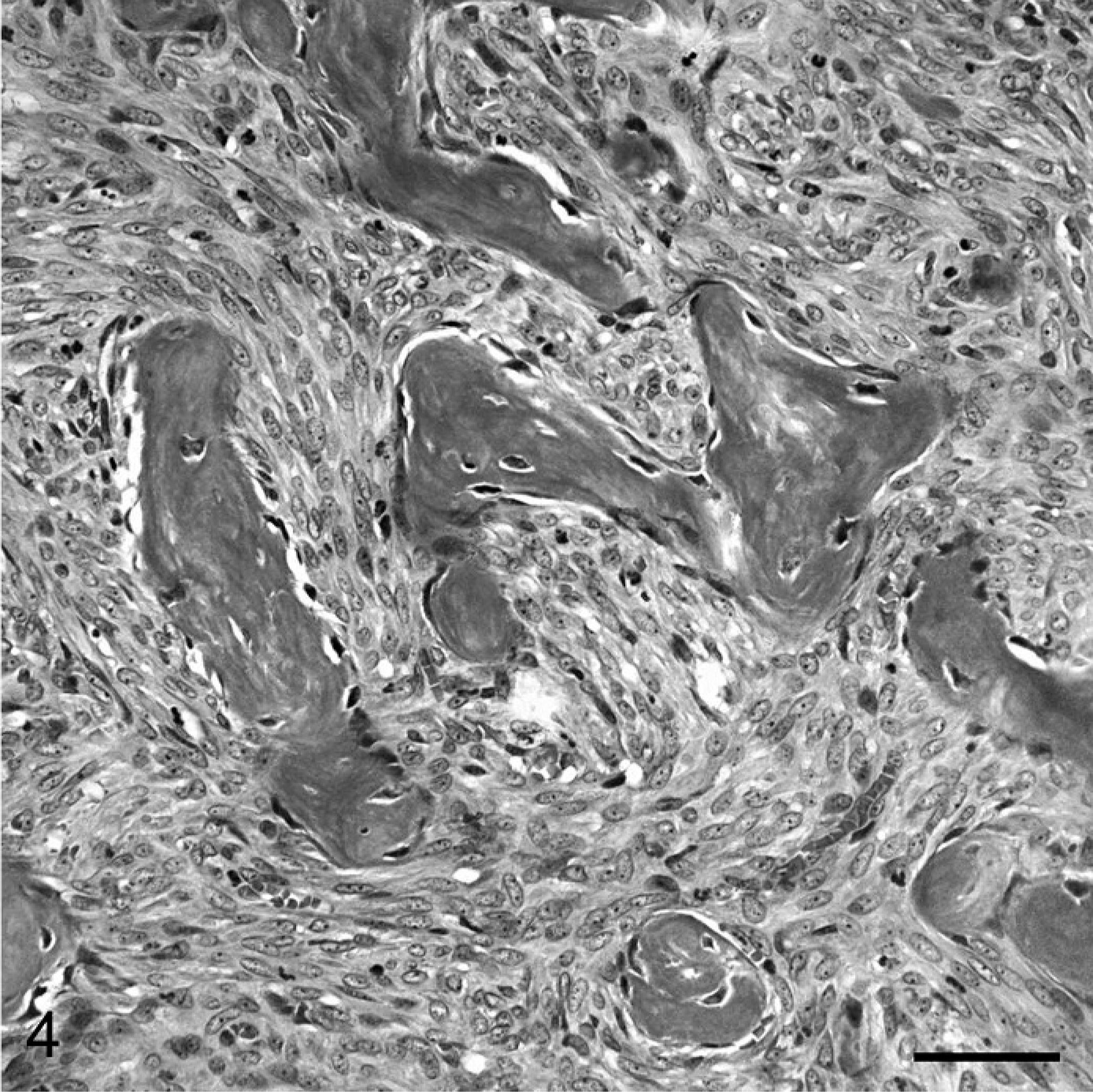
Ossifying fibroma; mandible; dog. Detail of the tumor with irregular trabeculae of woven bone in cellular fibrous stroma. Fusiform tumor cells have an oval hypochromic nucleus, small nucleolus, no mitotic figures, and scanty cytoplasm with indistinct cell borders. Bony trabeculae are rimmed by a row of osteoblasts. Masson's trichrome stain. Bar = 50 μm.
Footnotes
Acknowledgements
We thank Drs. Shirley Waibel and Lisa Banker, Blair Animal Clinic, West Lafayette, IN, for case referral and follow-up information.