
Abstract
Cytologic criteria were evaluated for their diagnostic value in liver disease in dogs. Therefore, histopathologic and cytologic examination was performed on liver biopsy samples of 73 dogs with liver diseases and 28 healthy dogs. Logistic regression analysis was used to select the measured parameters to be included in a multistep approach. With the logistic regression method, different characteristic cytologic parameters could be defined for each histopathologic diagnosis. In malignant lymphoma of the liver, the presence of large numbers of lymphoblasts with a minimum of 5% of all cells was found. Clusters of epithelial cells with several cytologic characteristics of malignancy intermixed with normal hepatocytes were indicative of metastatic carcinoma or cholangiocellular carcinoma. Liver cells in hepatocellular carcinoma were characterized by a high nucleus/cytoplasm ratio, large cell diameters, increased numbers of nucleoli per nuclei, small numbers of cytoplasmic vacuoles, and frequently, small numbers of lymphocytes. Extrahepatic cholestasis was characterized by excessive extracellular bile pigment in the form of biliary casts, an increased number of nucleoli within hepatocytes, decreased hepatic cell size, and low numbers of lymphocytes. In destructive cholangiolitis, increased numbers of neutrophils and a small mean nuclear size within hepatocytes were seen. Acute and nonspecific reactive hepatitis are diagnosed based on the presence of moderate reactive nuclear patterns, including more pronounced chromatin, prominent nucleoli, increased numbers of inflammatory cells, excluding lymphocytes, and the absence of increased numbers of bile duct cell clusters. Increased number of mast cells also was indicative of nonspecific reactive hepatitis. Important cytologic criteria for the diagnosis of liver cirrhosis, in addition to chronic hepatitis, are intracellular bile accumulation and increased numbers of bile duct cell clusters. In summary, the stepwise approach based on logistic regression presented in this study might be helpful in the objective cytologic diagnosis of hepatic diseases.
Cytologic examination of hepatic tissue obtained by fine-needle aspiration biopsy (FNAB) of the liver is being used with increasing frequency in companion animal medicine. 4,5,14,19,22,24,26,27,29 However, the gold standard for the diagnosis of most liver diseases is histologic evaluation of a number of wide-bore needle or wedge biopsy samples. Histologic examination is then based on the assessment of a number of liver acini. In contrast to histologic biopsies, the procedure to obtain fine-needle aspirates is minimally invasive and easy to perform without anesthesia or sedation, and smears can be examined immediately. Furthermore, fragments of histologic biopsy samples can be examined cytologically with impression smears.
Cytologic criteria for various liver diseases in the dog have not yet been well defined and often are only extrapolated from human literature. In addition, key criteria rarely are separated from secondary criteria. Not only is sound scientific knowledge lacking in the cytologic diagnosis of liver diseases but also is variation present within cytologic specimens from normal liver aspirates. In healthy humans 10,18 and dogs, 25 mild cellular variation and a few inflammatory cells are considered part of this normal variation. Furthermore, in healthy dogs there is evidence of age-dependent variation of cellular criteria. 25 Objective cytologic criteria in dogs with liver diseases have not been evaluated, making an objective and standardized cytologic examination of FNAB difficult.
This study analyzes hepatocellular cytologic criteria in dogs with different hepatobiliary diseases and helps develop a stepwise approach for the cytologic diagnosis of liver diseases in the dog.
Materials and Methods
Animals
Seventy-three dogs were referred to the Utrecht University Clinic of Companion Animals (UUCCA) with suspected liver disease during the years 1993–1996. Liver disease was suspected in these dogs by either abnormal liver parameters of clinical chemistry results or abnormal appearance of the liver during abdominal ultrasonography. In addition, 28 healthy blood donor dogs owned by the UUCCA also were included.
In all dogs, hematology, clinical chemistries, coagulation screening tests (prothrombin time, activated partial thromboplastin time, and fibrinogen concentration), and liver evaluation using abdominal ultrasound were performed. Diagnosis of liver disease was made by histopathologic examination of at least three 18-gauge-needle liver biopsy samples. Liver diseases identified included malignant lymphoma (n = 8), hepatocellular carcinoma (n = 12), metastatic carcinoma (n = 6), steroid-induced hepatopathy (n = 6), lipidosis (n = 1), extrahepatic cholestasis (n = 6), nonspecific reactive hepatitis (n = 10), acute hepatitis (n = 6), chronic hepatitis (CH) (n = 7), cirrhosis (n = 8), and destructive cholangiolitis (n = 3). All 28 healthy control dogs had normal liver histology.
Liver biopsy samples
In dogs with suspected focal liver disease on abdominal ultrasonography, biopsy samples were obtained under ultrasound guidance using an 18-gauge Trucut needle (William Cook Co.). Dogs were clipped, disinfected with alcohol (70%), and placed in right lateral recumbency, and the abdominal wall and the skin were locally anesthetized with 3% lidocaine. Under ultrasound guidance, a Trucut biopsy needle was placed through a small stab incision in the abdominal wall made with a surgical blade and advanced to the abnormal area for biopsy. Blind percutaneous liver biopsies were performed in right lateral recumbency in dogs with suspected diffuse hepatic disease, identified by ultrasonography, using a technique as first described by Lettow (1963). 15 Preparations and local anesthesia were similar to those used for Trucut biopsies. A small incision was made through the abdominal wall 1–2 cm caudal to the xyphoid, and an 18-gauge Menghini needle (William Cook Co.) attached to a 5-ml 0.9% saline-filled plastic syringe was inserted into the abdomen until it reached the left lateral lobe. Liver tissue was then aspirated with slight vacuum. From every dog, three biopsy samples, each 2–3 cm in length, were obtained.
One portion of each piece of hepatic tissue was used for cytologic impression smears, which were air-dried and stained with May-Grünwald-Giemsa. The other portion was fixed in 10% neutral buffered formalin. The fixed tissue was routinely embedded in paraffin, and 4-µm-thick sections were stained according to standard techniques with hematoxylin and eosin, Van Gieson stain, and Gordon and Sweet reticulin stain. Liver histology was evaluated by one experienced liver histopathologist (T. van den Ingh), and cytology was performed by one examiner (C. Stockhaus).
Cytologic examination
Cytologic smears were coded to prevent the observer from knowing the diagnosis. On initial evaluation of the smear, several representative parts of the slides were selected for further evaluation. As already described by Stockhaus et al., 25 slides were analyzed for general cell criteria, nuclear criteria, cytoplasmic criteria of hepatocytes, and the frequency of cell populations other than hepatocytes (Table 1). The number of intracellular vacuoles and bile pigment content were evaluated and scored 0–3 (0 = no vacuoles; 1 = small amounts of vacuoles in a minority of cells; 2 = variable amounts of vacuoles in a majority of cells; 3 = large amounts of vacuoles in almost every hepatocyte). For calculating incidence rates, the number of different cell types per 250 hepatocytes was used. Cell and nucleus sizes were measured with an ocular micrometer.
Description of cytologic criteria for evaluating liver impression smears in dogs.
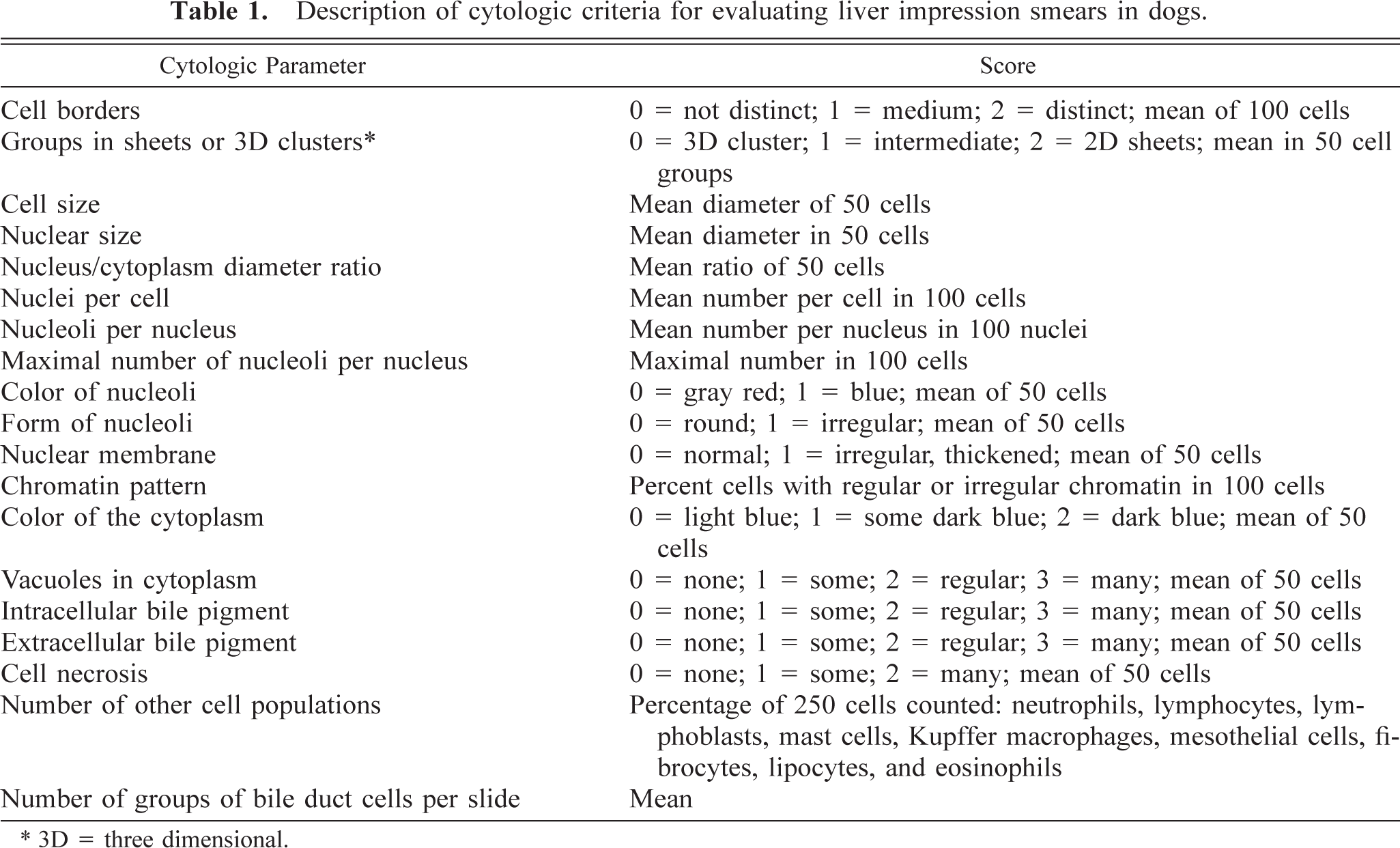
3D = three dimensional.
In a previous study, 25 significant age influences were observed for the parameters cell size, number of nuclei per cell, and nucleus/cytoplasm ratio. Therefore, these parameters were corrected for age influence by taking the individual difference of this parameter with the mean value of a comparable age group in healthy dogs. 25
Statistical analysis
Statistical analysis was performed by SPSS Windows 9.05 statistical packages. 20 Differences between groups were analyzed with the one-way analysis of variance for interval data, the Kruskal-Wallis test for ordinal data, and the chi-square test for bivariate data. Stepwise logistic regression analysis was performed to identify the significant variables important to diagnose the different liver diseases. For each step, variables with a P-value less than 0.20 on univariate regression score were included in the multiple regression model with forward-step analysis. In such a logistic regression model, Y = ln(P/(1 − P)) = β0 + (β1X1) + (β2X2) (βnXn), independent variables (X1, X2, …, Xn) are combined in a linear equation that is used to estimate the logarithm (Y) of the probability for the occurrence of an event (P) divided by the probability that it does not occur (1 − P). 2 Negative parameters in the equation have an opposite effect on the probability of the event as to positive parameters. Based on the values of the independent variables, the estimated logarithm given by a logistic regression equation can be used to calculate a conditional probability (P) of belonging to the group with the event using the formula P = (1 + exp(−Y))−1, where exp(−Y) is the exponential value of −Y. 12 For all significance testing, P-values less than 0.05 were considered to be significant.
Results
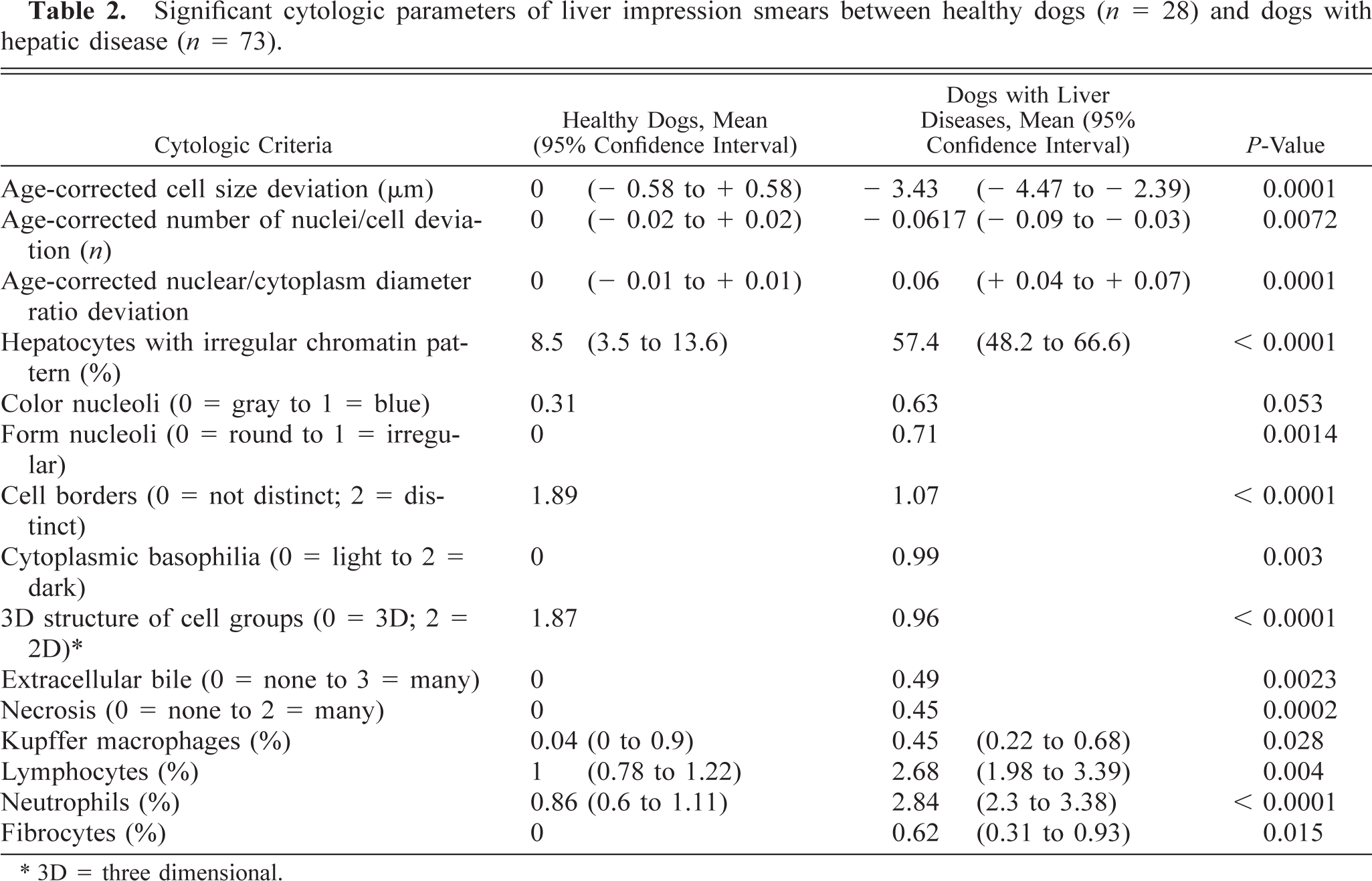
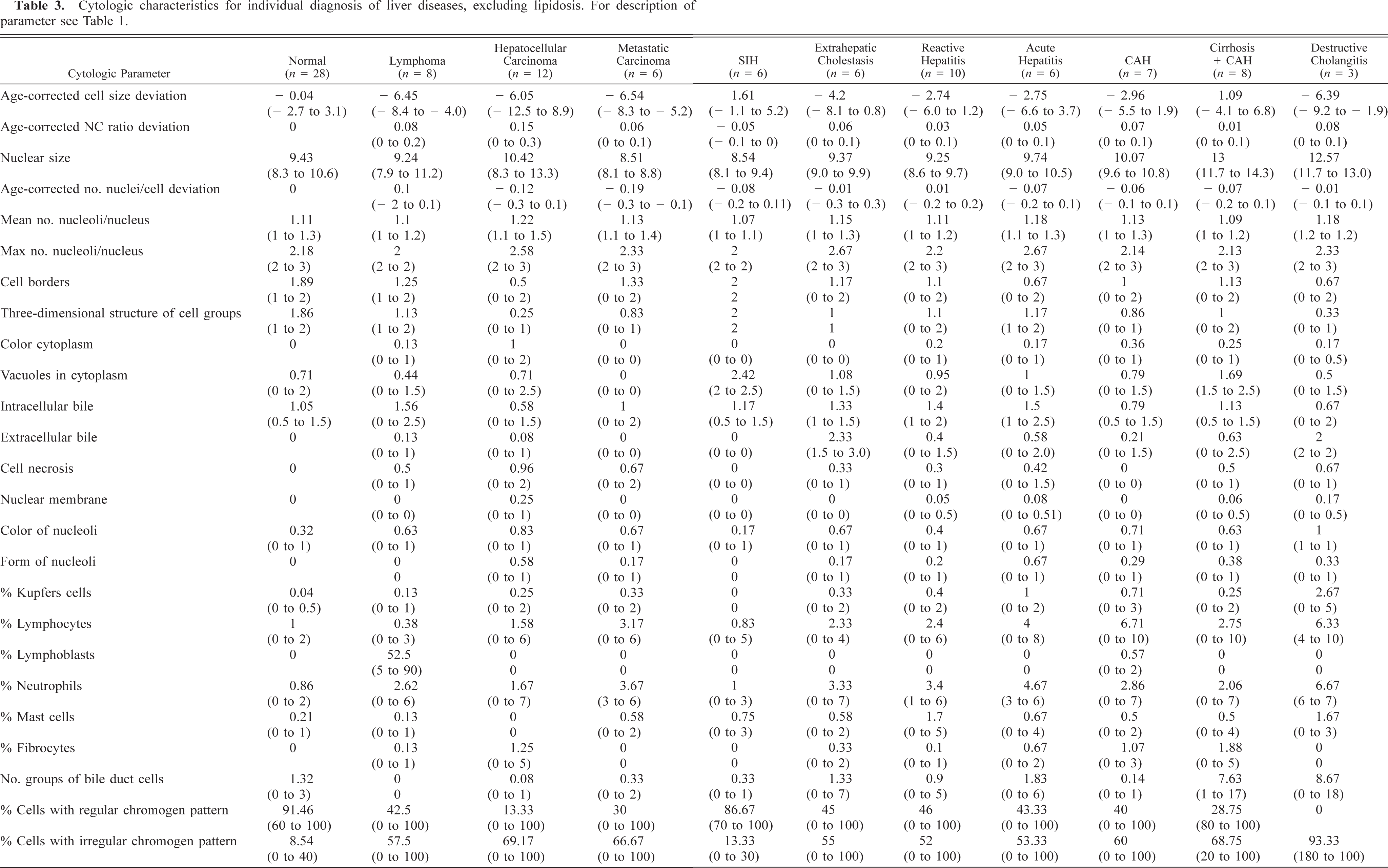
Individual cytologic criteria in the different liver diseases and healthy dogs are given in Table 1. Differences in cytologic parameters between the 28 healthy dogs and the 73 dogs with hepatic diseases are listed in Table 2.
Significant cytologic parameters of liver impression smears between healthy dogs (n = 28) and dogs with hepatic disease (n = 73).
3D = three dimensional.
Cytologic characteristics for individual diagnosis of liver diseases, excluding lipidosis. For description of parameter see Table 1.
Steroid-induced hepatopathy, lipidosis, and extra-medullary hematopoiesis were not included in the stepwise logistic regression method because they were considered to be secondary diagnoses (n = 7). The remaining 94 hepatic biopsy samples were included in the stepwise approach of cytologic evaluation of these smears.
In step 1, malignant lymphoma was diagnosed by the presence of large numbers of lymphoblasts (≥ 5% of total nucleated cells present in the biopsy sample) among the hepatocytes. During this step, mast cell metastasis to the liver also could be diagnosed. High numbers of mast cells or mast cells in sheets as well as mast cells with variable degrees of granulation are present in mast cell neoplasia. 16,19 During step 1, only eight dogs with malignant lymphoma were diagnosed. The remaining biopsy samples were used for step 2.
In step 2, clusters of epithelial cells with cytologic characteristics of carcinoma cells, such as anisocytosis, anisokaryosis, multiple or abnormal nucleoli, variable nucleus/cytoplasm ratio, and abnormal nuclear characteristics including clumped chromatin patterns, intermixed with normal hepatocytes, were indicative for metastatic carcinoma or cholangiocellular carcinoma. The remaining biopsy samples were used for step 3.
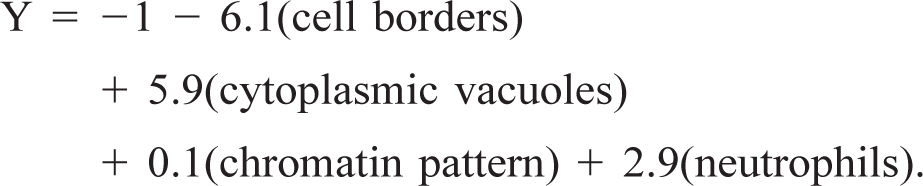
In step 3, a logistic regression was performed to distinguish normal liver biopsy samples from abnormal biopsy samples not diagnosed in step 1 or step 2. Those variables with a P-value less than 0.2 on univariate regression score were included in the model. With the multiple regression model, only parameters cell borders, vacuoles in cytoplasm, chromatin pattern, and presence of neutrophils were considered significant. The following regression formula was calculated:
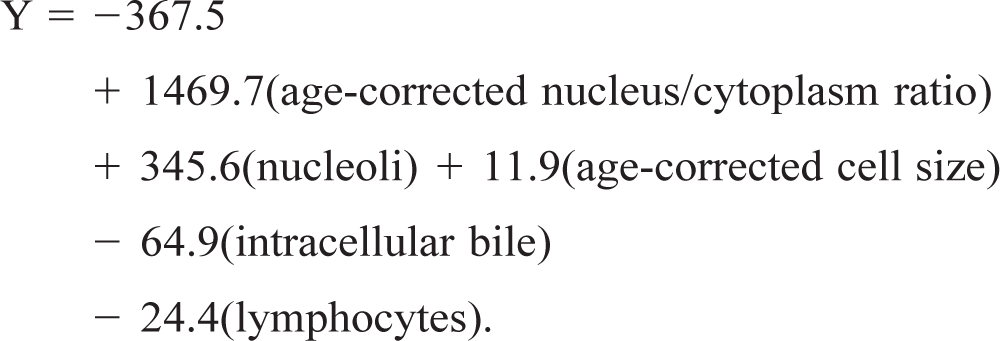
In step 4, a logistic regression was performed to distinguish hepatocellular carcinoma from other abnormal biopsy samples not diagnosed in steps 1 through 3. Those variables with a P-value less than 0.2 on univariate regression score were included in the model. With the multiple regression model, only parameters age-corrected nucleus/cytoplasm ratio, age-corrected cell size, number of nucleoli per nucleus, intracellular bile pigment content, and number of lymphocytes were considered significant. The following regression formula was calculated:
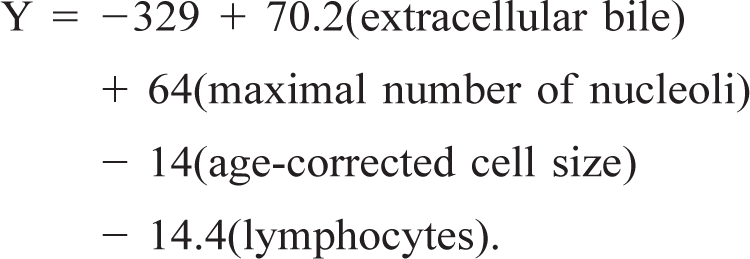
In step 5, a logistic regression was performed to distinguish acute or chronic extrahepatic cholestasis from other abnormal biopsy samples, not diagnosed in step 1 through step 4. Those variables with a P-value less than 0.2 on univariate regression score were included in the model. With the multiple regression model, only parameters extracellular bile, maximal number of nucleoli, age-corrected cell size, and presence of lymphocytes were considered significant. The following regression formula was calculated:
In step 6 a logistic regression was performed to distinguish destructive cholangiolitis from other abnormal biopsy samples not diagnosed in step 1 through step 5. Those variables with a P-value less than 0.2 on univariate regression score were included in the model. With the multiple regression model, only parameters numbers of neutrophils and mean nuclear size were considered significant. The following regression formula was calculated:

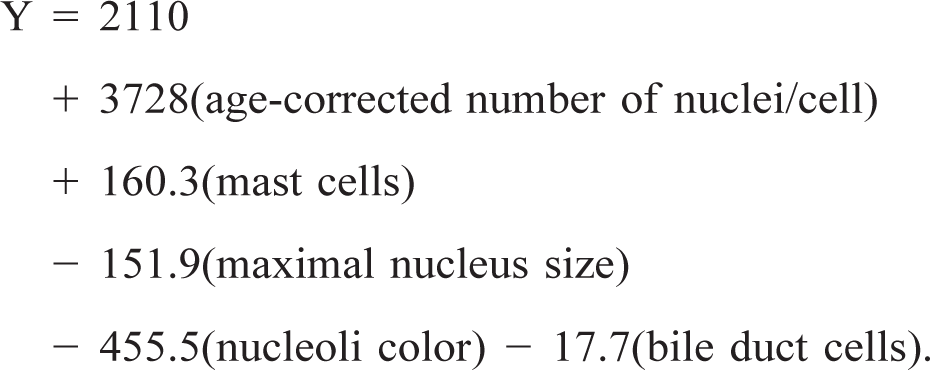
In step 7, a logistic regression was performed to distinguish nonspecific reactive hepatitis samples from other abnormal biopsy samples not diagnosed in steps 1 through 6. Those variables with a P-value less than 0.2 on univariate regression score were included in the model. With the multiple regression model, only parameters age-corrected number of nuclei per cell, presence of mast cells, maximum size of the nucleus, color of the nucleoli, and number of groups of bile duct cells were significant. The following regression formula was calculated:
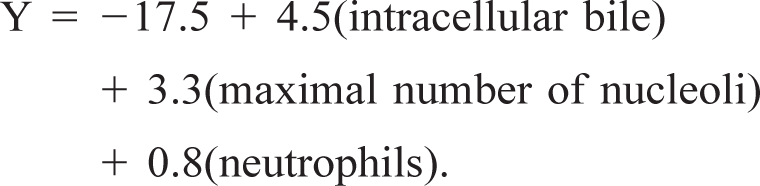
In step 8, a logistic regression was performed to distinguish acute hepatitis from CH. Because of the decreasing number of cases left, only those variables with a P-value less than 0.15 on univariate regression score were included in the model. With the multiple regression model, only parameters intracellular bile pigment content, maximum number of nucleoli per nucleus, and number of neutrophils were considered significant. The following regression formula was calculated:
In step 9 a logistic regression was performed to decide if cirrhosis was present in addition to CH. Those variables with a P-value less than 0.1 on univariate regression score were included in the model. With the multiple regression model, only parameters intracellular bile pigment content and number of groups of cuboid bile duct cells were considered significant. The following regression formula was calculated:

Discussion
Although cytologic examination of liver biopsy samples is becoming more popular, objective cytologic criteria in different liver diseases in the dog have not until now been documented. In the literature, diagnostic criteria are based on histologic criteria or cytologic criteria extrapolated from human studies. Often, these studies did not separate key criteria from secondary criteria. Only rarely a statistical approach has been used to identify important cytologic criteria for a certain hepatic disease. 6 By using a stepwise approach, including regression analysis, this study was performed to identify the major cytologic criteria to differentiate between normal and abnormal liver tissue and between the different pathologic abnormalities.
A significant age influence had been observed in a previous study in healthy dogs for the cytologic parameters cell size, number of nuclei per cell, and nucleus/cytoplasm ratio. 25 These parameters were therefore age corrected before they were used in the statistical models of this survey.
In this study, lipidosis, steroid-induced hepatopathy and extramedullary hematopoiesis were not included in the regression analysis because these diseases can be easily detected cytologically and are frequently a sequel of other diseases. 4,5,14,19,24,26,27
The first step in the multistep approach was to exclude metastatic tumor disease. High numbers of lymphoblasts within the liver specimens support the diagnosis of malignant lymphoma. 16 In this study, the mean number of lymphoblasts was 50% of all nucleated cells present within the biopsy sample; however, in a few cases, the number of lymphoblasts was only 5%. This might be caused by partial tumor remission induced by previous prednisolone therapy or an unequal distribution of lymphoblasts within the liver, which can be missed by FNAB. Diagnosis might be further confused because small numbers of lymphoblasts among plasma cells and lymphocytes may sometimes be detected in patients with CH in this study.
Excessive numbers of mast cells or mast cells in sheets as well as mast cells with variable degrees of granulation are detectable in mast cell neoplasia. 4,16 Care should be taken not to overdiagnose mast cell tumors within the liver. In this study, mast cells could be detected in nearly every disease with higher numbers in nonspecific reactive hepatitis and destructive cholangiolitis. However, these mast cells were mostly well differentiated and appeared as individual cells and not in groups. Furthermore, scattered individual mast cells occur in liver aspirates of healthy dogs. 25 At the time of this study, histologically confirmed liver biopsy sample of a mast cell tumor was not available; therefore, this diagnosis was not included in the model.
In metastatic carcinoma, normal liver cells intermixed with a distinct population of epithelial cells exhibiting several criteria of malignancy can be detected. These tumors are sometimes difficult to distinguish from primary hepatic carcinoma because of tissue necrosis and reactive cell patterns of liver cells, and identification of the origin of metastatic carcinoma cells by cytologic examination is frequently not possible. 1,19 Cochand-Priollet et al. 9 observed in humans an overall diagnostic accuracy of cytology of 82.6% in the differentiation of primary and secondary hepatic neoplasia. The use of peroxidase-antiperoxidase staining technique and transmission electron microscopy can be further applied to cytologic specimens, rendering a more accurate diagnosis in selected cases. 21 In companion animals, diagnostic accuracy of cytology in the detection of epithelial tumor metastases is not known.
After exclusion of metastatic disease, the following step is used to decide whether abnormal cell patterns indicative for primary liver disease are present. Hepatic cell morphology and cell types in healthy dogs have already been described. 25 In this survey, less well-defined cell borders of the hepatocytes, cytoplasmic vacuolization, and more pronounced irregular chromatin morphology in addition to excessive numbers of neutrophils were significant criteria for the identification of primary hepatic disease. These cellular alterations and cell types can be detected in primary neoplastic as well as nonneoplastic hepatic diseases. For the inexperienced cytologist, liver cells can appear very aggressive in different forms of hepatitis and can be confused with hepatocellular carcinoma. 4,18
Cytologic diagnosis of hepatocellular carcinoma can be very difficult, particularly in well-differentiated cases. 19 In this study, liver cells in hepatocellular carcinoma were characterized by a high nucleus/cytoplasm ratio, larger cell diameters, increased numbers of nucleoli per nuclei, small numbers of cytoplasmic vacuoles, and small numbers of lymphocytes intermixed with hepatocytes. Other characteristics, which could occasionally be observed without reaching significance, were crowding of liver cells, significant cellular necrosis, and abundance of cells with irregular and frequently condensed chromatin patterns. Morphologic characteristics of pleomorphic liver cells also have been described in man, but in well-differentiated tumors, these criteria can be totally absent. 13 In human medicine, several criteria to distinguish well-differentiated hepatocellular carcinoma from inflammatory or regenerative conditions include cellular crowding with increased nucleus/cytoplasm ratio and enlargement of nucleoli, 11 thickened nuclear membrane, 8 nuclear vacuolization, 7 and giant cells containing multiple nuclei or cells with small satellite nuclei. 17 Berman and McNeill 3 emphasize that atypical cell populations should show uniformity in contrast to dysplastic cell conditions with markedly atypical cells adjacent to normal-appearing cells. An important diagnostic criterion of hepatocellular carcinoma in man may further be the accumulation of intracytoplasmic hyaline bodies 13, which were not detected in this study.
In this study, significant parameters for the detection of extrahepatic cholestasis included a high content of extrahepatic bile pigment in the form of biliary casts and an increased number of nucleoli within hepatocytes on the one hand and a decreased cell size of the hepatocytes and low numbers of lymphocytes on the other hand. Although large quantities of extracellular bile accumulations were detectable in extrahepatic cholestasis and destructive cholangiolitis, mild intra-hepatic accumulations could be found in other diseases, including acute hepatitis, nonspecific reactive hepatitis, and CH. The association of extracellular bile pigment accumulation with the presence of extrahepatic cholestasis is a nonspecific change that may occur either in extrahepatic bile obstruction or with intrahepatic cholestasis associated with hepatitis. 23
Further identification of destructive cholangiolitis is based on high numbers of neutrophils and small mean nuclear size of hepatocytes. Although these criteria also might be detectable in histologic slides, 28 it is difficult to determine whether pericholangiolar inflammatory reactions can be definitively diagnosed using cytologic criteria alone.
Diagnosis of acute forms of hepatitis like purulent and nonspecific reactive hepatitis was based on criteria that document moderate reactive nuclear patterns, increased numbers of inflammatory cells, excluding lymphocytes, and absence of increased numbers of bile duct groups. The frequency of inflammatory cells might be difficult to interpret if slides contain large amounts of blood. 22 In these cases consideration of the peripheral leukogram in conjunction with the cytologic observation may be helpful. 21 In this study, the presence of increased numbers of mast cells was indicative of nonspecific reactive hepatitis.
According to observations in human medicine in CH without cirrhosis, the appearance of high numbers of lymphocytes was obvious, whereas in CH with cirrhosis, fewer lymphocytes combined with increased numbers of cuboid biliary epithelial cells were detectable. 10,18,23 Although increased numbers of lymphocytes could be detected in every patient with CH, it is questionable, in the face of the heterogenous distribution of lymphocytes in CH, whether cytologic examination is sensitive enough to detect CH. Lymphocytes are frequently located within dense connective tissue deposits in portal areas inhibiting exfoliation of cells in cytologic biopsy samples. 29 In addition, because anatomic relationships are lost in cytologic preparations, zonal inflammatory reactions can easily be missed, whereas diffuse distribution of inflammatory cells are more likely detected. 22
Important cytologic criteria for the diagnosis of liver cirrhosis are intracellular bile accumulation and appearance of increased numbers of bile ductules, probably related to bile duct proliferation in liver cirrhosis. Although bile duct proliferation can occur in patients with liver cirrhosis, it can also occur in extrahepatic cholestasis and inflammatory conditions of the bile duct system. More specific morphologic criteria of CH and cirrhosis, including several types of necrosis, fibrosis, and formation of regenerative nodules, cannot be diagnosed using cytologic examination. It should be emphasized that CH and cirrhosis were the remaining groups in this stepwise logistic regression analysis. Of course, there exists more than the 11 liver diseases represented in this analysis, and in a larger series, it may prove necessary to apply additional criteria to diagnose CH. Another point is that we have used smears of parts of the histologic biopsy samples, which makes comparison between cytology and histology of the same specimen possible. However, in practice, cytologic specimens will usually be obtained by FNAB. It remains to be investigated whether this described multistep approach also is valid for fine-needle aspirates, which may be less representative of the true disease process.
In conclusion, this study demonstrated that key cytologic criteria of different hepatobiliary diagnoses can be identified in the dog using a stepwise logistic approach. Based on these results, diagnostic accuracy of cytologic liver examination in the dog by means of a multistep logistic regression method will need to be evaluated in a prospective study.