
Abstract
Heterobilharzia americana is a trematode of the Schistosomatidae family that infects dogs, raccoons, and other mammals as definitive hosts. This parasite is considered endemic in the southern Atlantic and Gulf coasts; however, only a few cases are reported. A 7-year-old dog from Louisiana was referred for persistent hypercalcemia, hyperglobulinemia, and weight loss. Abdominal ultrasound revealed diffuse hyperechogenicity of the liver with several hyperechoic nodules of varying size. Cytologic examination of fine-needle aspirates of the liver revealed few ovoid to round basophilic thin-walled eggshell fragments and rare ciliated miracidia. H. americana eggs were identified on fecal sedimentation.
Heterobilharzia americana is a trematode of the Schistosomatidae family. Despite H. americana being considered endemic in the Gulf and southern Atlantic coasts, only a few cases have been described in the literature, with the majority occurring in Texas and Louisiana. 7,8
The life cycle includes 2 hosts: the definitive hosts are dogs, raccoons, and other mammalian species, while the intermediate hosts are lymnaeid freshwater snails (Bakerilymnaea cubensis and Pseudosuccinea columella). As opposed to other trematodes, schistosomes are not hermaphrodites. The adult male and female parasites live in copula in the mesenteric veins. The eggs, which lack opercula and contain a ciliated miracidium, are released in the mesenteric venules, from which they migrate through the secretion of proteolytic enzymes to the intestinal lumen and are ultimately excreted in feces. Following contact with fresh water, the eggs rapidly release the ciliated miracidia, which actively seek and penetrate the soft mantle of the snail, where they mature into cercariae. Mature cercariae are released as free-swimming, fork-tailed cercariae. When these come into contact with the definitive hosts, they penetrate the hosts’ intact skin, lose their tails, and migrate through the blood vessels to the lungs and to the liver, where they mature into adults and finally locate in the mesenteric veins. 2,7
Aberrant migration of the eggs in the definitive host may lead to infection of the liver and other organs, producing variable degrees of granulomatous inflammation and fibrosis. 8 In this article, we describe the first case of H. americana infection diagnosed by cytologic examination of fine-needle aspirates of the liver of an infected dog.
A 7-year-old male neutered Longhaired Dachshund from Louisiana was referred to the Louisiana State University Veterinary Teaching Hospital internal medicine service for a 3-month history of lethargy, decreased appetite, weight loss, marked hypercalcemia, and marked hyperglobulinemia. Radiographs performed at that time showed no abnormalities. The dog was treated with glucocorticoids twice prior to referral, with mild improvement followed by relapse of clinical signs each time. In addition, the hypercalcemia and hyperglobulinemia persisted through multiple visits to the referring veterinarian.
On presentation at Louisiana State University Veterinary Teaching Hospital, the dog was quiet and alert. He was thin, with a body condition score of 3 of 9 and had lost 1.2 kg over the past 3 months. The remainder of his physical examination was unremarkable. Complete blood count revealed a mild normocytic normochromic nonregenerative anemia (packed cell volume, 34%; reference interval [RI], 37%–55%; reticulocytes 21900/µl) consistent with anemia of inflammatory disease and a stress leukogram with mild leukopenia (7600/μl; RI, 8000–14500/μl) characterized by mild lymphopenia (800/μl; RI, 1000–4800/μl). The serum biochemistry panel confirmed the presence of marked hypercalcemia (16.9 mg/dl; RI, 9.4–11.4 mg/dl) and marked hyperglobulinemia (6.9 g/dl; RI, 2.5–4.0 g/dl). Mild hypoglycemia (67 mg/dl; RI, 80–115 mg/dl) and mild hypocholesterolemia (95 mg/dl; RI, 150–240 mg/dl) suggested decreased hepatic functional mass. Blood urea nitrogen was marginally increased (33 mg/dl; RI, 8–22 mg/dl), while the creatinine was within the RI. Electrolyte abnormalities included minimal hyponatremia (139 mmol/l; RI, 140–153 mmol/l), mild hypochloremia (103 mmol/l; RI, 107–115 mmol/l), mild hypokalemia (3.6 mmol/l; RI, 3.8–5.5 mmol/l), mild hypophosphatemia (2.6 mg/dl; RI, 3.4–6.3 mg/dl), and mild hypomagnesemia (1.5 mg/dl; RI, 1.7–2.2 mg/dl) secondary to possible gastrointestinal or renal loss. The urinalysis showed a urinary specific gravity of 1.013, pH 6.0, and several calcium oxalate dihydrate crystals on the urinary sediment. A cervical ultrasound was performed to evaluate thyroid and parathyroid glands and was unremarkable. No abnormalities were noted on thoracic radiographs, whereas abdominal radiographs revealed an enlarged liver. Ultrasonographic examination of the abdomen revealed diffuse hyperechogenicity of the liver with several hyperechoic nodules of varying size. Both kidneys showed decreased corticomedullary definition with presence of several nephroliths bilaterally in renal cortices. The urinary bladder had hyperechoic sediment, which was consistent with the several calcium oxalate crystals seen in the urinary sediment. The submucosal layer of the jejunum appeared diffusely thickened, and a focal area of thickening of the wall of the descending colon was observed. Portal and jejunal lymphadenopathy was present. Fine-needle aspirates of the liver were submitted for cytologic examination.
The fine-needle aspirates from the liver were highly cellular with mild hemodilution. They contained several variably sized clusters of uniform hepatocytes, which occasionally contained small amounts of intracytoplasmic dark green granular pigment consistent with either bile or lipofuscin. Scattered among these clusters were few basophilic, ovoid (approximately 70–150 × 40–60 µm) to round (approximately 50–60 µm in diameter) to irregularly shaped, thin-walled structures consistent with parasite eggshell fragments (Figure 1). Additionally, rare ovoid organisms (approximately 80–140 × 50–70 µm) surrounded by many thin cilia (∼20 µm long) consistent with ciliated miracidia were observed (Figures 2 and 3). The internal structure of the miracidia consisted of aggregates of many dense nuclear-like particles (4–6 µm) contained in a pale basophilic material. Miracidia displayed variable numbers of round, deeply basophilic structures (∼20–30 µm in diameter). A moderate amount of extracellular dark yellow to brown granular pigment consistent with hematin was often present in proximity of these structures and diffusely in the background. Several spindle-shaped mesenchymal cells displaying mild to moderate anisocytosis and anisokaryosis were also present, along with moderate numbers of macrophages and fewer neutrophils and small lymphocytes (Figure 4). Rare variably sized and shaped crystals suggestive of soft tissue mineralization were seen in the background.
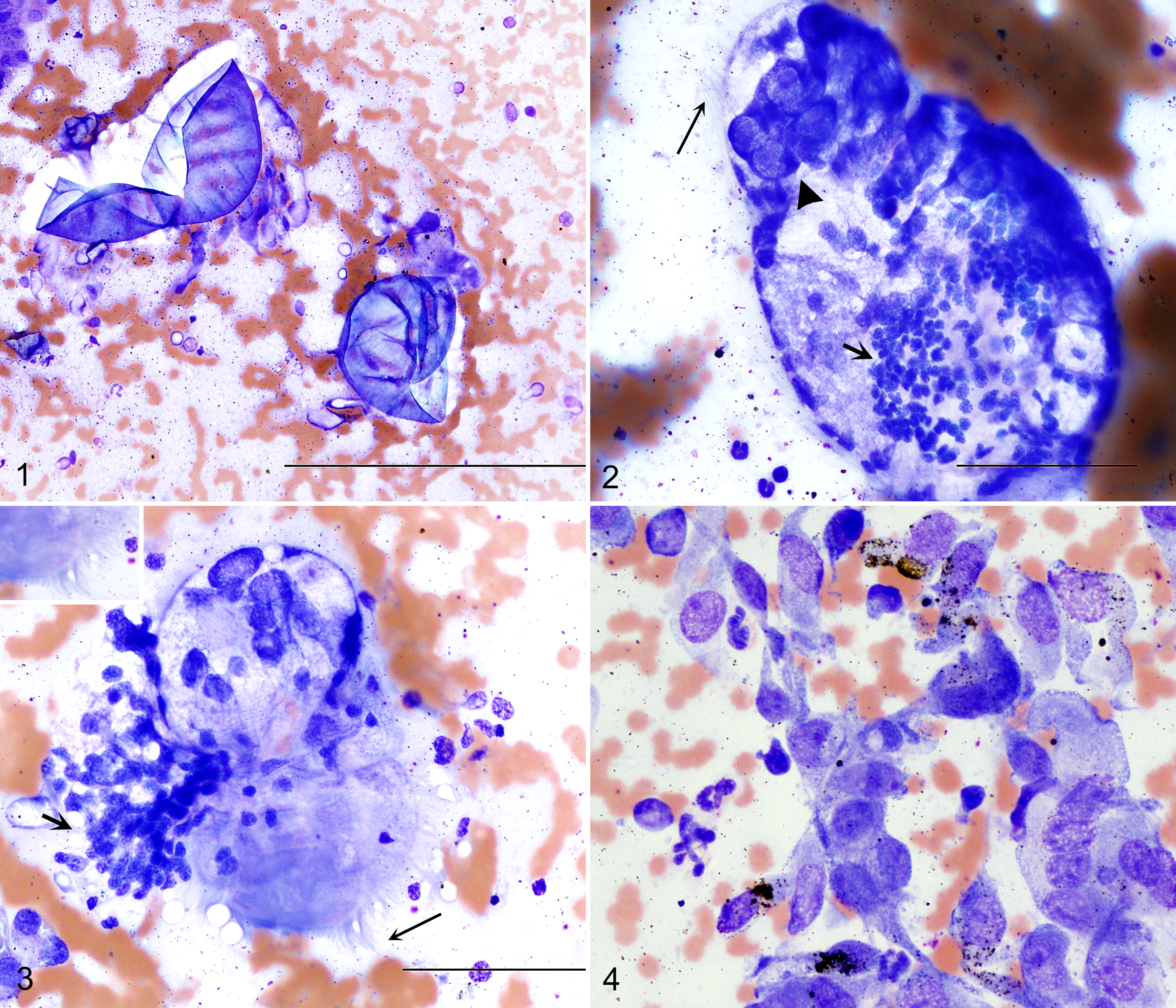
Heterobilharzia americana infection, liver, dog. Fine-needle aspirate, Wright-Giemsa.
A diagnosis of parasitic infection with granulomatous inflammation and fibrosis was made. The most likely cause was H. americana, and a fecal sedimentation was recommended. H. americana eggs were identified on fecal sedimentation as 70–90 µm in diameter, thin-walled, nonoperculated, miracidia-laden eggs. Parathyroid hormone–related protein (PTHrP) levels were additionally measured to assess the persistent hypercalcemia; however, the results were within RI. The dog was placed on intravenous fluids at 25 ml/h to promote diuresis and calcium excretion. He was treated with fenbendazole (50 mg/kg/d) for 10 days, metronidazole (15 mg/kg/d), and calcitonin (8 mg/kg) subcutaneously every 8 hours.
Diagnosis of H. americana typically requires visualization of eggs with fecal sodium chloride sedimentation. Fecal sedimentation is not routinely performed in private practices; moreover, the intermittent shedding of eggs decreases the sensitivity of coprologic examination. 1 Polymerase chain reaction is available for testing on feces, liver, and intestinal biopsies (Gastrointestinal Laboratory at Texas A&M University, www.vetmed.tamu.edu/gilab). Histopathology and cytologic examination of liver and other affected tissues may also reveal the presence of eggs and parasites.
Clinical signs of H. americana infection are typically associated with gastrointestinal disease and include decreased appetite, weight loss, vomiting, and diarrhea. 2 Additional clinical signs are related to migration through tissues and include dermatitis secondary to penetration of the cercaria through the skin and coughing secondary to lung migration. 4,10 Hypercalcemia has been described in about half of the reported cases. Fradkin et al described 2 cases of H. americana infection with severe hypercalcemia secondary to increased PTHrP. 3 The mechanism by which this trematode induces increased PTHrP is unclear, as is the pathogenesis of hypercalcemia in this case without an increase of PTHrP. In the remaining cases, hypercalcemia of granulomatous disease has been hypothesized. Hypercalcemia of granulomatous disease is believed to be secondary to increased production of 1, 25-dihydroxyvitamin D3 from tissues other than kidneys, although 1, 25-dihydroxyvitamin D3 has inconsistently been reported elevated. 3,5,9 A persistent severe hypercalcemia and hyperglobulinemia characterized the clinical history of the present case. As the cervical ultrasound and the PTHrP were normal, we believe that the hypercalcemia was most likely secondary to the granulomatous inflammation, whereas the hyperglobulinemia was secondary to antigenic stimulation caused by the eggs and adult parasites.
In the cytologic specimen, variable numbers of round, deeply basophilic structures of approximately 20–30 µm in diameter, often in close proximity to one another, were observed on the miracidia. These likely represent apical papilla with sucker-like cups. The sucker-like pad of schistosomes’ miracidia has been identified by scanning microscopy in Schistosoma japonicum and Schistosoma haematobium and is believed to facilitate the attachment and penetration of the snail dermis. 6
Cytologic examination of the fine-needle aspirates of the liver demonstrated the presence of a mesenchymal cell population with moderate dysplasia that was interpreted as fibrosis, although a concomitant mesenchymal neoplasm could not be completely ruled out. Histopathologic evidence of fibrosis was detected in approximately 30% of liver and intestinal biopsies and, with granulomas, represents the most common histopathologic change in liver of dogs infected with H. americana. 8
Cytologic identification of ciliated miracidia and thin-walled eggshell fragments in this case was essential for the diagnosis of H. americana infection. This case demonstrates how cytology represents a valid and rapid diagnostic method for diagnosing canine schistosomiasis. It also provides a detailed cytologic description of the organisms, as a reference for clinicians, parasitologists, and pathologists reviewing cytologic specimens from infected dogs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.