
Abstract
Abdominal ultrasound examination in an 11-year-old, intact, female Labrador dog with hepatic disease revealed a nodular swelling of the left adrenal gland. Hyperadrenocorticism was suspected, but endocrine tests were negative. At the owner's request, an adrenalectomy was performed. Grossly, a nodular mass protruded from the external surface of the left adrenal gland and in cut section was hemorrhagic and effaced the cortical and medullary regions. Histologic examination revealed a cortical neoplasm with medullary involvement. The mass was composed of well-differentiated adipose cells, megakaryocytes, hematopoietic cells, and macrophages containing hemosiderin deposits. A diagnosis of cortical adrenal myelolipoma was made.
Keywords
Adrenal myelolipoma is a benign, endocrinologically inactive tumor, composed of well-differentiated adipose tissue and a variable amount of hematopoietic cells of both lymphoid and myeloid lineages. Admixed calcified or osseous foci can also be observed. 3 Despite being a relatively frequent neoplasm in humans, 18 myelolipoma is uncommon in veterinary species. In humans, adrenal myelolipomas were first described by Gierke 5 in 1905 and by Oberling 14 in 1929 and were later also observed in the lung, 19 presacral retroperitoneum, 22 and mediastinum. 4 There is also an association in humans between occurrence of adrenal myelolipoma and adrenogenital syndrome 11 in which there is a congenital adrenal hyperplasia because of 21-hydroxylase 2, 12, 15, 16, 24 or 17alpha-hydroxylase deficiency, 13 both of which are enzymes essential to the synthesis of adrenocortical hormones. Secondary to this reduced hormonal synthesis, there is an excessive stimulation of the adrenal cortex by adenocorticotropic hormone (ACTH), with subsequent cortical hyperplasia. The features observed in the adrenogenital syndrome associated with myelolipoma can include Cushing disease, 27 pseudo-hermaphroditism, 16 testicular tumors, 2, 17 Addison disease, and obesity of unknown cause. 26
The excessive ACTH secretion is considered to play a significant role in the pathogenesis of adrenal myelolipoma. 13, 21 Most of the adrenal myelolipomas in humans are small and asymptomatic and usually represent incidental findings at autopsy or during diagnostic imaging studies performed for other reasons. 1, 7
In the veterinary medical literature, myelolipomas have been described in the spleen of the dog, 23, 28 cat, 20 and ferret, 9 in the liver of a cat, 10 in the subcutaneous tissue and liver of exotic birds, 8 and in the adrenal gland of nonhuman primates. 6, 25
An 11-year-old, intact, female Labrador dog was presented for clinical evaluation of hepatic disease. Serum biochemistry analysis revealed elevated levels of alkaline phosphatase (540 IU/liter). Abdominal ultrasound examination was performed, and a mass on the left adrenal gland was observed. Endocrinologic tests for Cushing disease (basal serum cortisol and low-dose dexamethasone stimulation) were performed and were within normal limits; however, at the owner's request, an adrenalectomy was performed. No clinical or anatomical features consistent with adrenogenital syndrome were noted.
The left adrenal gland was markedly enlarged (25 × 15 × 15 mm) with a focal 10-mm-diameter nodule protruding from the external cortical surface. On transverse cut section, normal adrenal gland architecture was effaced by a moderately well-demarcated, firm, white-tan nodule with admixed and surrounding areas of hemorrhage (Fig. 1).
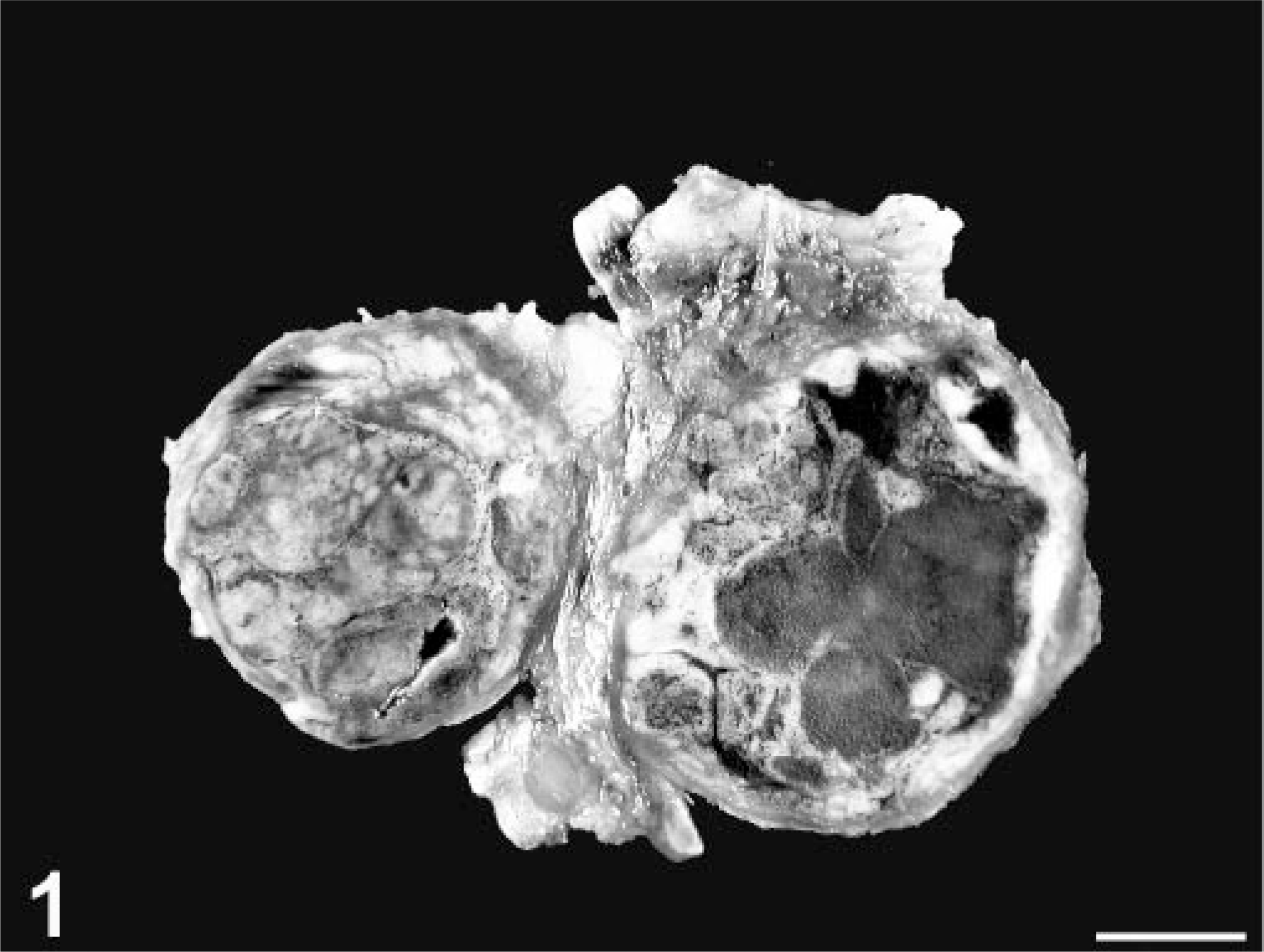
Adrenal gland; dog. Cross section with nodular cortical lesion (left) and hemorrhage (right). Bar = 45 mm.
Formalin-fixed samples of the adrenal gland were embedded in paraffin and sections stained with hematoxylin and eosin.
Histologic examination revealed a tumor that originated in the adrenal cortex and extended into the medulla. The neoplasm was composed of an accumulation of well-differentiated adipose cells that extended, in particular, to the level of the zona fasciculata of the adrenal cortex (Fig. 2) and was surrounded by a variable amount of hematopoietic elements that included megakaryocytes along with erythroid and myeloid precursors in progressive phases of maturation (Figs. 3, 4).
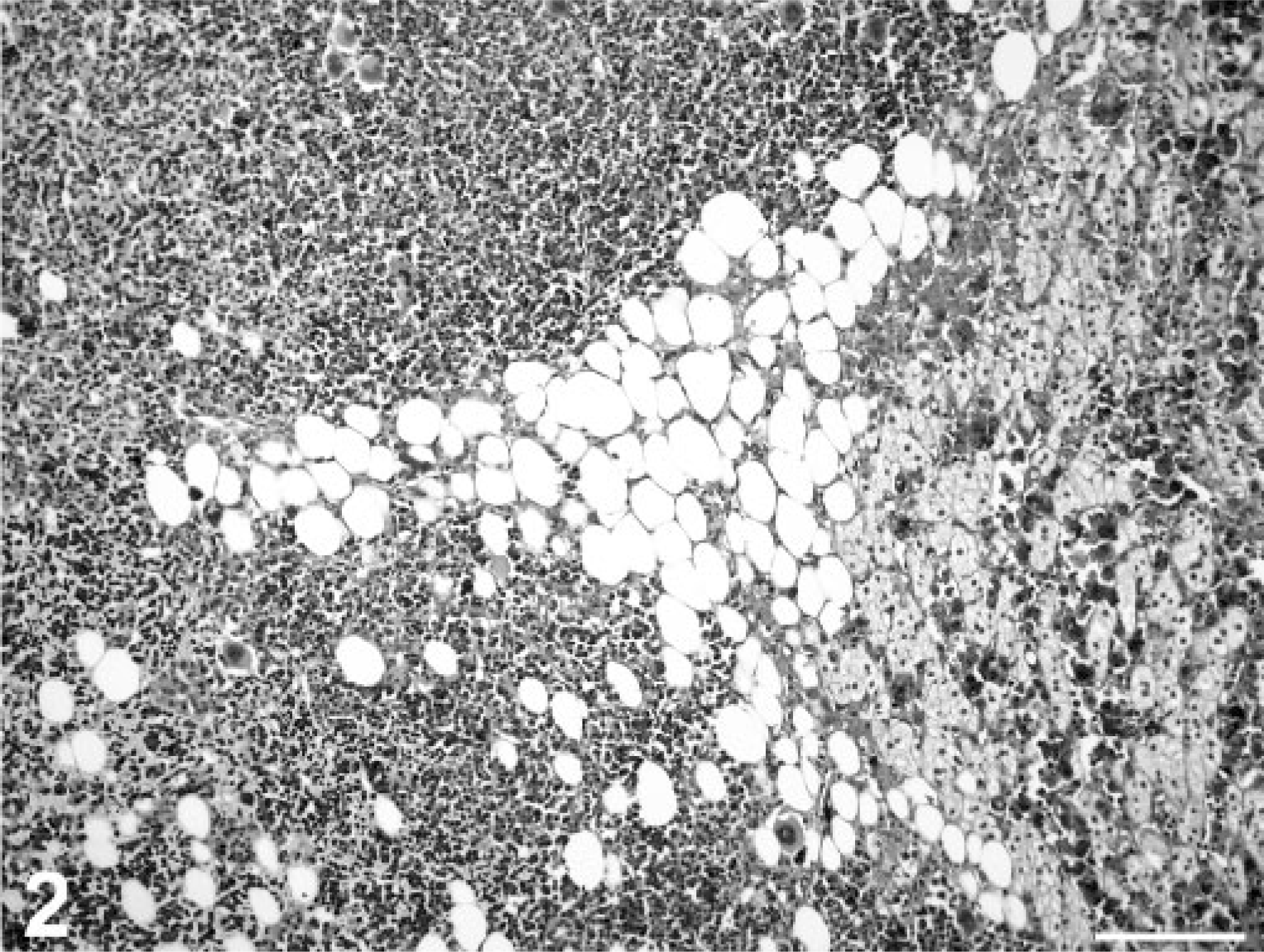
Adrenal myelolipoma; dog. Accumulation of well-differentiated adipose tissue and hematopoietic cells (left) close to adrenal cortex (right). Macrophages containing hemosiderin deposits are also visible in the zona fasciculata. HE. Bar = 120 μm.
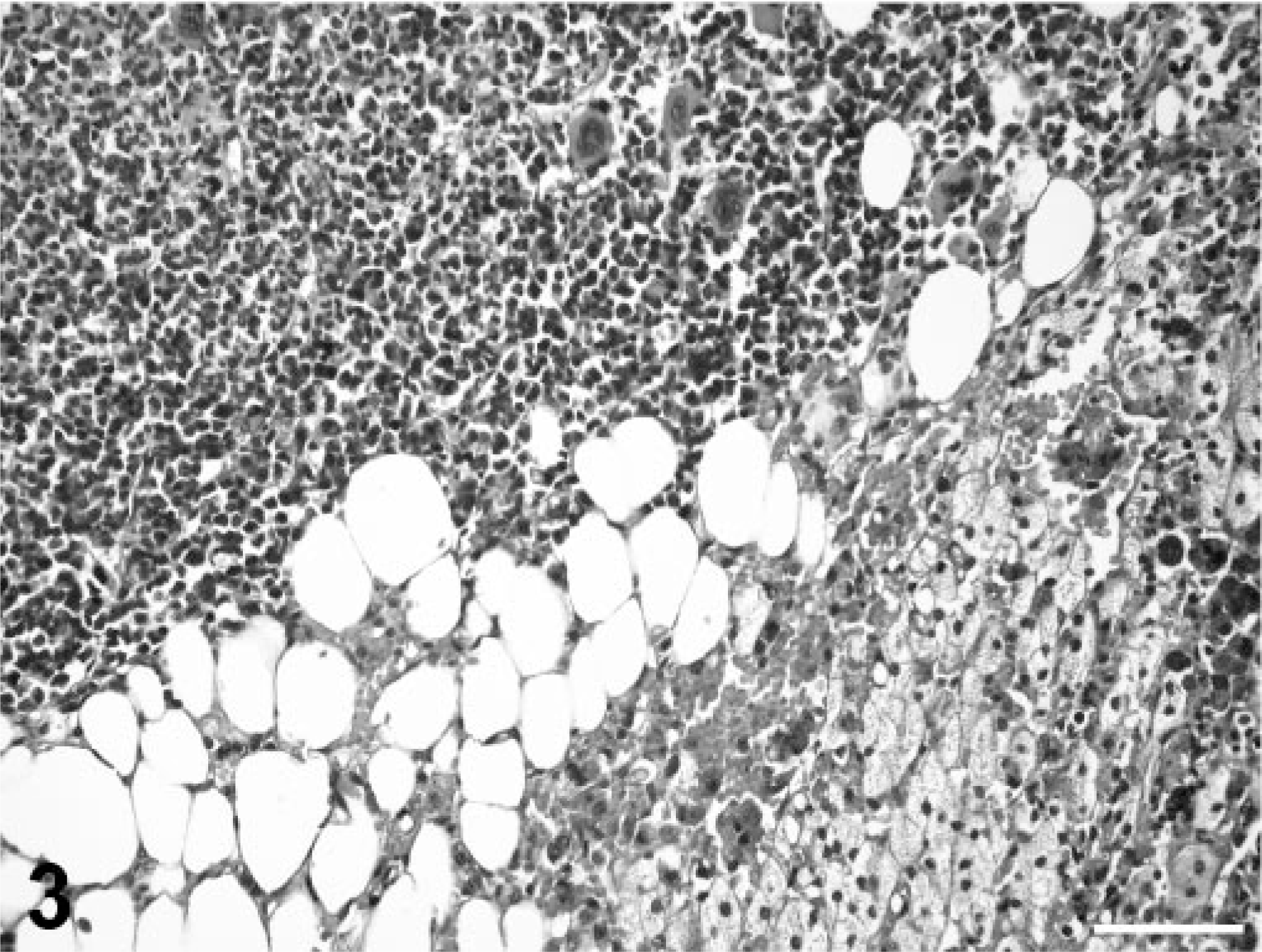
Adrenal myelolipoma; dog. Well-differentiated adipose cells admixed with megakaryocytes, erythrocytes, and hematopoietic cells. HE. Bar = 60 μm.
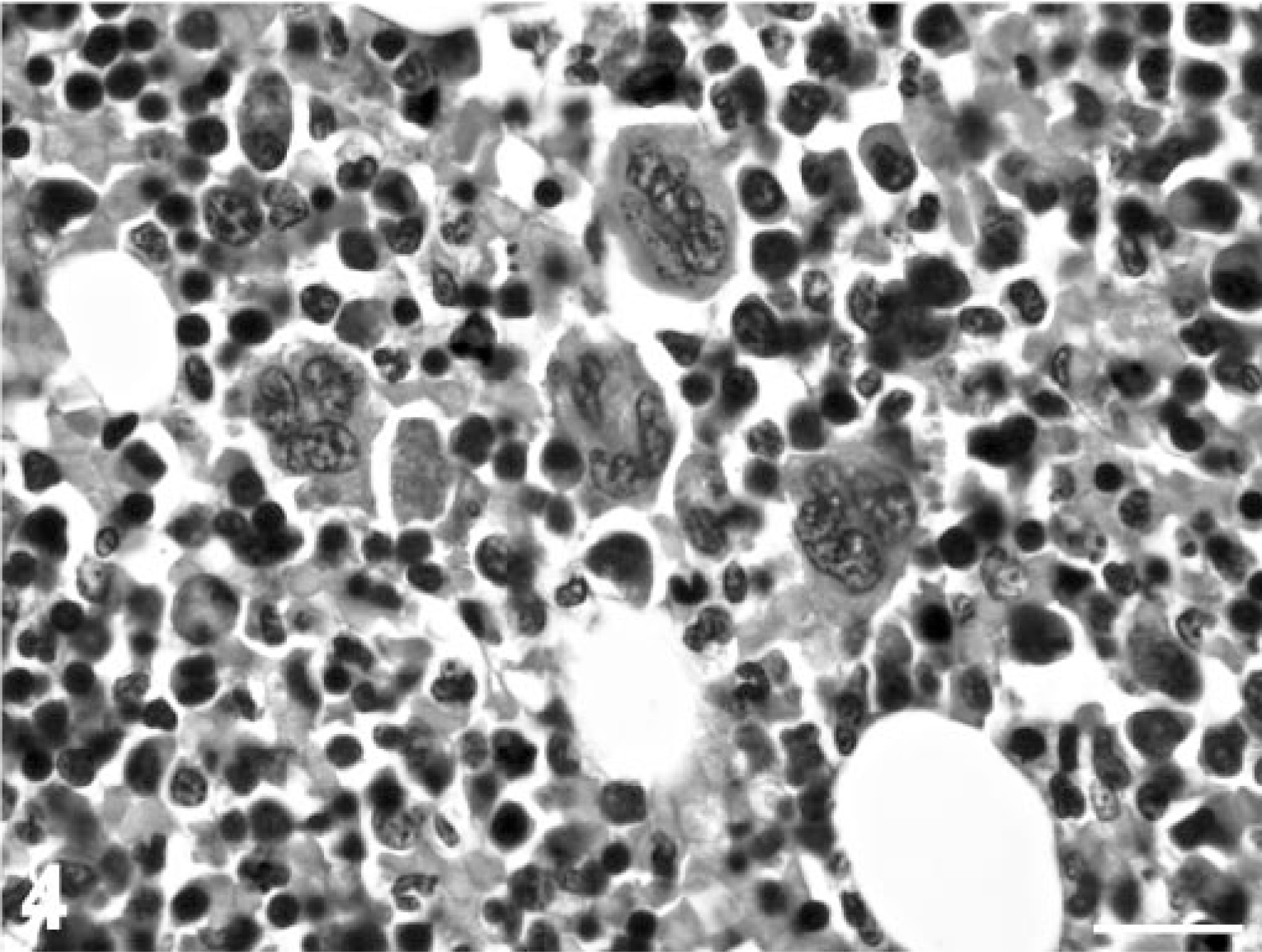
Adrenal myelolipoma; dog. Mature adipose cells and megakaryocytes with admixed myeloid and erythroid cells. HE. Bar = 20 μm.
Occasional megakaryocytes, lymphocytes, plasma cells, hemosiderinladen macrophages, and foci of moderate hemorrhage were also present in the adjacent regions of unaffected adrenal cortex.
Regarding adrenocortical masses, differential diagnoses to consider should include additional primary tumors of the adrenal cortex, such as adrenal adenoma and carcinoma. 3 In general, adrenocortical adenomas tend to be yellow-brown, firm, and very well demarcated on gross examination. However, adrenocortical carcinomas are often more friable and variably yellow-brown to reddened and less well demarcated. In the dog described in this report, the adrenocortical tumor was whitetan, firm, and moderately well demarcated. Although the gross features of such tumors may be helpful in considering certain differential diagnoses, it is important to remember that histopathologic examination is essential to make a definitive diagnosis. Microscopically, the presence of adipose cells with megakaryocytes and other hematopoietic elements is consistent with a diagnosis of myelolipoma.