
Abstract
Canine chronic hepatitis (CCH) is a progressive inflammatory disease of unknown etiology. To characterize the inflammatory infiltrate, 16 dogs with CCH were selected and classified into three groups based on the stage of fibrosis, as evaluated with Masson's trichrome stain. The inflammatory infiltrate in each liver section was immunohistochemically characterized and evaluated using CD3, lysozyme, λ and κ light chain, and α-smooth muscle actin antibodies. Numerous breeds were affected, and middle-aged females predominated in this select group. Necroinflammatory activity progressively increased and then waned as the hepatitis progressed to cirrhosis. CD3+ lymphocytes were the most numerous lymphoid cells in dogs with CCH. Degenerate hepatocytes were occasionally surrounded by CD3+ lymphocytes. Necrosis was positively correlated with the number of CD3+ lymphocytes. The λ and κ light chain-positive cell infiltrate was variable but generally mild. A positive correlation between the λ and κ light chain-positive cells and the portal α-smooth muscle actin was found. The number of α-smooth muscle actin-positive cells (myofibroblasts) in portal triads and fibrous septa was positively correlated with the stage of fibrosis. In contrast, no correlation was found between the number of lysozyme-positive cells (Kupffer cells) and the stage of fibrosis. These results further support the idea of an immune-mediated process in CCH and suggest that periductular myofibroblasts play an important role in canine liver fibrogenesis.
Canine chronic liver disease encompasses various forms of chronic hepatitis and cirrhosis whose etiopathogenesis is still obscure. In spite of the diagnostic arsenal currently available, most of the cases of canine chronic liver disease remain idiopathic. 6 Several infectious and noninfectious causes have been suggested for chronic liver disease, such as canine adenovirus type 1 (CAV-1), Leptospira interrogans var. grippotyphosa, canine acidophil cell hepatitis virus, copper accumulation, drug administration, alpha-1-antitrypsin anomaly, and autoimmunity. 4,8,12,13,16,20,23,28 Despite variable etiologies, cases of canine chronic hepatitis (CCH) share similar histologic changes, including piecemeal necrosis, inflammation, and progressive fibrosis that evolves into cirrhosis. Over the years, CCH has been classified histomorphologically as chronic active hepatitis, chronic progressive hepatitis, and lobular dissecting hepatitis. 3,10,11,26
Four decades of histologic and immunopathologic investigations have led to remarkable progress in the understanding of chronic human liver diseases. An understanding of the composition of the inflammatory infiltrate and its relationship to the evolution of human hepatitis has been very helpful for determining the pathogenesis of liver disease. The importance of histology and immunopathology as prognostic values has largely been shown in human cases of liver disease. 1,9,18
CCH has been widely described histologically, but there is a paucity of information regarding the exact nature of the inflammatory infiltrate. The aims of the present study were to define the nature of the lymphoid cells involved in CCH and to look for correlations between the stage of fibrosis and the presence of lymphoid cells, Kupffer cells, neutrophils, and myofibroblasts in selected dogs with CCH.
Materials and Methods
Case selection
All biopsy and necropsy cases of CCH and cirrhosis diagnosed at the Service de Diagnostic of the Faculté de Médecine Vétérinaire, Université de Montréal, from January 1986 to May 1998 were reviewed. The histologic criteria used for selection of the cases were adapted from a definition suggested by the International Association of the Study of the Liver and by the World Congress of Gastroenterology; these criteria included piecemeal necrosis, portal and periportal fibrosis, and portal to periportal necroinflammatory activity. 2 Histologic criteria for cirrhosis included nodular regeneration with progressive bridging fibrosis associated with inflammation. Sixteen dogs with idiopathic chronic hepatitis were selected on the basis of these criteria and on the absence of a specific cause and were classified into three groups based on the stage of fibrosis (1 = mild portal fibrosis; 2 = moderate portal fibrosis with mild periportal and septal fibrosis; 3 = severe portal fibrosis with marked periportal and septal fibrosis or cirrhosis). Normal liver sections obtained from five dogs without evidence of infectious, neoplastic, or cardiac disease were used as controls.
Histopathology
All liver samples were fixed in 10% buffered formalin, routinely processed, and embedded in paraffin. Four-micrometer sections were cut and stained with hematoxylin, phloxin, and saffron (HPS) and with Masson's trichrome for light microscopic examination.
Immunohistochemical procedure
In canine liver, anti-CD79 (Hm57) antibody was very indiscriminant and stained hepatocytes and smooth muscle cells as well as B lymphocytes. Trials to block this background staining were unsuccessful; therefore, λ and κ light chain antibodies were used.
Each liver was evaluated for the expression of CD3, λ and κ light chains, lysozyme, and α-smooth muscle actin using an avidin–biotin peroxidase complex (ABC) technique (Vector Laboratories, Burlingame, CA). Four-micrometer sections were mounted on poly-
Quantitative and semiquantitative analyses
CD3+ cells, κ and λ light chain–positive cells, and neutrophils were counted in 12 randomly selected portal areas (40×) and 12 lobular areas (20×) of liver for each slide. Fibrous septa were considered extensions of portal triads. Cells were always counted by the same two observers in agreement (J. Boisclair and C. Girard). The median was determined for portal space and lobular area for each cell type.
Semiquantitative scoring was done by two observers in agreement (L. Chouinard and C. Girard or J. Boisclair and C. Girard). Necroinflammatory activity and cholestasis were semiquantitatively scored as absent (0), mild (1), moderate (2), or severe (3). Inflammation was evaluated regardless of cellular type. Bile duct proliferation was also semiquantitatively scored as absent (0), mild (less than three bile ducts per portal space, 1); moderate (three to five bile ducts per portal space, 2); and severe (more than five bile ducts per portal space, 3). Semiquantitative analysis (J. Boisclair and C. Girard) was also used to grade the expression of α-smooth muscle actin (0 = absence; 1 = weak and multifocal; 2 = moderate; and 3 = strong) and lysozyme (0 = very few Kupffer cells; 1 = some Kupffer cells; 2 = moderate number of Kupffer cells; and 3 = numerous Kupffer cells). The α-smooth muscle actin was scored for portal tracts including fibrous septa and lobular areas. To assess Kupffer cells, lysozyme was scored in sinusoids only.
Statistical analysis
To compare groups, the Kruskal–Wallis H-test was applied. When the differences were significant, the Wilcoxon Mann–Whitney U-test using comparison-related significance levels was performed for all pairs of groups. Results were also analyzed by Spearman's correlation test to verify a possible association between histologic changes and numbers of inflammatory cells. A nominal significance level of P < 0.05 was used.
Results
Characteristics of selected dogs
Sixteen dogs with CCH or cirrhosis were grouped based on the stage of fibrosis (Figs. 1–4). Characteristics of affected dogs and controls are presented in Table 1. The mean age of affected dogs was 5.5 years (range 1–13 years). Females were overrepresented (10 females, six males). Ages of control dogs ranged from 3 to 5 years (○ = 3.8 years), and there were three males and two females.
Breed, sex, and age of control dogs and dogs with chronic hepatitis.
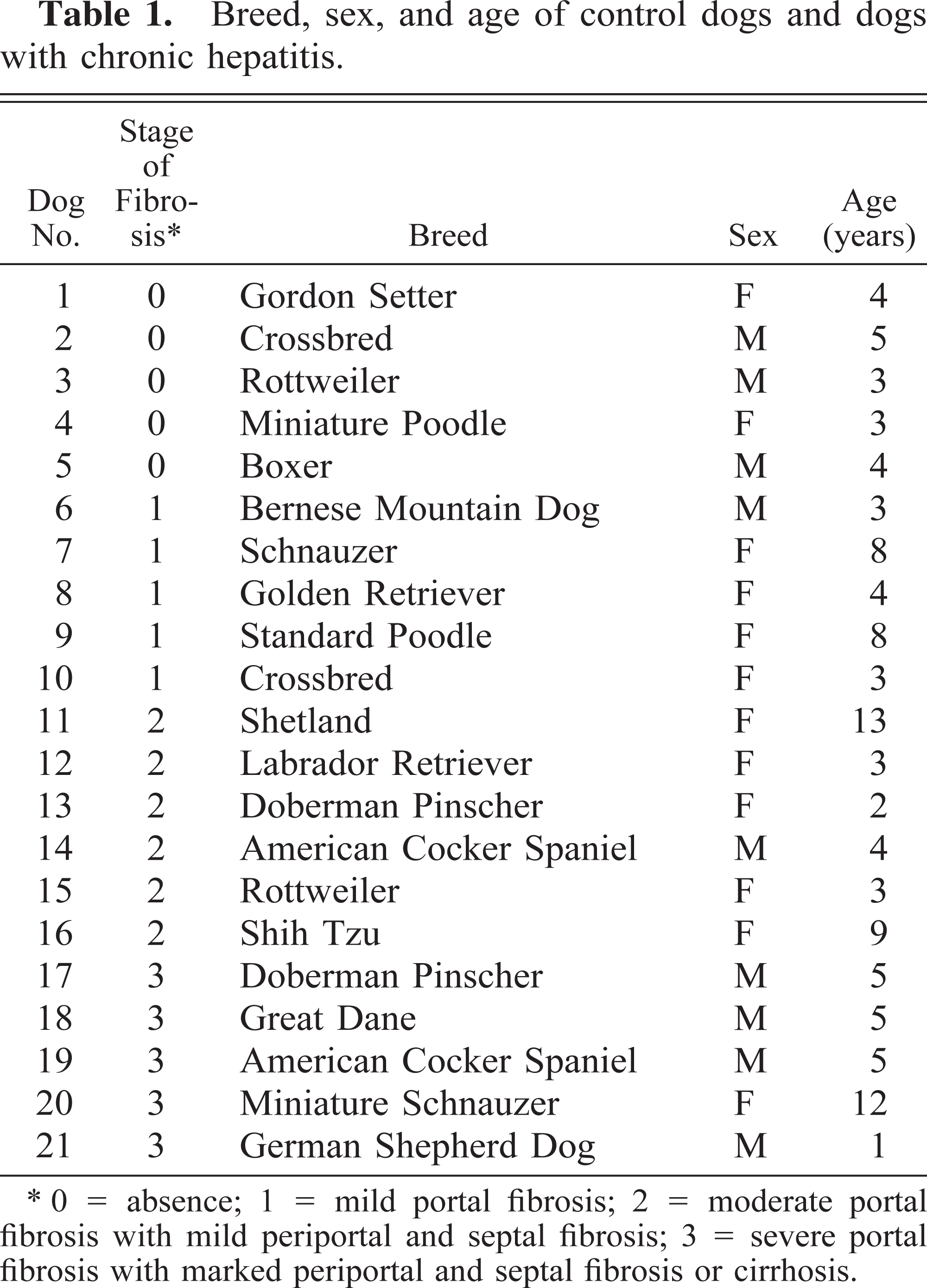
∗ 0 = absence; 1 = mild portal fibrosis; 2 = moderate portal fibrosis with mild periportal and septal fibrosis; 3 = severe portal fibrosis with marked periportal and septal fibrosis or cirrhosis.
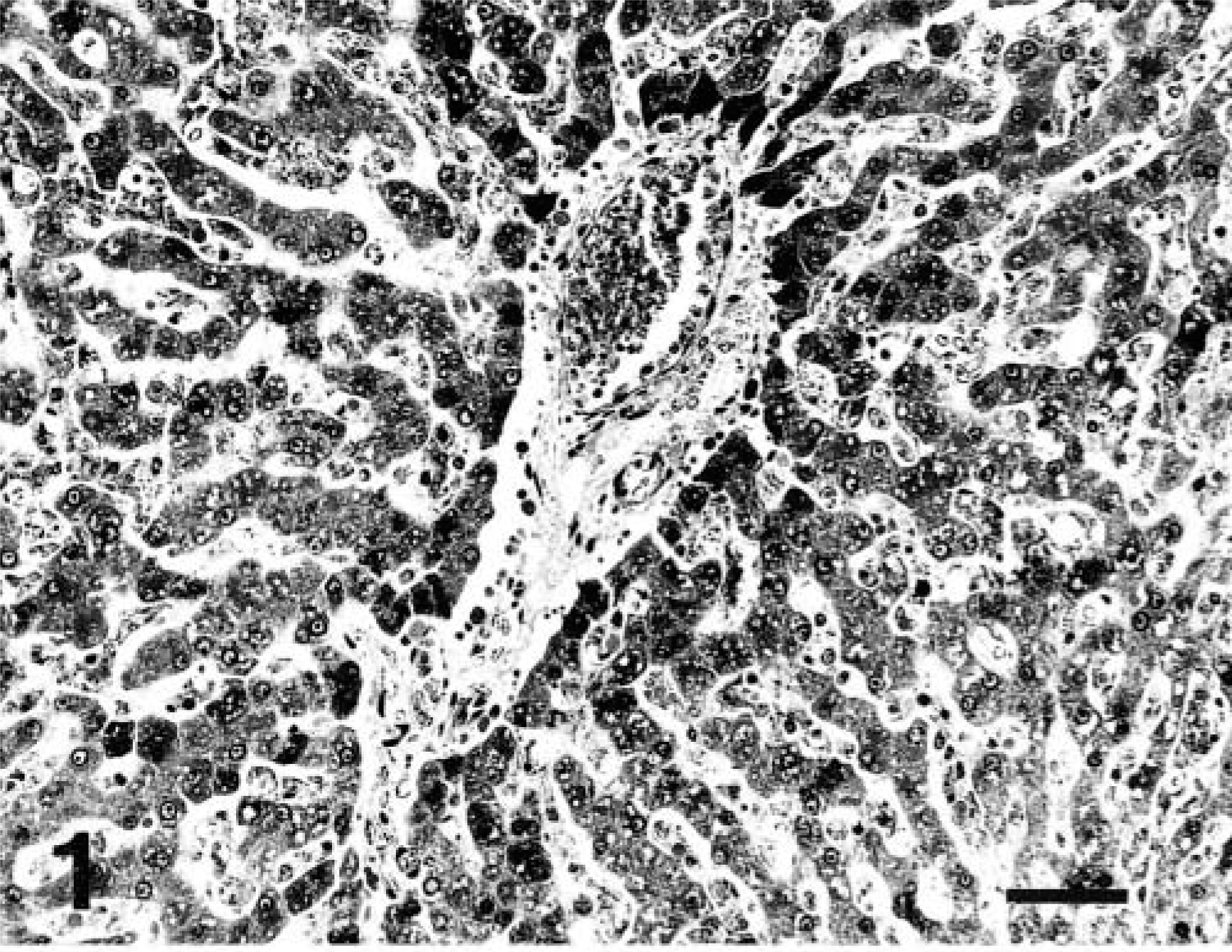
Liver; control dog No. 2. Masson's trichrome. Bar = 50 µm.
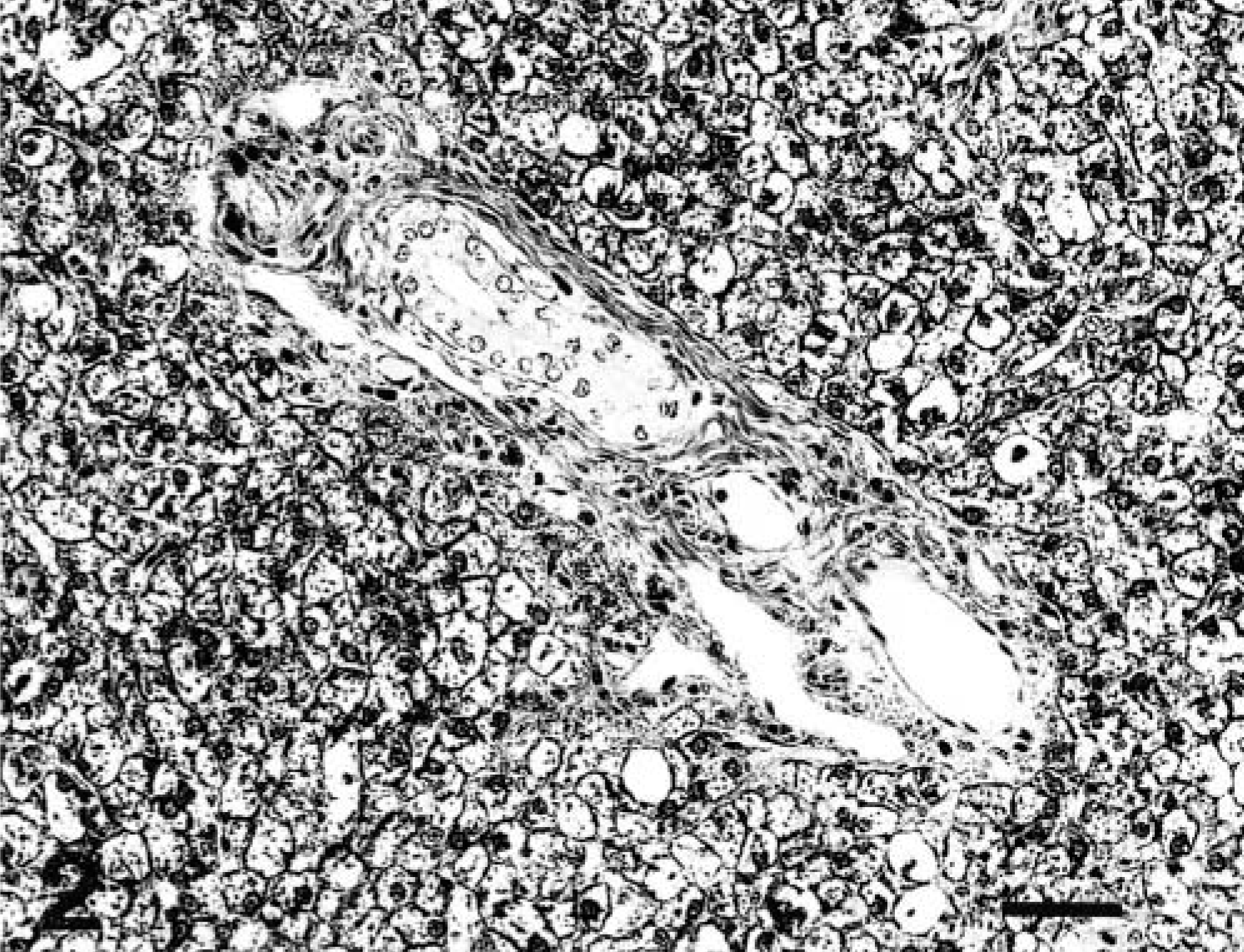
Liver; dog No. 7. Stage 1 fibrosis. There is a slight expansion of portal space by fibrous tissue. Masson's trichrome. Bar = 50 µm.
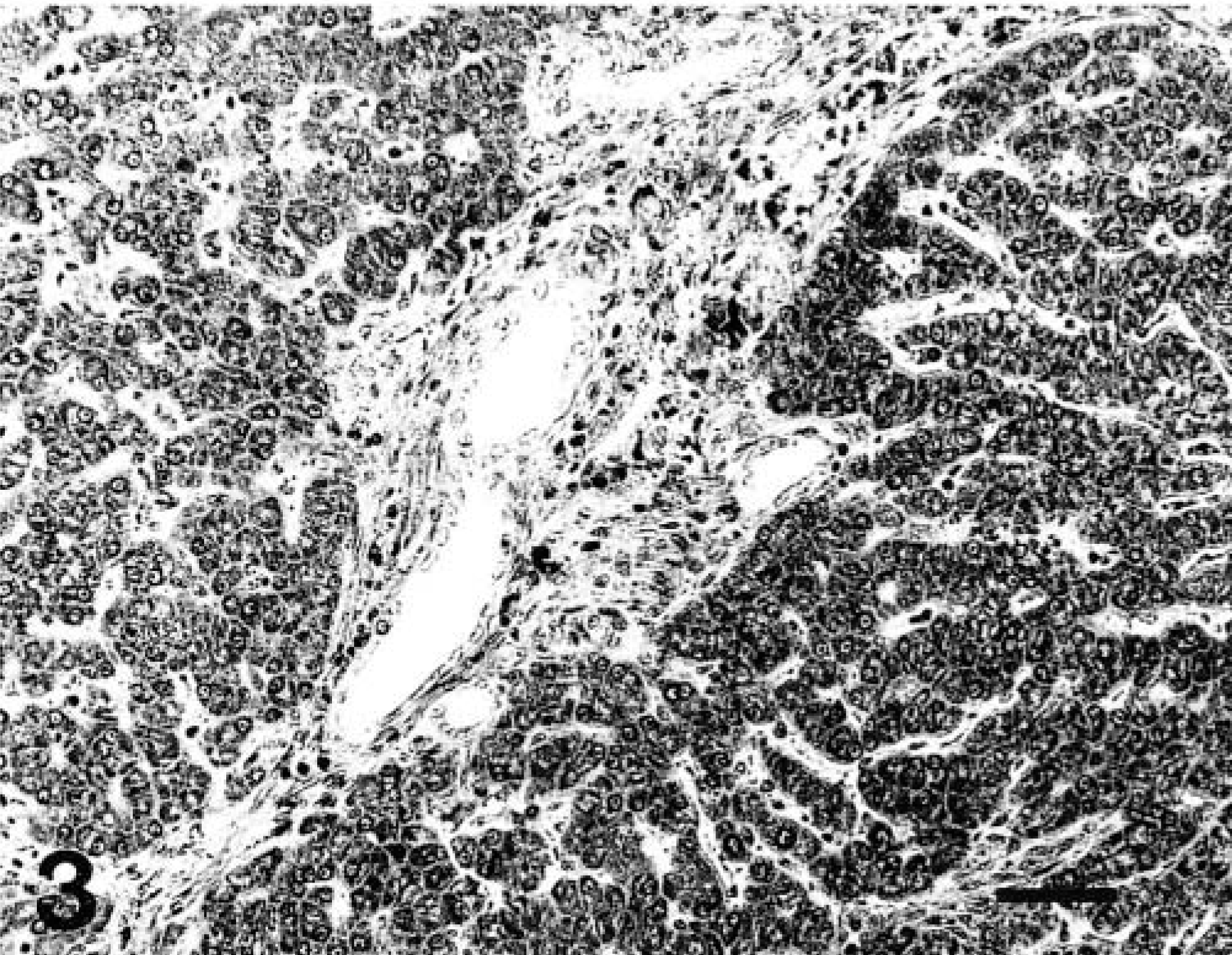
Liver; dog No. 11. Stage 2 fibrosis. There is moderate portal fibrosis with mild periportal and septal fibrosis. Masson's trichrome. Bar = 50 µm.
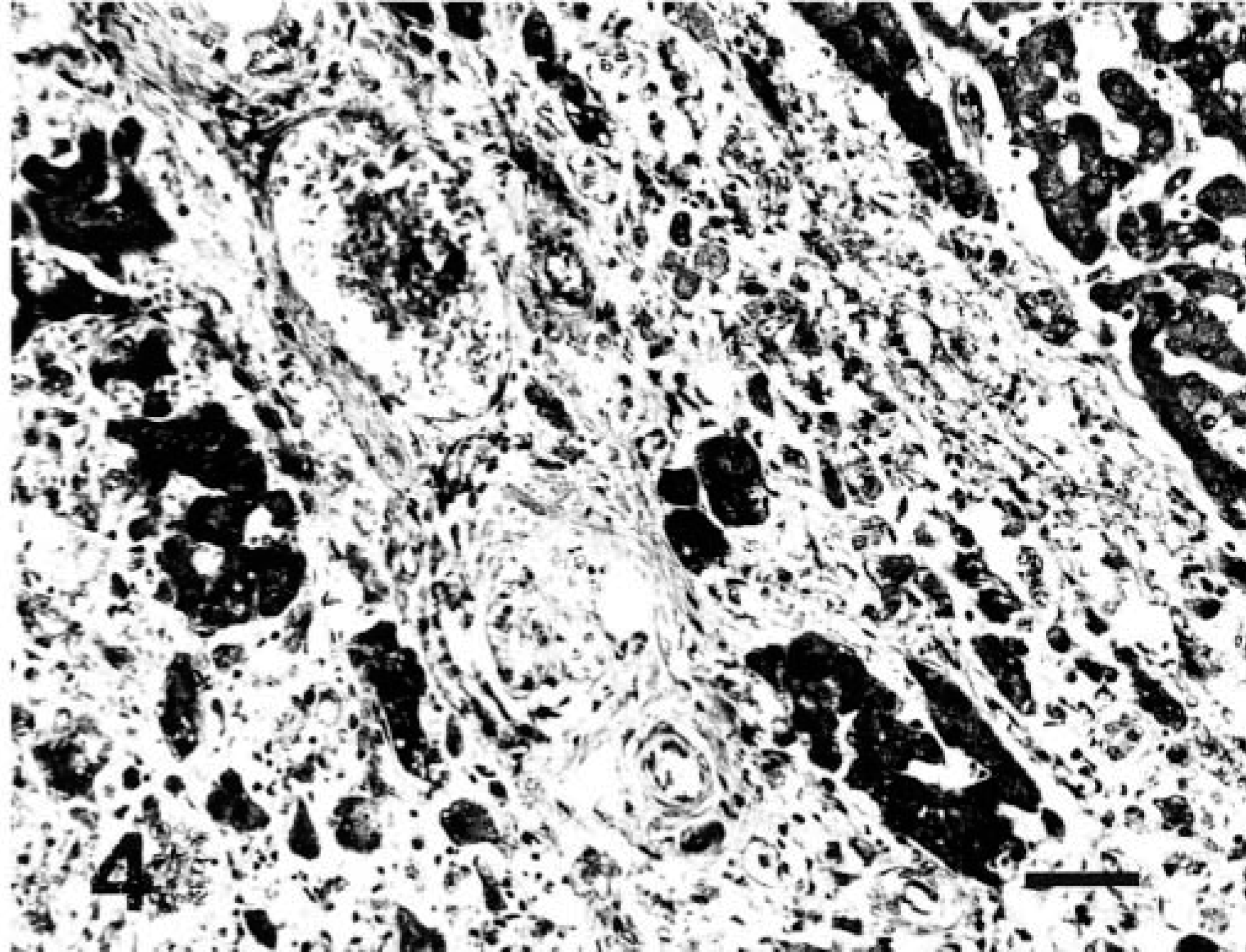
Liver; dog No. 18. Stage 3 fibrosis. Portal spaces are severely expanded by fibrous tissue that extends intralobularly, dissecting hepatocytes and surrounding a hyperplastic nodule. Masson's trichrome. Bar = 50 µm.
Immunohistochemistry
CD3+ lymphocytes were the most numerous lymphoid cells observed in portal triads of affected dogs. Numbers of CD3+ cells varied greatly among portal triads for a given individual and among individuals within a group. In lobular areas, CD3+ lymphocytes were more numerous in proximity of centrilobular veins. Randomly distributed round, intensely eosinophilic hepatocytes surrounded by CD3+ lymphocytes were seen in eight dogs, all with stage 1 or 2 fibrosis (Fig. 5). No CD3+ lymphocytes were seen in hepatic lobular areas and portal triads of control dogs, except a few CD3+ lymphocytes in portal spaces of one animal.
Liver; dog No. 13. Stage 2 fibrosis. Intensely eosinophilic hepatocyte is surrounded by CD3+ lymphocytes. ABC method, CD3 antibody, Mayer's hematoxylin counterstain. Bar = 30 µm.
Intralobular λ and κ light chain–positive cells were not evaluated because of the difficulty of differentiating intrasinusoidal from intralobular cells. Generally, λ light chain–positive cells were more numerous than κ light chain–positive cells. Numbers of λ and κ light chain–positive cells differed greatly among portal triads for a given individual and among individuals within a group, but this infiltrate was generally mild compared with CD3+ lymphocytes. As for CD3, very few λ and κ light chain–positive cells were observed in hepatic portal triads of some controls.
Lysozyme antibody stained neutrophils as well as macrophages, monocytes, and Kupffer cells. To assess Kupffer cells, only intrasinusoidal stellate or fusiform lysozyme-positive cells were evaluated. The distribution of intrasinusoidal lysozyme-positive cells in controls was mainly perilobular. There was no particular distribution in affected dogs.
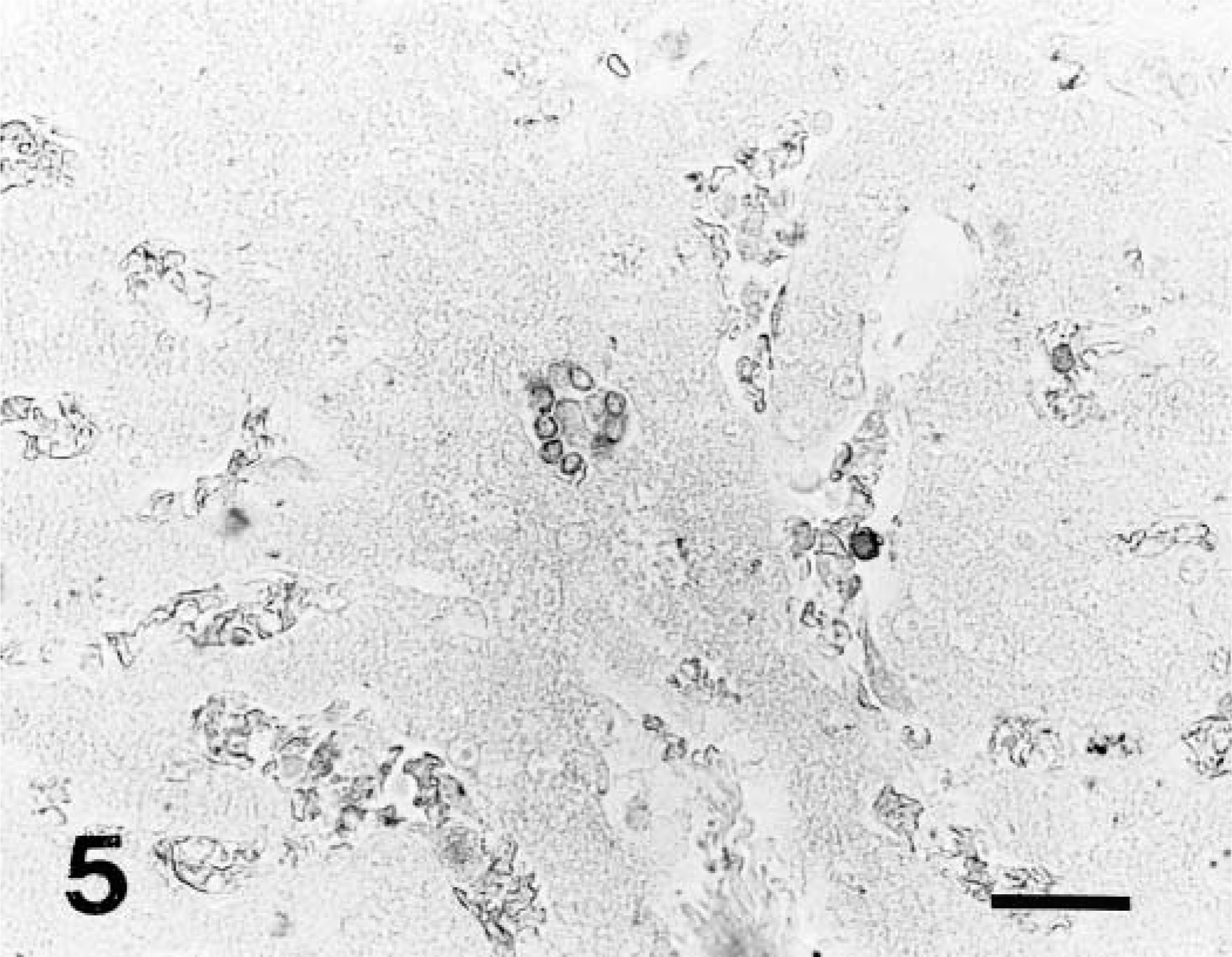
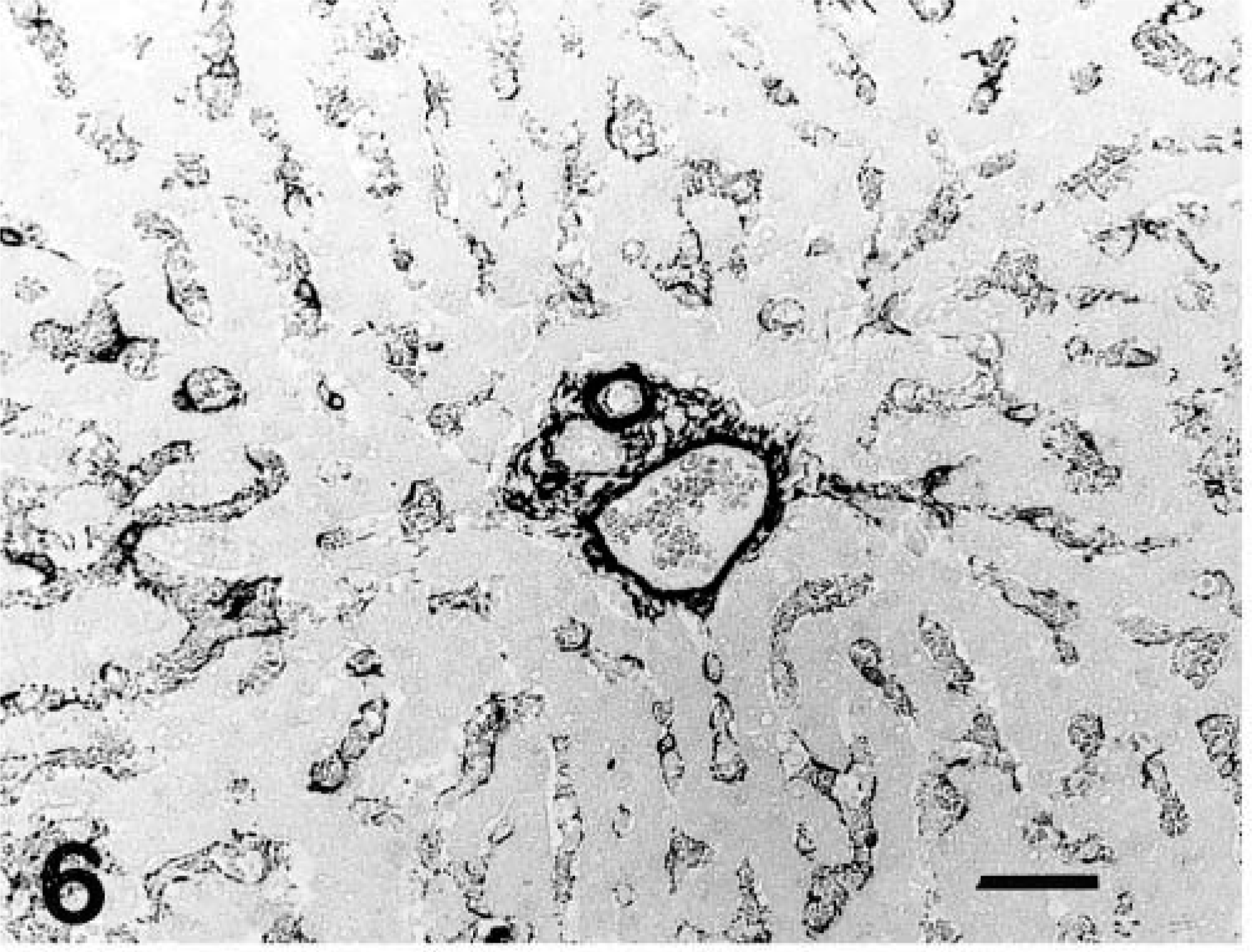
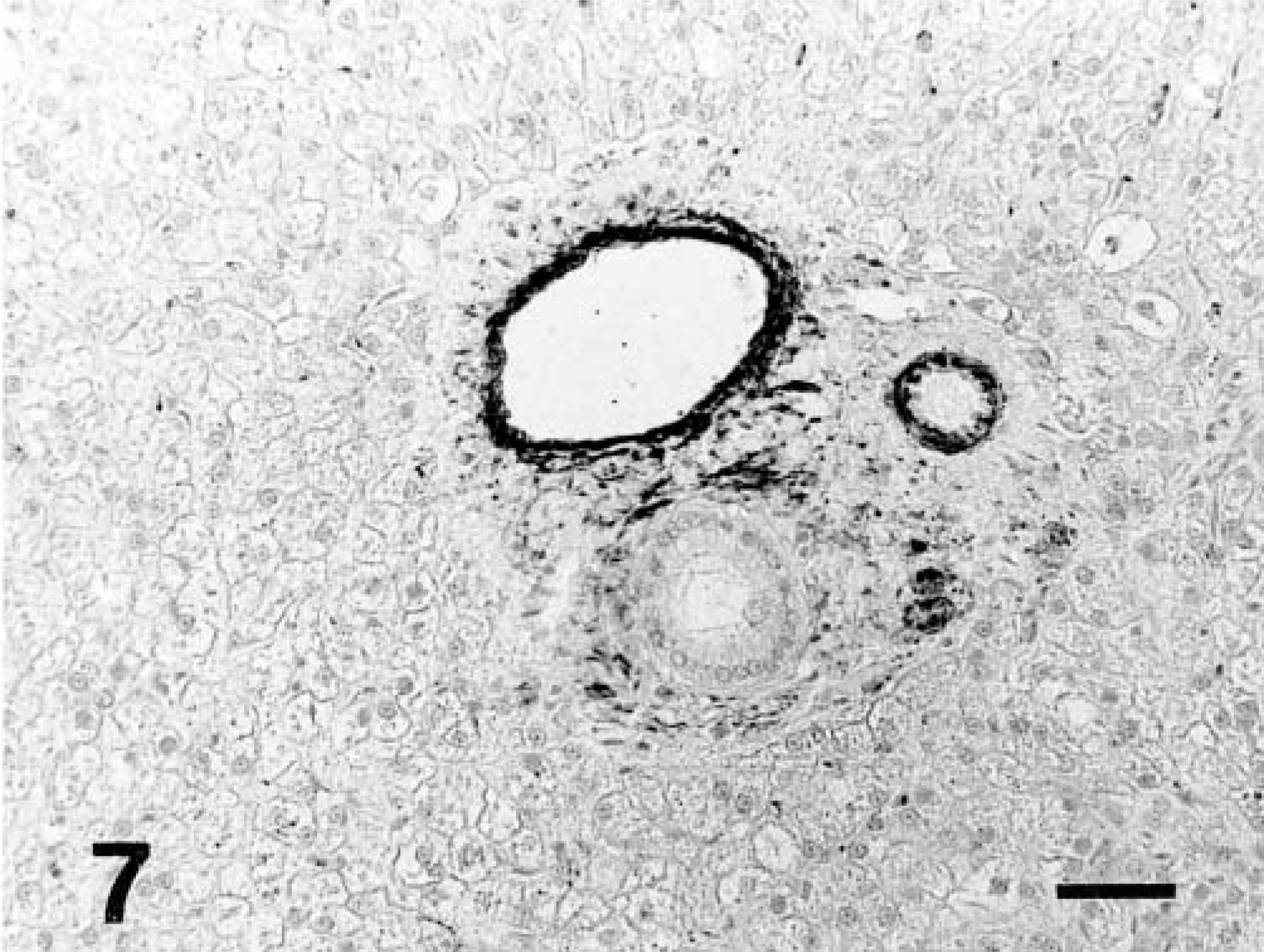
Intralobular α-smooth muscle actin positivity was mainly linear, fine, and bordering the perisinusoidal space (Fig. 6). Intralobular distribution of α-smooth muscle actin–positive cells was diffuse in controls, compared with the irregular distribution observed in fibrotic livers; some lobules contained numerous α-smooth muscle actin–positive cells, whereas only a few positive cells were seen in other lobules. In nonfibrotic areas of affected livers, the number of sinusoidal α-smooth muscle actin–positive cells was similar or reduced compared with controls. Positivity was often reduced or absent in foci of nodular hyperplasia. Few α-smooth muscle actin–positive cells were noted around blood vessels in the portal space of controls. In livers showing chronic hepatitis, numerous α-smooth muscle actin–positive cells were observed in and around enlarged portal areas and in fibrous septa (Figs. 7–9).
Liver; control dog No. 2. Intralobular α-smooth muscle actin reaction is mainly linear, fine, and bordering the perisinusoidal space. ABC method, α-smooth muscle actin antibody, Mayer's hematoxylin counterstain. Bar = 50 µm.
Liver; dog No. 13. Stage 1 fibrosis. No sinusoidal α-smooth muscle actin–positive cells are observed. ABC method, α-smooth muscle actin antibody, Mayer's hematoxylin counterstain. Bar = 50 µm.
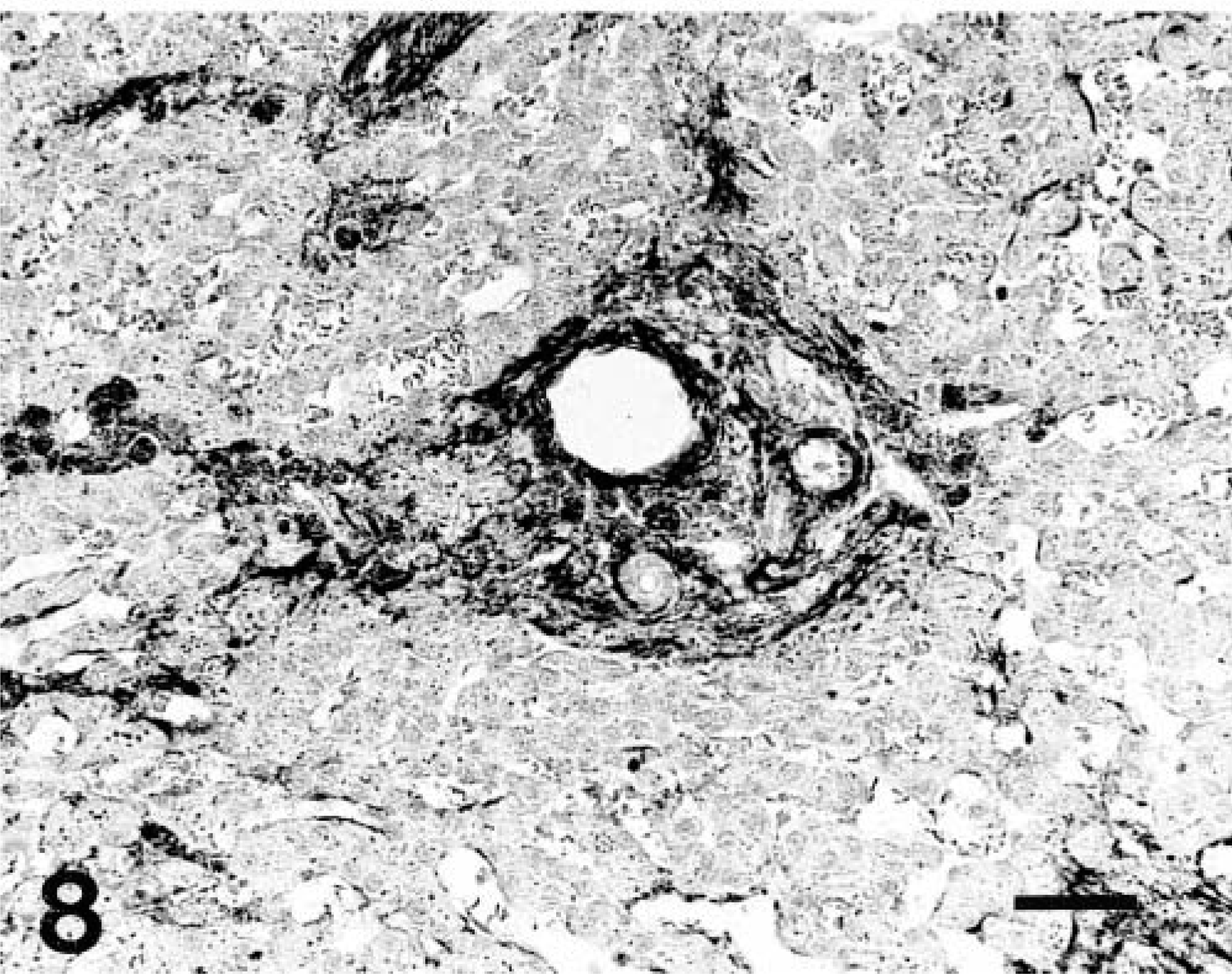
Liver; dog No. 11. Stage 2 fibrosis. Some sinusoidal α-smooth muscle actin–positive cells are observed in the enlarged portal areas and in fibrous septa. ABC method, α-smooth muscle actin antibody, Mayer's hematoxylin counterstain. Bar = 50 µm.
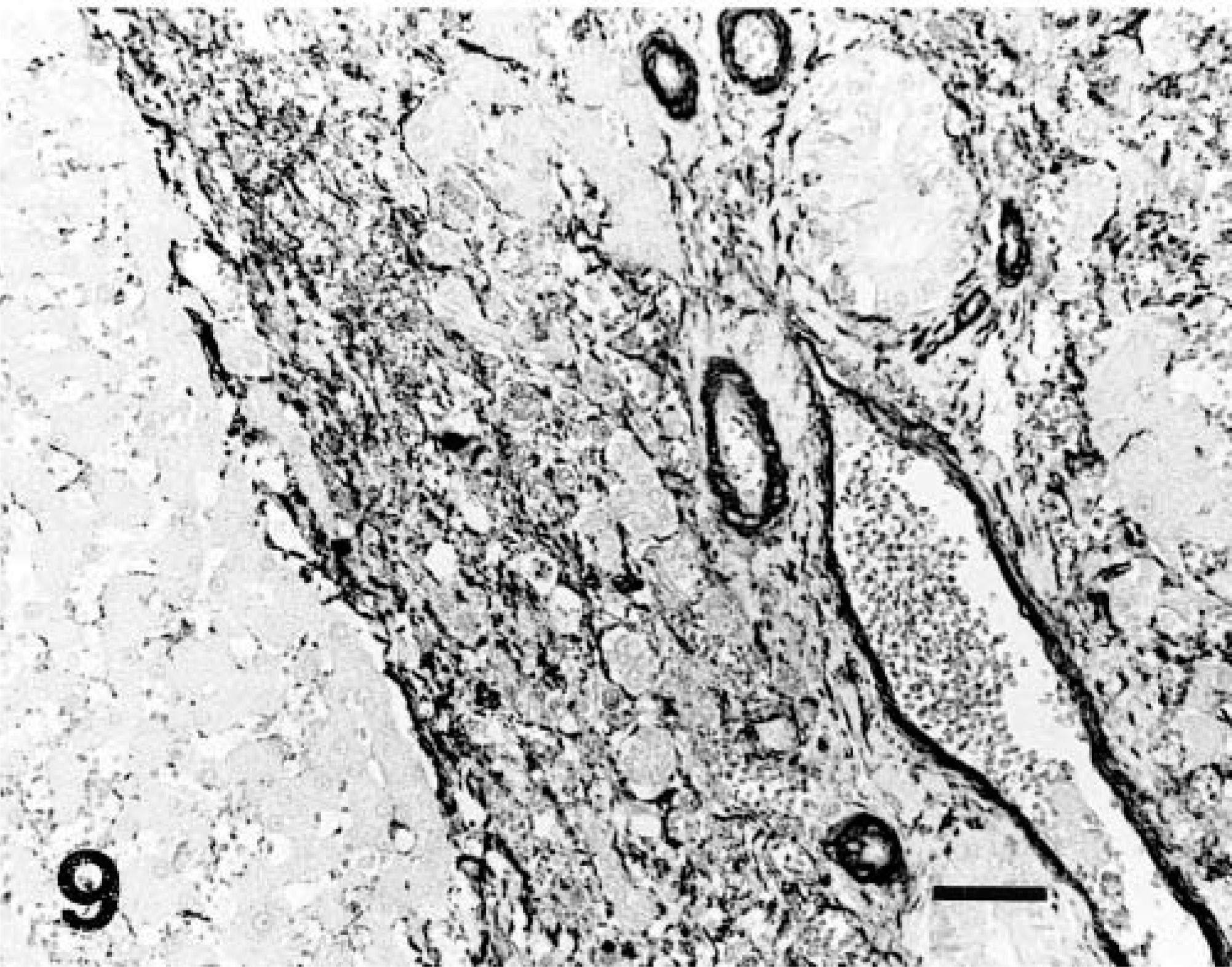
Liver; dog No. 18. Stage 3 fibrosis. Numerous α-smooth muscle actin–positive cells are observed in and around enlarged portal areas. ABC method, α-smooth muscle actin antibody, Mayer's hematoxylin counterstain. Bar = 50 µm.
Scoring and statistical analysis
All statistical results are summarized in Table 2.
Median values for various histologic and immunohistochemical variables in groups of dogs at different stages of chronic hepatitis development.
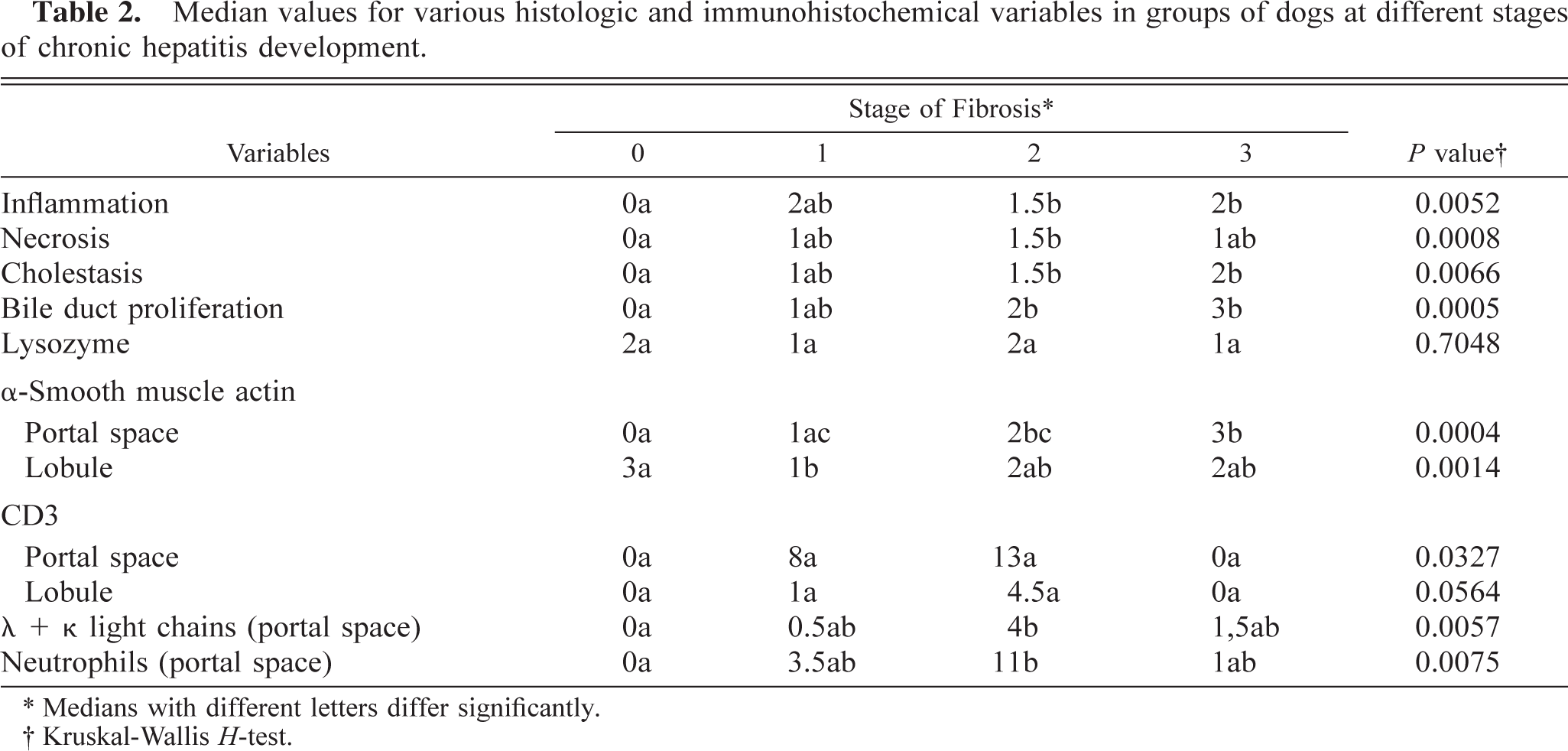
∗ Medians with different letters differ significantly.
† Kruskal-Wallis H-test.
Comparison of histologic changes among dogs in different stages of fibrosis
Inflammation status varied among stages of fibrosis (Table 2). Post hoc tests revealed that inflammation was increased in dogs with stages 2 and 3 compared with controls. Neutrophils were significantly more numerous in dogs with stage 2 fibrosis compared with controls.
Necrosis in dogs with stage 2 fibrosis was significantly increased compared with controls. Dogs in Stage 1 and 3 also tended to have more necrosis than did the control group. However, there was no significant difference in necrosis among dogs in the three stages of fibrosis.
Cholestasis and bile duct proliferation were increased significantly in dogs with stages 2 and 3 fibrosis compared with controls.
Comparison of immunohistochemical observations among dogs in different stages of fibrosis
Compared with controls and group 3 dogs, dogs with stage 2 fibrosis had higher numbers of CD3+ cells in triads and fibrous septa. According to the global test (Kruskal–Wallis test), there was a significant difference between groups, but the post hoc test (Wilcoxon Mann-Whitney U-test) did not confirm this difference. Dogs in stage 2 also tended to have more intralobular CD3+ cells, but the difference was not significant. The number of λ and κ light chain–positive cells in portal triads was higher in dogs with stage 2 fibrosis than in controls.
There was no difference among stages of fibrosis in regard to sinusoidal lysozyme and α-smooth muscle actin. However, the density of sinusoidal α-smooth muscle actin–positive cells was higher in controls than in dogs with stage 1 fibrosis. In contrast, α-smooth muscle actin–positive cells in portal triads were significantly more numerous in dogs with stage 3 fibrosis than in controls and dogs in stage 1 and were significantly more numerous in dogs with stage 2 fibrosis than in controls.
Association between inflammatory cells and histologic changes
According to the Spearman correlation test, the number of CD3+ cells in portal triads was positively correlated with the number of neutrophils and λ and κ light chain–positive cells (P < 0.001). The number of λ and κ light chain–positive cells was positively associated with the number of neutrophils (P < 0.001). There was also a significant positive association between necrosis scores and the number of portal and lobular CD3+ lymphocytes (P < 0.001), λ and κ light chain–positive cells (P < 0.001), and neutrophils (P < 0.001).
The density of α-smooth muscle actin–positive cells in portal triads was positively correlated with fibrosis (P < 0.005), inflammation (P < 0.001), necrosis (P < 0.001), and bile duct proliferation (P < 0.05). A positive association was noted between the portal α-smooth muscle actin scoring and the number of λ and κ light chain–positive cells (P < 0.001).
Discussion
Middle-aged purebred dogs were overrepresented in this study. Females predominated in the selected dog population, as has been the case in several previous reports of chronic hepatitis. 8,11,21,26,27
In the present study, livers were grouped according to the stage of fibrosis. Fibrosis is a well-known prognostic indicator in human chronic hepatitis. 29,31 It has also been recognized as a progression factor in Doberman Pinscher hepatitis. 25
Cholestasis and bile duct proliferation increased along with stage of fibrosis possibly because of the compression exerted on bile ducts in distorted fibrotic liver and/or a cytokine-induced proliferation of bile ducts. 24
The necroinflammatory activity tended to increase progressively in dogs with stages 1 and 2 fibrosis and then to subside in dogs with stage 3 fibrosis. This finding might indicate that the process is active in the subacute phase of canine hepatitis but wanes as the hepatitis progresses to a more chronic stage. Furthermore, according to the Spearman correlation test, necrosis was positively associated with the number of inflammatory cells (CD3+ cells, λ and κ light chain–positive cells and neutrophils).
In the lobules, CD3+ lymphocytes were more numerous in centrilobular areas, as noted in Doberman Pinscher hepatitis. 27 CD3+ lymphocytes closely apposed to degenerated hepatocytes were noted in eight dogs, all in stages 1 or 2 fibrosis and belonging to different breeds. A positive correlation between necrosis and the number of portal and lobular CD3+ lymphocytes was noted. These results further support the hypothesis of an immune-mediated response in some cases of canine chronic liver disease. 26,27 The λ and κ light chain–positive cell infiltrate was variable but generally mild. The positive correlation between the λ and κ light chain–positive cells and the portal α-smooth muscle actin is difficult to explain. In human hepatic fibrogenesis, B cells do not seem to be implicated in the process of activation and transformation of the myofibroblast-like cells. 14
The nature of the mononuclear infiltrate could not be determined immunohistochemically in dog No. 8; most mononuclear cells were CD3 and λ and κ light chain negative. Inadequate fixation might have deteriorated the epitopes recognized by the CD3 and λ and κ light chain antibodies. The presence of CD3- and λ and κ light chain–negative cells may also suggest the involvement of natural killer cells in few dogs with CCH, but this hypothesis would have to be confirmed by the use of specific antibodies for those cells.
Alpha smooth muscle actin is a marker for Ito cells and myofibroblasts. Ito cells in humans and rats increase in number and differentiate into myofibroblast-like cells, with marked expression of α-smooth muscle actin during hepatic fibrogenesis. 5,15,17,19,30 Myofibroblasts in normal human and rat livers are not confined to perisinusoidal spaces but can also be found around blood vessels and bile ducts. 17,19,32 Those periductular myofibroblasts seem important in hepatic fibrosis and liver remodeling. 17,32 When activated by various cytokines (e.g., transforming growth factor beta and platelet-derived growth factor), Ito cells and probably periductular myofibroblasts are qualitatively and quantitatively the most important producers of extracellular matrix proteins in human and rat chronic liver diseases. 5,14 Activated human Ito cells also produce an inhibitor of metalloproteinase (TIMP-1), decreasing interstitial collagenase activity and contributing to extracellular matrix accumulation. 5 As in human and rat chronic liver disease, α-smooth muscle actin–positive cells, corresponding probably to periductular myofibroblasts, tended to increase in portal and fibrotic areas along with the stage of fibrosis. The expression of sinusoidal α-smooth muscle actin (Ito cells) increased in lobular areas adjacent to fibrosis, principally around expanded portal spaces and fibrous septa as already noted for human chronic hepatitis. 30 Absence of positive cells in foci of nodular hyperplasia might be due to a lack of migration of Ito cells during hepatic regeneration. According to Spearman correlation tests, the density of α-smooth muscle actin–positive cells in portal triads was correlated with inflammation, bile duct proliferation, and fibrosis. These results suggest that inflammation in canine liver, as in human and rat liver, is associated with the activation of periductular myofibroblasts and possibly the proliferation of bile ducts. 5,14,24
In mouse and human liver disease, Kupffer cells are a source of tumor necrosis factor, and this cytokine is partly responsible for activation of myofibroblasts and T lymphocytes. 7,22 In the present study, there was no difference in number of intrasinusoidal lysozyme–positive cells among diseased livers and controls. The role of Kupffer cells in canine hepatitis needs further investigation.
Numerous dog breeds were affected with CCH, and middle aged females predominated. Necroinflammatory activity progressively increased and then waned as the hepatitis progressed to cirrhosis. The predominance of CD3+ lymphocytes and the presence of degenerated hepatocytes surrounded by those cells in many cases of active stage of chronic hepatitis was highly suggestive of an immune-mediated process. The exact phenotype of the CD3+ lymphocytes (CD4 or CD8) should be investigated. Periductular myofibroblasts seemed to play an important role in canine liver fibrogenesis.
Footnotes
Acknowledgements
We thank J. Deslandes, D. Naydan, J. Cardin, L. Pépin, and B. Pépin for technical assistance. Funding from Le fonds Du Centenaire supported this research.