
Abstract
A malignant pheochromocytoma with multiple metastases was diagnosed in a 7-year-old male wolfdog that resulted from a cross between an eastern timber wolf (Canis lupus lycaon) and an Alaskan malamute. A yellowish white neoplastic mass approximately 10 cm diameter was found in the right adrenal gland. The neoplasm penetrated through the wall of the caudal vena cava. A diagnosis of pheochromocytoma was established by histopathologic and immunohistochemical procedures. Immunohistochemically, the neoplastic cells expressed chromogranin A, substance P, synaptophysin, Leu-7, protein gene product 9.5, methionine- enkephalin, S100 protein, and galanin. Multiple metastatic tumors were found in the kidneys, spleen, lungs, heart, and liver.
Pheochromocytoma, an endocrine neoplasm derived from chromaffin cells, is the most common tumor in the adrenal medulla of animals. 2,4,5,17 Pheochromocytomas develop most often in cattle and dogs. 2,4,5 Functional pheochromocytoma has been reported infrequently in animals. 4,5,7 In human medicine, various neuropeptides in addition to epinephrine and norepinephrine have been demonstrated in normal adrenals and pheochromocytomas. 1,9,11,12,14 When metastases are present in nonchromaffin tissues, a pheochromocytoma in humans is considered to be a malignant neoplasm and is frequently nonfunctional. 6 There are only a few reports of malignant pheochromocytomas with multiple metastases have been noted in domestic animals. 2,4 Here, we describe the histopathologic and immunohistochemical characteristics of a pheochromocytoma with multiple metastases.
A 7-year-old male wolfdog that resulted from a cross between an eastern timber wolf (Canis lupus lycaon) and an Alaskan Malamute dog developed clinical signs of dysbasia. One month later, the wolfdog developed signs of hyperpnea, emaciation, and vomiting. The clinical course was progressive, and the animal eventually died.
Macroscopically, the right adrenal gland was enlarged by a 10-cm-diameter neoplastic mass that was yellowish white and had areas of hemorrhage and necrotic foci on the cut surface. The enlarged adrenal was adhered to adjacent organs, including the right kidney, liver, and caudal vena cava. The neoplasm penetrated through the wall of the caudal vena cava. A thrombus composed of neoplastic cells was present in the caudal vena cava, and the lumen of the vessel was greatly distended caudally. A small pheochromocytoma also was found the left adrenal gland. Multiple white nodular metastases 1–15 mm in diameter were observed in the kidneys, spleen, lungs, and liver. Chronic pulmonary congestion was evident, and in the heart there was right ventricular dilatation and tricuspid insufficiency.
Tissue samples from the main visceral organs and the adrenal neoplasm were fixed in 10% formalin, routinely processed, and embedded in paraffin. Histologic sections (4 µm) were prepared from paraffin-embedded tissues and stained with hematoxylin and eosin (HE), Giemsa stain, and the Grimelius method.
Histopathologically, the neoplastic cells of the right adrenal gland were arranged in lobules supported by a fine fibrovascular stroma (Fig. 1). The neoplastic cells had round hyperchromatic nuclei and granular eosinophilic to basophilic cytoplasm. The cytoplasmic granules were stained by the Grimelius method. Mitotic figures and giant cells were found frequently. Necrosis was also frequently observed in the center of the tumor. In the left adrenal gland, a small mass composed of neoplastic cells similar to those in the right adrenal gland was found. In the renal cortex, multiple metastatic neoplastic foci were found. Neoplastic cells frequently had giant nuclei and little cytoplasm, and the cells were arranged in irregular cords (Fig. 2). Neoplastic cells were also found in the glomeruli. Deposits of hyaline material were frequently observed in the mesangium of the lobules of glomerulus. The afferent arteriole showed occasional hyaline changes. In the spleen, metastatic neoplastic cells invaded the splenic artery and capsule. The central artery had a thick hyalinized wall and a much reduced lumen from the deposition of eosinophilic amorphous material beneath the endothelium and in the media. Multiple metastatic foci were also observed at the parenchyma of visceral organs such as the liver, lungs, and heart.
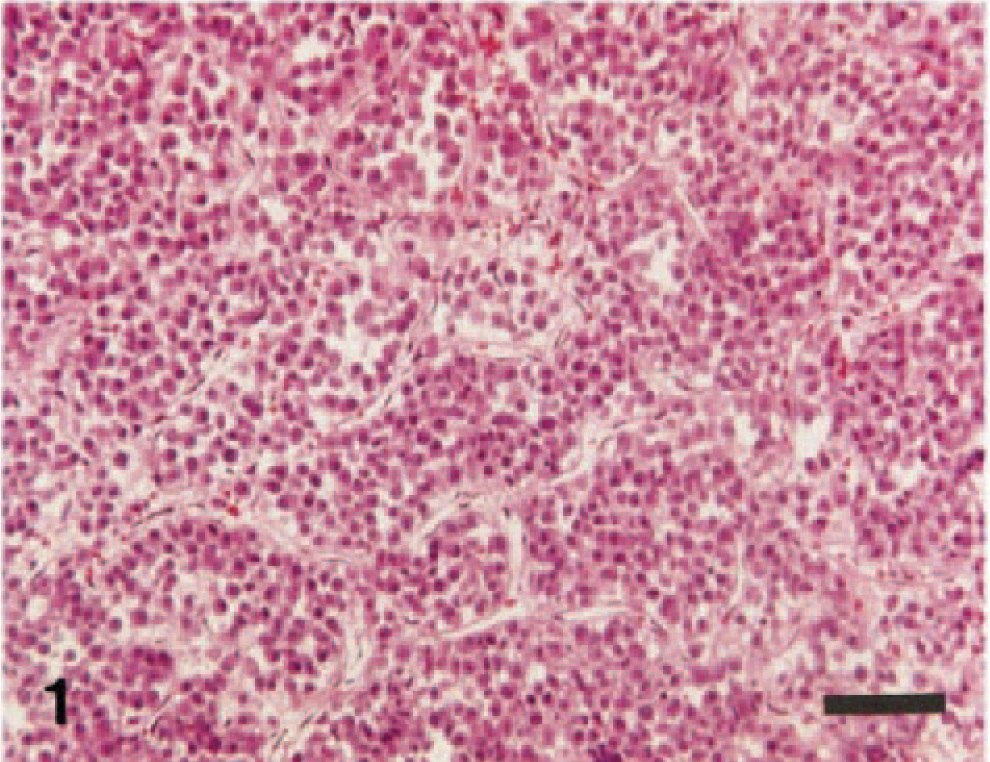
Adrenal gland pheochromocytoma; wolfdog. The neoplastic cells are arranged in small lobules supported by a fine fibrovascular stroma and have round nuclei and granular cytoplasm. HE. Bar = 60 µm.
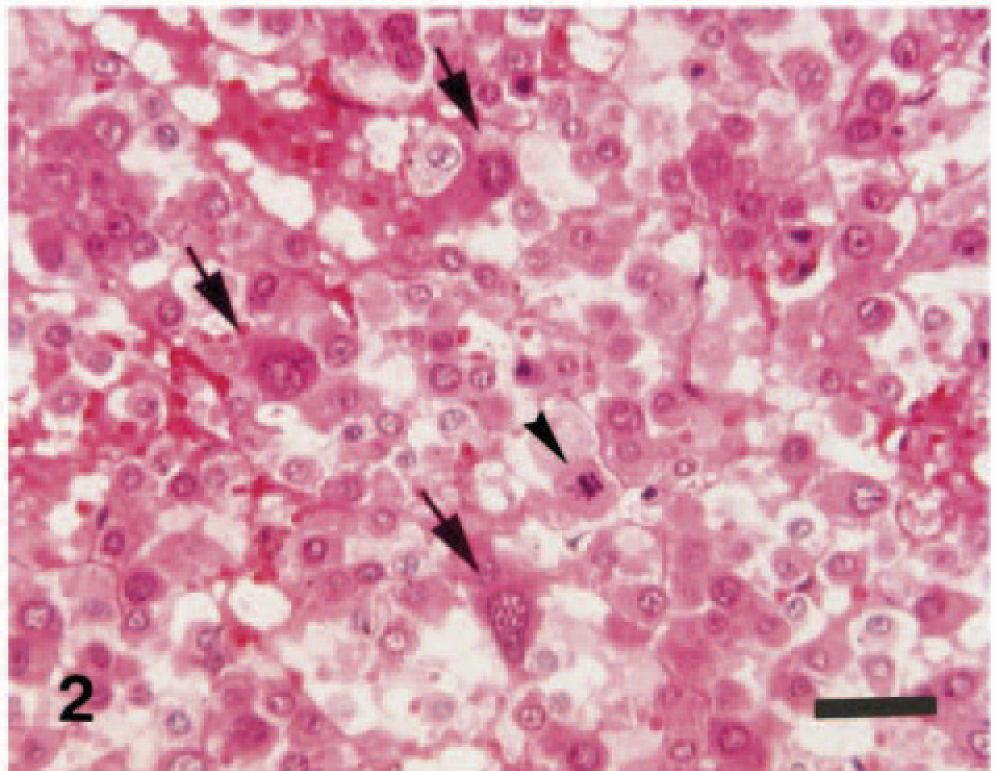
Kidney pheochromocytoma; wolfdog. Neoplastic cells in the metastatic foci are of various sizes and have mitotic figures (arrowhead) and large pleomorphic nuclei (arrows). HE. Bar = 30 µm.
Serial sections from the neoplasm were immunohistochemically examined by the avidin–biotin–peroxidase complex (ABC) procedure (Vectastain Elite ABC Kit; Vector Laboratories, Burlingame, CA). Details of the specific antisera used are summarized in Table 1. Deparaffinized sections were blocked for endogenous peroxidase in 3% H2O2 for 10 minutes. All sections were incubated with primary antibody at 4 C for 16 hours, with biothylated secondary antibody for 30 minutes at room temperature, and with avidin–peroxidase conjugate for 30 minutes. Staining was developed in 0.05% 3,3′-diaminobenzidine solution. For immunohistochemical control purposes, adrenal tissue from a normal dog was used. Control procedures included the use of excess antigen in relation to immune sera and nonimmune sera instead of the primary antibody; omission of the primary antibody resulted in the absence of specific reaction.
Immunohistochemical staining results for neoplasm in the adrenal gland of a wolfdog.
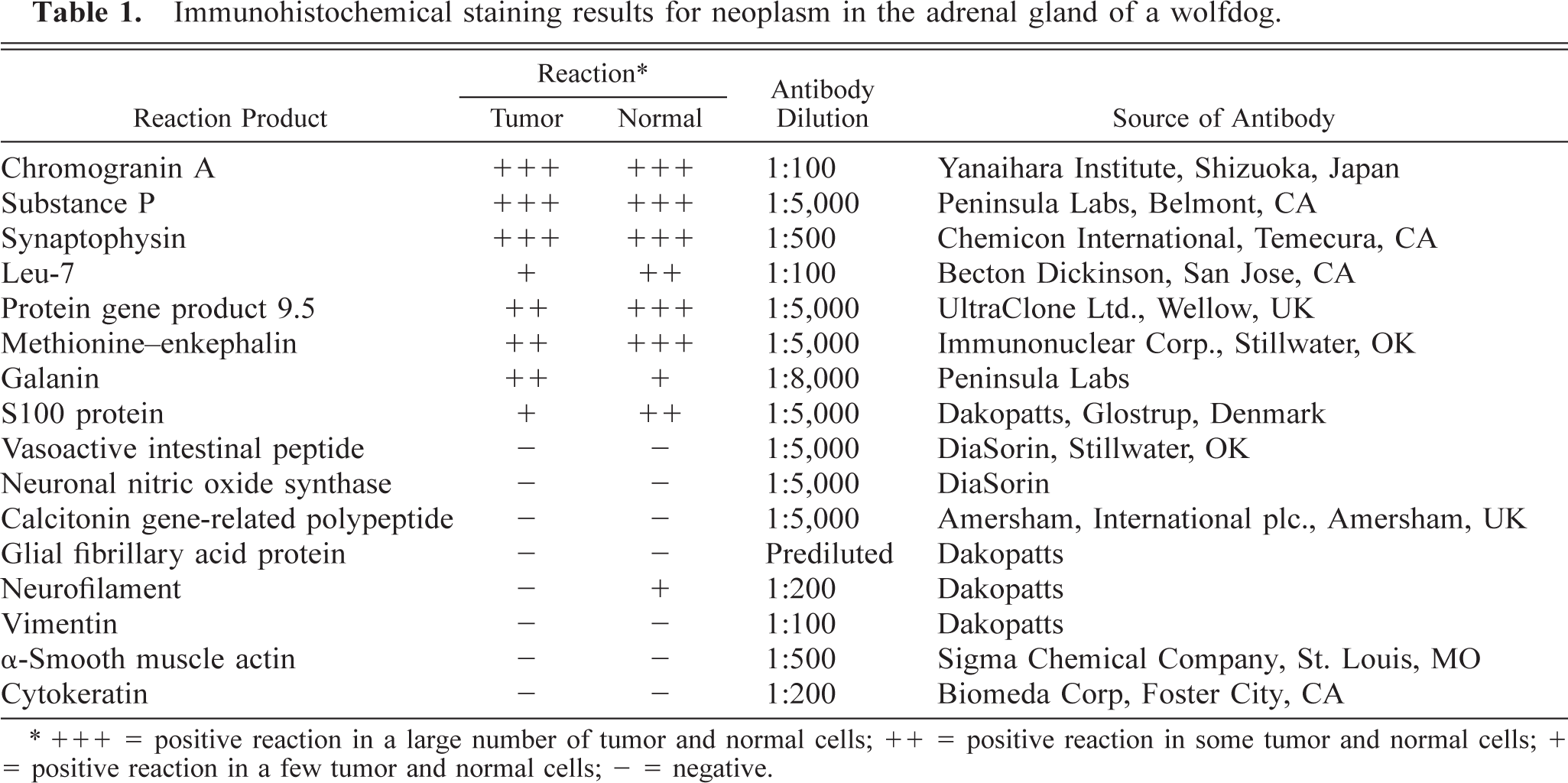
∗ +++ = positive reaction in a large number of tumor and normal cells; ++ = positive reaction in some tumor and normal cells; + = positive reaction in a few tumor and normal cells; - = negative.
A large number of the neoplastic cells in the primary neoplasm and the metastases were strongly positive for chromogranin A (CGA), synaptophysin (SYN) (Fig. 3), and substance P (SP). Some neoplastic cells reacted to protein gene product 9.5 (PGP 9.5) (Fig. 4) and methionine–enkephalin (ME) (Fig. 5), and galanin (GAL). A small number reacted to Leu-7 (Fig. 6) and S100 protein. However, the neoplastic cells were negative for vasoactive intestinal peptide (VIP), neuronal nitric oxide synthase (nNOS), calcitonin gene-related peptide (CGRP), glial fibrillary acid protein, neurofilament, vimentin, α-smooth muscle actin, and cytokeratin. The results of the immunohistochemical analysis are summarized in Table 1.
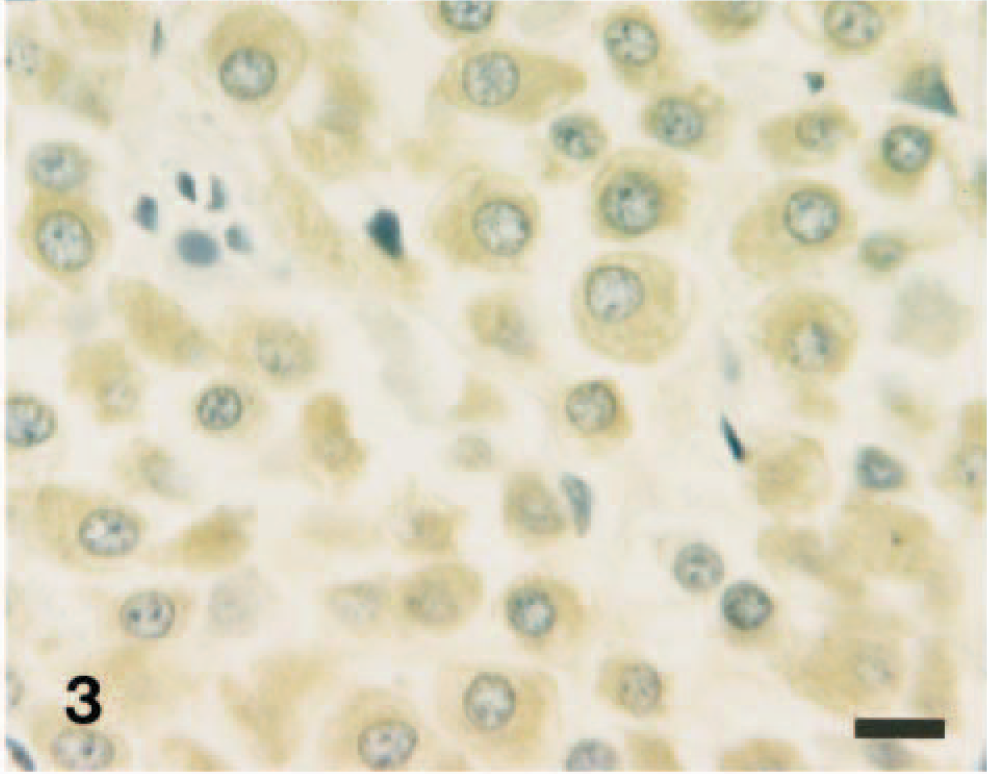
Adrenal gland pheochromocytoma; wolfdog. Most neoplastic cells react positively for the presence of synaptophysin. ABC method, Mayer's hematoxylin counterstain. HE. Bar = 10 µm.
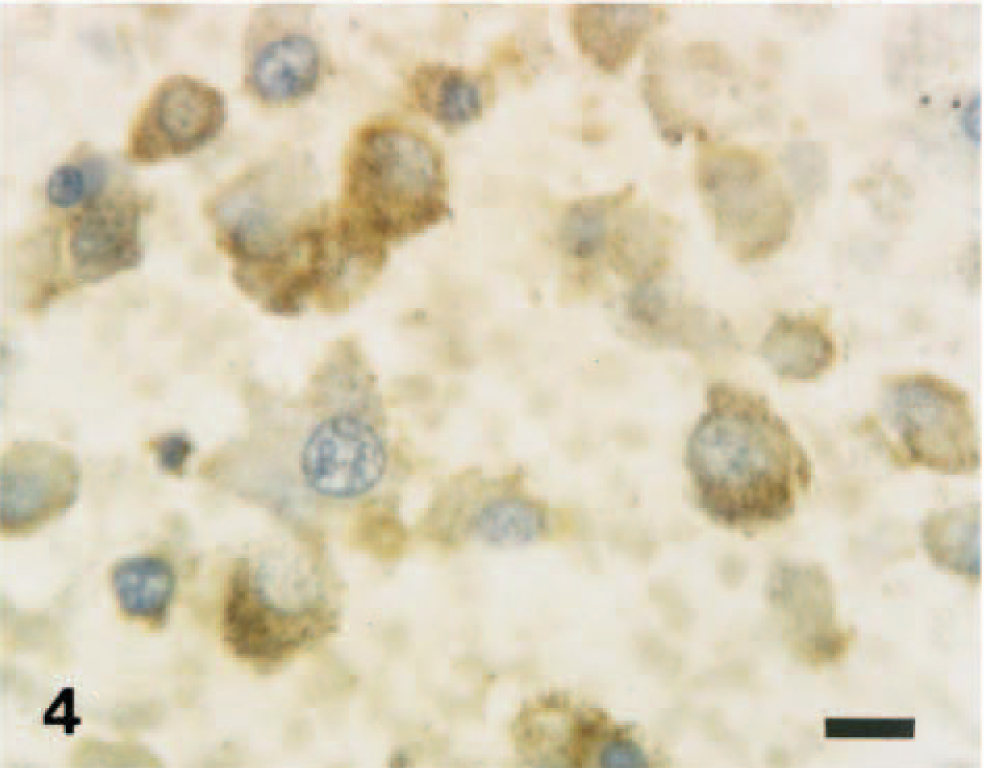
Adrenal gland pheochromocytoma; wolfdog. Neoplastic cells react positively to protein gene product 9.5. ABC method, Mayer's hematoxylin counterstain. HE. Bar = 10 µm.
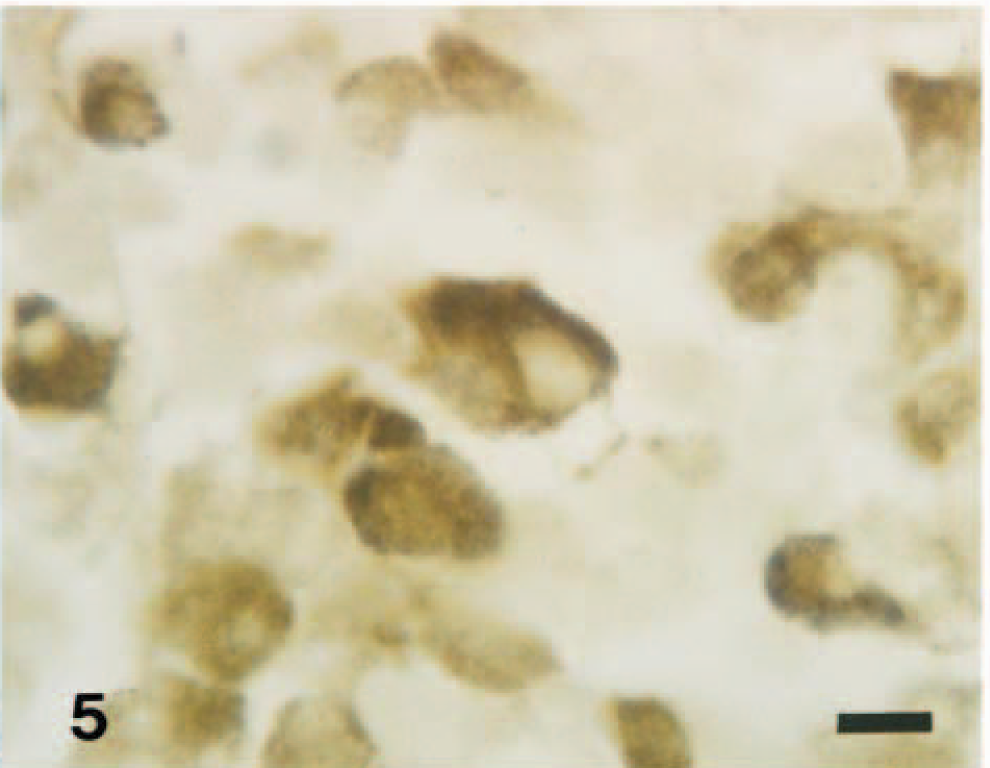
Adrenal gland pheochromocytoma; wolfdog. Neoplastic cells react positively to methionine–enkephalin. ABC method without counterstain. Bar = 10 µm.
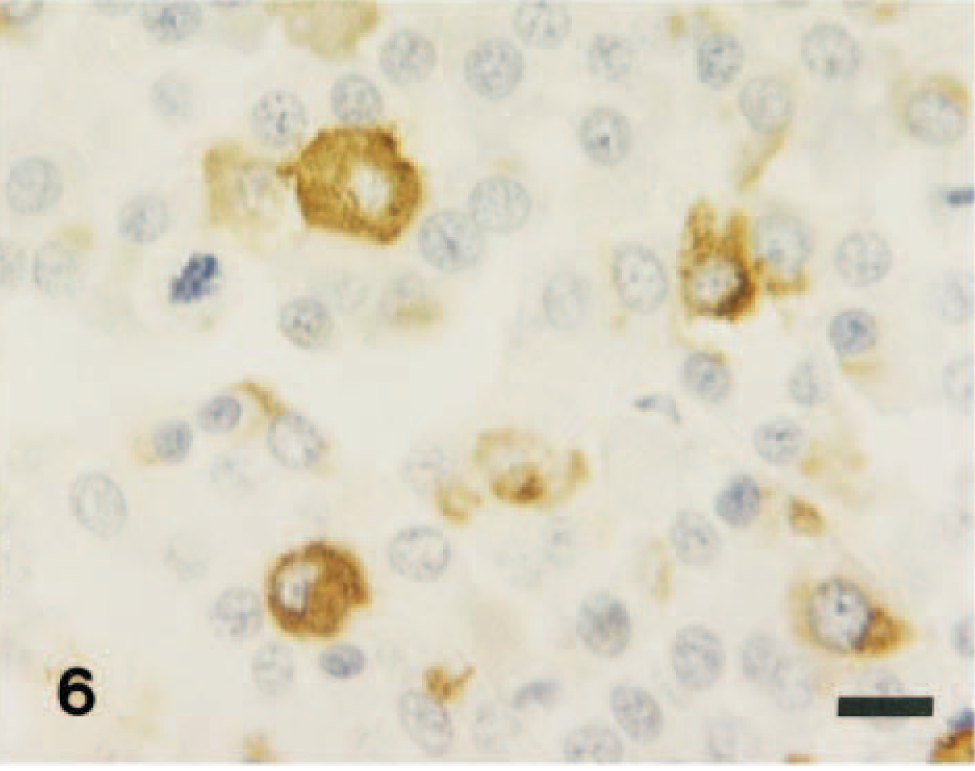
Adrenal gland pheochromocytoma; wolfdog. A few neoplastic cells react positively to Leu-7. ABC method, Mayer's hematoxylin counterstain. Bar = 10 µm.
In the present study, an adrenal neoplasm was diagnosed by histopathologic and immunohistochemical methods as a malignant pheochromocytoma with multiple metastases. Adrenal pheochromocytomas in dogs are usually benign neoplasms that have the potential for local invasion, but they are occasionally malignant with metastases to distant organs. 2,4,5
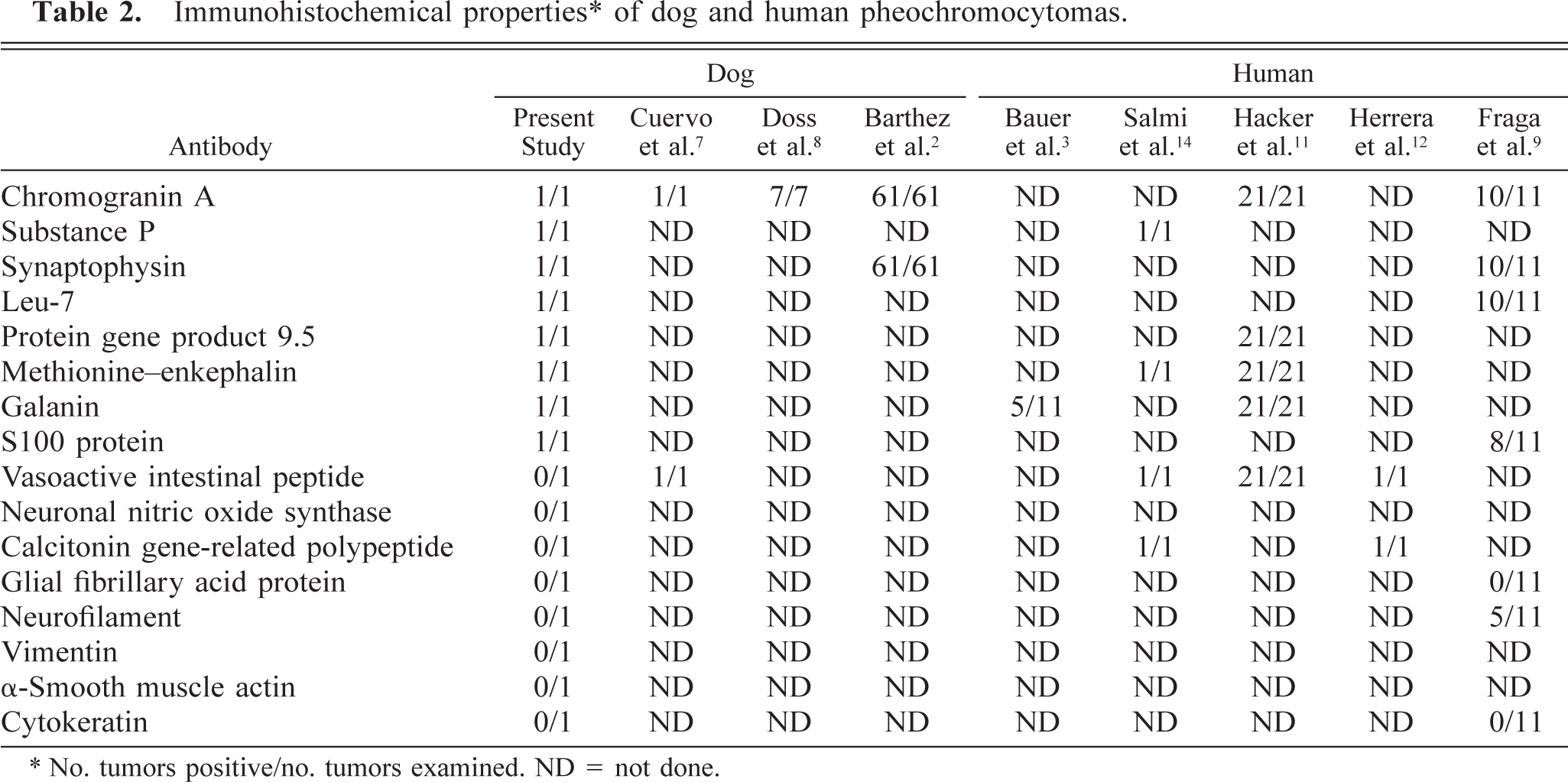
Immunohistochemical evaluation using antibodies against various neuropeptides is useful for confirming the chromaffin cell origin of neoplasms in humans and dogs. 2,7,9,11 CGA and SYN are usually detected in neoplastic cells of adrenal pheochromocytomas in dogs (Table 2). 2,7,8 In human medicine, the neoplastic cells react positively for CGA, SP, SYN, VIP, neuropeptide Y, ME, CGRP, calcitonin, PGP 9.5, Leu 7, S100 protein, and GAL (Table 2). 3,9,11,12,14 Further laboratory examinations have shown elevated levels of epinephrine, norepinephrine, somatostatin, pancreatic polypeptide, calcitonin, SP, ME, nNOS, CGRP, GAL, PGP 9.5, and VIP in the plasma of patients with adrenal pheochromocytomas. 1,11–13,15,16 These results suggest the production of catecholamines and various neuropeptides by the neoplastic cells. In the present study, the immunohistochemistry results suggested that, like human pheochromocytomas, the neoplastic cells may contain various neuropeptides such as CGA, SP, SYN, Leu-7, PGP 9.5, ME, S100 protein, and GAL. However, the presence of VIP and CGRP was not demonstrated in these neoplastic cells.
Immunohistochemical properties ∗ of dog and human pheochromocytomas.
∗ No. tumors positive/no. tumors examined. ND = not done.
Pheochromocytomas may occasionally be associated with clinical signs as a result of the continuous or episodic secretion of one or more of the catecholamines: epinephrine, norepinephrine, or dopamine. 5,6,11,12 Elevations of blood pressure induced by the sudden release of catecholamines can precipitate acute congestive heart failure, pulmonary edema, myocardial infarction, ventricular fibrillation, and cerebral hemorrhage. 5,6 Arteriolar sclerosis and medial hyperplasia of arterioles are histopathologically observed in dogs with pheochromocytomas. 5 No hormonal measurements were performed in this wolfdog; however, the glomerulosclerosis and splenic arteriosclerosis suggest possible hypertension due to episodic catecholamine secretion by the tumor. 10