
Abstract
An 8-year-old castrated male mixed-breed dog had an ill-defined hemorrhagic and painful lesion in the base of the claw of the second digit of the right forelimb. Radiographically, the expansile and lytic lesion affected the distal phalanx. The digit was amputated and submitted for histologic examination. Histologically, the distal phalanx was largely replaced by a mass composed of variably sized cavernous vascular spaces lined by a single layer of flattened endothelial cells. A similar mass was in the subcutis adjacent to the distal phalanx. The benign vascular proliferation involving the medulla of bone and a second tissue type in this dog is consistent with skeletal–extraskeletal angiomatosis as described in humans. To the authors' knowledge, this is the first report of skeletal–extraskeletal angiomatosis in the veterinary literature.
Angiomatosis is a condition with multiple tumorlike lesions caused by congenital or developmental malformations of blood vessels. In veterinary medicine, the term angiomatosis has been used to describe various conditions, including a benign dermal vasoproliferative lesion in young adult cattle (cutaneous bovine angiomatosis); 5 multifocal vascular proliferations in the abdominal and thoracic viscera (disseminated hemangioma) in a dog; 4 vascular malformations in the thoracic vertebrae (vertebral angiomatosis) in cats; 14 multifocal vascular proliferations in the dermis and subcutis (cutaneous angiomatosis) in dogs, 8,12 cats, 2,12 and horses; 13 multifocal nodules of numerous abnormal vascular channels in the intestines and/or ovary in horses; 9,13 and vascular malformations in the meninges (meningoangiomatosis) in dogs. 1 Here, we report skeletal–extraskeletal angiomatosis characterized by vascular proliferative lesions involving the distal phalanx and the adjacent subcutis of the second digit of the right forelimb in a dog.
Clinical History
An 8-year-old castrated male mixed-breed dog was presented to the University of Missouri Veterinary Medical Teaching Hospital for an ill-defined lesion of the claw base of the second digit of the right forelimb, with pain and profuse bleeding. Radiographically, an expansile and lytic lesion was observed in the distal phalanx of the affected digit (Fig. 1). Thoracic radiographs were unremarkable. There was a normocytic hypochromic anemia (hematocrit, 22% [reference interval, 37–57%]; mean corpuscular volume, 59 fl [reference interval, 59–76 fl]; mean corpuscular hemoglobin concentration, 28.1 g/dl [reference interval 32.0–36.4 g/dl]) with mild polychromasia and reticulocytosis (reticulocyte, 4% [no reference range]). Hematologic findings were consistent with the clinical history of profuse external hemorrhage. Based on the location of the lesion and the radiographic findings, subungual squamous cell carcinoma was suspected. The affected digit was amputated at the metacarpophalangeal joint and submitted for histopathology.

Dorsopalmar radiograph of the right front paw; dog. An expansile lytic lesion (arrow) is in the distal phalanx of the second digit.
Gross and Histologic Findings
The amputated digit was fixed in 10% formalin for approximately 24 hours before trimming. Upon dissection, a white to tan plaque-like nodule (approximately 8 × 6 × 1 mm) was revealed in the subcutis adjacent to the dorsal aspect of the middle to distal phalanges (Fig. 2). The skin and soft tissues were routinely processed for histologic examination. The phalanges were decalcified in Decalcifier II (Surgipath Medical Ind, Inc, Richmond, IL) for approximately 24 hours, bisected, and processed for histologic examination. Upon bisecting the phalanges, the medulla of the distal phalanx was brown to red; the grossly normal proximal and middle phalanges appeared pale gray to white (Fig. 3). In addition to hematoxylin and eosin (HE) stain, unstained 5-μm-thick paraffin-embedded tissue sections were prepared for immunohistochemistry, as performed with the MACH2 horseradish–peroxidase system and Romulin AEC chromogen kit (Biocare Medical, Concord, CA), according to the manufacturer’s instructions. Primary antibodies were CD31 (M0823, Dako, Carpinteria, CA) and smooth muscle actin (A0566, Dako).
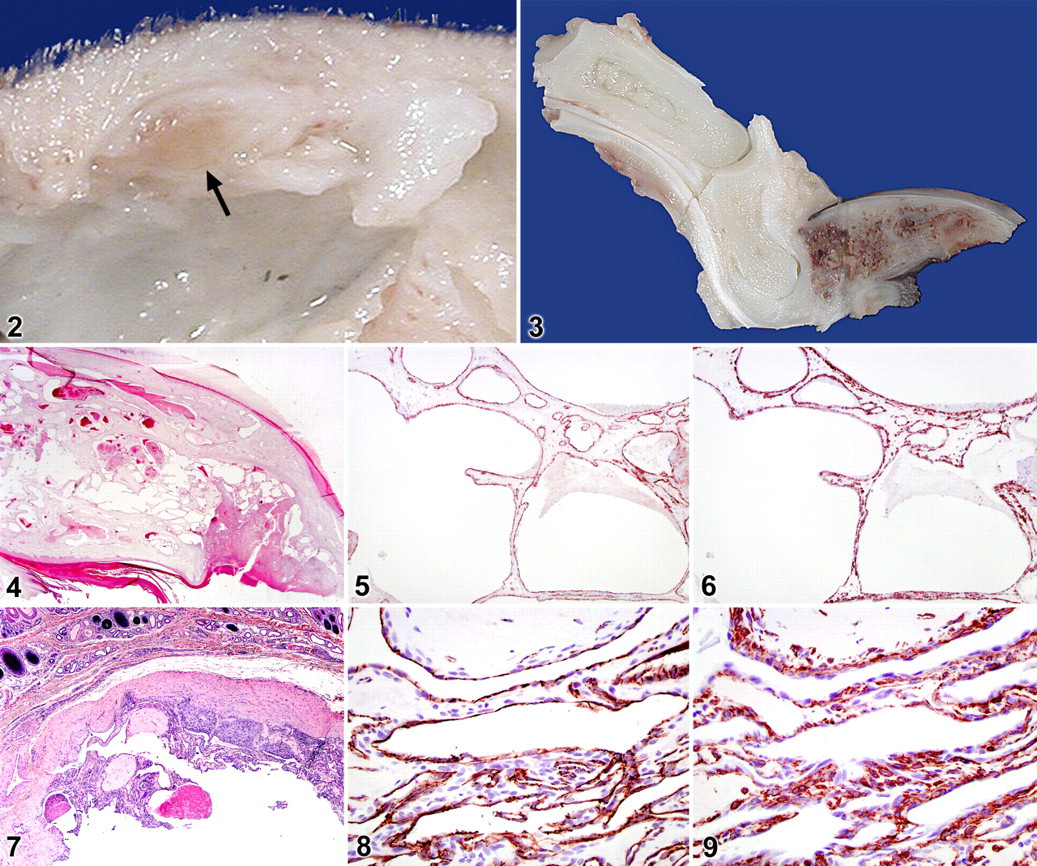
Histologically, the medulla and cortical bone of the distal phalanx were largely replaced by a nonencapsulated, relatively well-demarcated, moderately cellular mass composed of variably sized cavernous vascular spaces (Fig. 4). These spaces were lined by a single layer of flattened endothelial cells supported by 1 to 2 layers of smooth muscle cells, as demonstrated by immunohistochemistry for CD31 (Fig. 5) and smooth muscle actin (Fig. 6). There was little anisocytosis or anisokaryosis in the endothelial cells, and no mitotic figures were observed. Multifocally, the vascular spaces contained fibrin thrombi (Fig. 4). The distal palmar aspect of the claw bed epithelium was ulcerated and replaced by necrotic tissue coagulum with granulation tissue (Fig. 4). In the subcutis over the distal interphalangeal joint, a circumscribed but nonencapsulated moderately cellular mass was composed of variably sized and shaped vascular channels, proliferative capillary clusters, and blindly ending collagenous trabeculae lined by a single layer of flattened to plump cells (Fig. 7). As in the phalangeal mass, the vascular channels were lined by endothelial cells, as determined by CD31 immunohistochemistry (Fig. 8) and supported by 1 to 2 layers of smooth muscle cells (Fig. 9). Mild anisocytosis and anisokaryosis were noted in these endothelial cells, but no mitotic figures were observed. Focally, these vascular channels contained fibrin thrombi and organized thrombi (Fig. 7). The borders of both the masses in the distal phalanx and the subcutis were complete within the tissue sections examined. Both masses were considered benign vascular proliferative lesions based on the histologic findings, including little cellular atypia of endothelial cells and well-organized vascular structures lined by a single cell layer of endothelium and supported by 1 to 2 layers of smooth muscle cells. The diagnosis was angiomatosis of the distal phalanx and adjacent subcutis.
Discussion
Squamous cell carcinoma arising from the subungual epithelium is the most commonly detected digital tumor in dogs, constituting 51.6% of these tumors, 6 and is frequently associated with radiographic evidence of bone lysis. 11 Melanoma is the second-most-common digital tumor in dogs, constituting 15.6% of these tumors, 6 and is less commonly associated with radiographic evidence of bone lysis. 11 Given the lack of osseous response in this case, osteosarcoma—which accounts for 6.3% of canine digital tumors 6 —was considered less likely. Although digital metastasis from a primary bronchogenic carcinoma has been reported as one of the most frequently encountered digital tumors in cats, 16 a similar clinical syndrome has not been documented in dogs. Nevertheless, primary and secondary pulmonary neoplasia had been ruled out in this case on the basis of thoracic radiography before histologic examination. An infectious process could not be ruled out. Whether the lesion is neoplastic or an infectious process, amputation is a common treatment and diagnostic modality for canine digital conditions—especially, those in the nonweightbearing second or fifth digits. The treatment in this case consisted of amputation of the second digit at the metacarpophalangeal joint.
Carcinoma (primary or metastatic), melanoma, osteosarcoma, and inflammatory disease were eliminated from the differential diagnosis by histologic examination. When multiple vascular proliferative lesions involve a bone, as in this case, it can be difficult to ascertain if it is a primary medullary vascular neoplasm that has eroded into adjacent soft tissue, concurrent vascular neoplasms of bone and soft tissue, or angiomatosis. Although the distal phalangeal mass in this case was infiltrative and replaced bone structures and although a similar mass was in adjacent subcutis, malignancy was eliminated from the differential diagnosis for lack of the cellular pleomorphism and high mitotic index expected with hemangiosarcoma. Hemangioma is a well-circumscribed benign neoplasm of well-differentiated endothelial cells forming vascular channels, 5 whereas angiomatosis is a condition with multifocal tumorlike lesions composed of ill-defined vascular proliferations lined by a single layer of endothelial cells with minimal cellular atypia. 4 Although angiomatosis is considered a nonneoplastic condition, its term has been applied to multiple hemangiomas (disseminated hemangioma), 4 which reflects the difficulty in distinguishing nonneoplastic vascular proliferative growths from hemangiomas.
In human medicine, the term angiomatosis has been applied to an array of disparate lesions, ranging from large soft tissue lesions to multifocal skeletal lesions with various causes, including neoplasms, vascular malformations, and reactive changes. 3 The medical literature on angiomatosis of bone represents a plethora of conditions that include lesions restricted to the skeleton (cystic angiomatosis of bone), 10 focal or multifocal involvement of osseous structures by a benign vascular proliferation (primary hemangioma of bone), 7 lesions involving bone and extraosseous tissues (skeletal–extraskeletal angiomatosis), 3 and vanishing bone disease (Gorham disease). 15 Skeletal–extraskeletal angiomatosis is defined as a benign vascular proliferation involving the medullary cavity of bone and at least one other type of tissue, often adjacent soft tissue. 3 In this case, the histologic features of benign vascular proliferative lesions involving the medullary cavity of the distal phalanx and the adjacent subcutis are consistent with skeletal–extraskeletal angiomatosis as described in humans.
Clinically, expansile and lytic bone lesions with thinning of overlying cortical bone, as seen in this case, are the most frequent radiographic findings in human skeletal–extraskeletal angiomatosis. 3 Anemia secondary to chronic bleeding, as observed in this case, is also reported in human patients. 3 The dog of this report was 8 years old at diagnosis. Similarly, veterinary and human cases of angiomatosis are often diagnosed in middle-aged or older patients, 2 –4,9,12 suggesting that it is frequently an acquired condition or may remain latent for years.
The dog of this report had no evidence of residual lesions, regrowth, bleeding, dehiscence, or infection at the amputation site 12 months after surgery. Although digit amputation resulted in an excellent 1-year outcome in this case, the prognosis for skeletal–extraskeletal angiomatosis in veterinary patients should remain guarded on the basis of reported recurrence and fatalities in some human patients. 3 To the best of our knowledge, this is the first report of skeletal–extraskeletal angiomatosis in the veterinary medical literature. Thus, extraskeletal tissue—particularly, adjacent soft tissue—should be evaluated to rule in or rule out skeletal–extraskeletal angiomatosis when a benign vascular proliferation involves the medullary cavity of bone.
Footnotes
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.