
Abstract
Abstract
Purpose
Telescopic intramedullary nailing (TN) has become the main choice of treatment in children with osteogenesis imperfecta (OI). The classical parapatellar tibial nailing technique poses difficulties in maintaining reduction, insertion of the nail and fluoroscopic imaging. Also, deformities of the proximal tibia in relatively small children with OI can be problematic for tibial nailing. In this report, we present the retro-patellar approach in tibial TN of children with OI as an alternative to the classical approach and report the early radiographic and clinical results of our patients.
Methods
The nail is inserted through a skin incision proximal to the patella, passing inside the patellofemoral joint while the knee is positioned to 15° to 20° of flexion. In total, 30 tibiae of 15 patients had been operated and were reviewed after at least one year of follow-up. Any complications, such as implant failure, joint damage or instability, malunion, nonunion or refracture, were recorded.
Results
The mean age of our patients was 8.5 years, and the mean follow-up period was 27 months. There were no complaints involving the knee. All patients showed complete union without any implant failure or refracture. We did not observe any nail protrusion, bending or loss of correction during the procedure.
Conclusion
The retro-patellar approach for tibial TN appears to be safe and effective in patients with OI.
Level of Evidence
IV
Introduction
Osteogenesis imperfecta (OI) is a group of inherited connective tissue disorders in collagen structure, processing or cross-linking, new bone formation and osteoblast differentiation, which result in fragility of the bones, recurrent fractures and deformities. 1 Telescopic nails/nailing (TN) have been the preferred implant in the treatment of fractures and correction of deformities of long bones in children with OI, who have more than two years of growth remaining.2–6
TNs are traditionally inserted into the tibia through a patellar tendon splitting or para-patellar approach, similar to traditional tibial nailing.3,5,7 After previous articles about adult tibia fractures had reported difficulties with the para-patellar approach in nail alignment, fracture positioning and fluoroscopic imaging, the latest articles have popularized the retro-patellar approach in tibial nailing as an easy and safe method.7–11 There are also other difficulties encountered during TN of the tibia in children with OI. These are mostly deformities of the proximal tibia, very little space between the patella and the tibia due to patella baja or small size of the patient, and absence of a proximal slope in a TN contrary to rigid tibial nails. There is also a risk of deformity of the proximal tibia due to physeal injury with the anterior insertion of the nail through a parapatellar approach. 12
The aim of this article was to present the retro-patellar approach in TN of the tibia in children with OI and to report our early results.
Patients and methods
After receiving institutional review board approval, we reviewed the files of children with OI who had undergone TN of the tibia through a retro-patellar approach between 1st January 2014 and 31st December 2018. The indications for tibial TN were deformity > 20° and any fragility fracture of the tibia. Patients with at least one year of follow-up and at least two years of growth remaining were included in the study. Children with a history of surgery to the operated tibia were excluded from the study. In addition to the demographic data of the patients, the author team reviewed the files of each patient for the type of OI, medical therapy history, indication for TN and preoperative and follow-up activity levels, tibial refractures or nailing history of other bones, and any history of swelling, pain, locking sensation, limited movement or increased instability of the knee joint. The radiographs were reviewed by the leading author (O.A.E) and the senior author (M.I) for the position of the nail on the proximal tibial surface, tibial slope, union or nonunion, deformity of the bone or the nail and retrograde telescoping, which is a retrograde displacement of the tip of the obturator part, and for negative telescoping which is retrograde migration of the proximal tip of the sleeve part. Each patient was invited to our clinic for a final clinical review. Each patient was examined again with a primary focus on symptoms and signs of any injury to the knee joint.
Surgical technique
With the patient supine, a folded towel is placed under the knee to facilitate 15° to 20° of knee flexion. Tourniquets are avoided to prevent iatrogenic femoral fractures. After realignment of the fragments after required osteotomies, TN begins. For a retro-patellar approach to insert the TN, a 2-cm to 3-cm longitudinal skin incision is made in the midline just proximal to the superior pole of the patella (Fig. 1). The quadriceps tendon becomes visible after soft-tissue dissection. It is incised longitudinally to reach and pass the joint capsule. Then, a soft-tissue protector sleeve, which is included in the set, is applied through the wound distally. The trochlear groove is used as a guide for positioning the sleeve. When it is positioned, it should touch anterior to the middle of the proximal tibial surface.
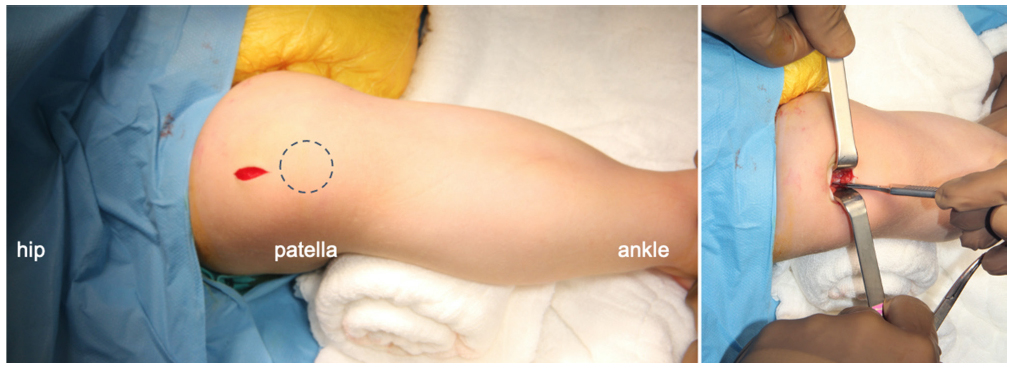
The pictures show the skin incision and incision of the quadriceps tendon, with the knee flexed 15° to 20° with a bump under it.
We used the TN with a corkscrew tip and D-profile in our patients, and the following description of the retro-patellar technique also mentions unique surgical principles of that TN. A 1.5-mm drill guide is advanced through the protector, and it is passed through the tibial articular surface just at the anterior part of the middle third of the slope, so it centralizes the tibial medullary canal. The position of the guidewire is confirmed by anteroposterior (AP) and lateral fluoroscopic views (Fig. 2). The AP view is obtained by tilting the fluoroscopy about 15° on the sagittal plane. The lateral view is obtained by externally rotating the ipsilateral hip and keeping the knee flexed to 15° to 20°. Tilting the image intensifier on the transverse plane of the patient might be needed if hip external rotation is limited. After confirming that the guide is centralized towards the centre of the medullary canal on both views, it is advanced down until the osteotomy or the fracture site. Then, a proper reduction is performed, and the guidewire is advanced until the distal metaphysis. A suitable reamer, which is 0.5 mm thicker than the thickness of the obturator or female component, is applied over the wire, and the medullar canal is carefully prepared. It should be noted that it is sometimes difficult to pass the old fracture sites with the reamer, and utmost care should be practiced against inadvertent fracture of the bone or bending of the wire. Reaming can also be performed from the osteotomy site, retrogradely for the proximal segment, depending on the preference or condition of the diaphysis, especially when it is very thin or sclerotic.
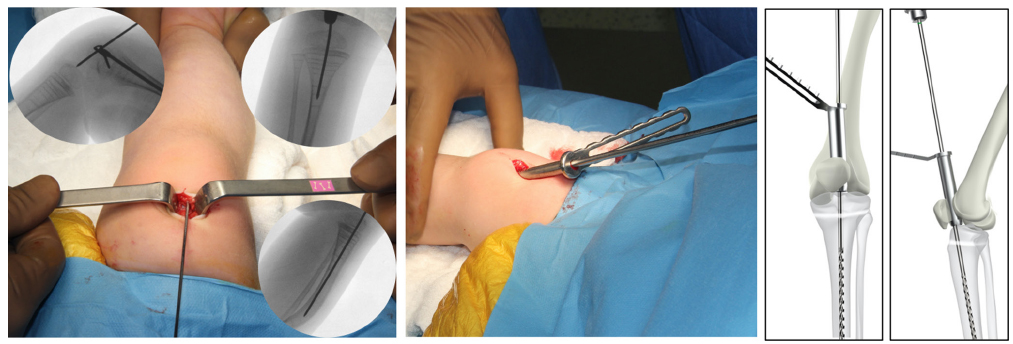
Intraoperative pictures and fluoroscopic views during guidewire placement and reaming are presented. When the position of the wire is confirmed under C-arm, the soft-tissue protector is positioned over the trochlear groove and reaming begins through it.
When the reaming is finished, first, the obturator or the male component of the TN is inserted through the retro-patellar space, inside the protector sleeve. It is cut to the most appropriate size after it passed the osteotomy site, depending on the distance between the tip of the obturator and the epiphysis. Then, different sizes of the sleeve or the female component are tried on the leg under the fluoroscopy. The soft-tissue protector is removed and the best fitting size of the female component is advanced over the obturator, and both components are pushed until the metaphysis. When the tip of the obturator component is near the physis, the system is turned clockwise until the corkscrew tip passes it and touches the subchondral bone, while the proximal threads of the sleeve component are fixed inside the proximal tibial epiphysis (Fig. 3). The knee is fully extended, the rotational alignment is controlled clinically and corrected if needed, and irrigation of the knee joint through the proximal wound is done to clear debris left after reaming. Finally, the distal interlocking of the tip into the epiphysis is performed under fluoroscopic control from the medial side of the distal tibia with 1.8-mm threaded wires passing between the threads of the corkscrew construct (Fig. 4). A long leg splint or a prefabricated ankle-foot orthosis (AFO) is applied if needed.
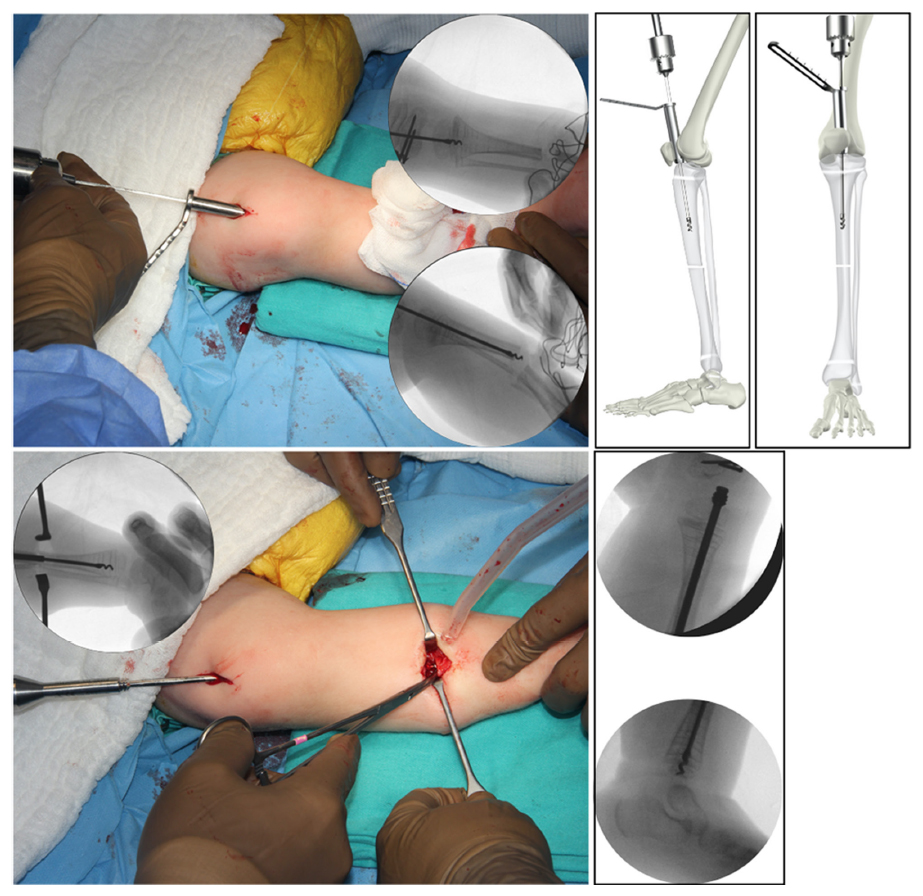
The steps of retro-patellar insertion of the telescopic nail after proper reaming and osteotomy are shown.

The distal interlocking and the final position of the wires are shown in the pictures.
When the postoperative pain improves, early range of movement exercises begin. At the end of the tenth day, the splint is changed to an AFO. When a bridging callus is observed at three cortices on radiographs, weight-bearing with the AFO is initiated. Criteria for a complete union during follow-up are callus formation at four cortices and/or absence of pathological movement at the osteotomy site and painless weight-bearing (Fig. 5). When this is achieved, AFO is removed, and free weight-bearing is allowed.

Preoperative, early postoperative and one-year follow-up radiographs of a patient are shown in order from left to right.
Collected data were presented through descriptive statistics using central tendency for continuous variables as mean and sd and dispersion as ranges.
Results
The clinical records of 24 patients who had undergone TN of the tibia using a retro-patellar approach between 2014 and 2018 were reviewed. In total, 15 patients with a complete follow-up of more than one year were included in the study. All cases were operated bilaterally in the same session (30 tibiae). The patient demographics are given in Table 1. Three tibiae were operated for a fragility fracture, and 27 were operated for a deformity. All of the deformities were located at the diaphysis and proximal or distal meta-diaphyseal junction. Most of the deformities (21) were multiplanar, located on both sagittal and frontal planes, some required two-level osteotomies (Table 2). All patients were operated using either a 3.5- or 4-mm TN (D-scope; TST Medical, Istanbul, Turkey), in nine cases and six cases, respectively. All patients reported transient knee discomfort for the first nine to ten days after the operation. Only one patient experienced knee pain for three weeks, which caused him to begin rehabilitation two weeks later.
Patient demographics
Clinical patient data
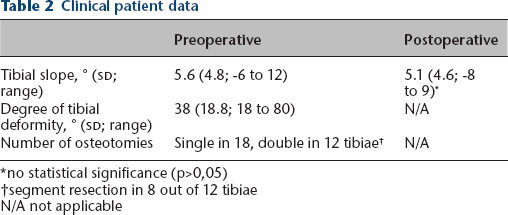
no statistical significance (p>0,05)
segment resection in 8 out of 12 tibiae
N/A not applicable
Weight-bearing began at an mean of 6.8 weeks (sd 1.2; 6 to 10). Each patient was under intravenous (I.V) pamidronate treatment before the operation. It was resumed when each patient was allowed to bear weight. The mean time of complete union was 10.5 weeks (sd 0.8; 10 to 12). The mean time for complete union of fractures was 10.3 weeks (10 to 11), while it was 11.2 weeks (10 to 12) for deformities. Every patient came for the last visit, and a detailed examination was performed, including a thorough knee examination. Any condition that might be caused by the retro-patellar approach was recorded, such as pain, instability, locking and limited movement at the knee. We did not detect any scar hypertrophy or any other condition at the incision or nail entry site, any patellar instability or pain at the patellofemoral joint or stiffness, increased instability or pain at the tibiofemoral joint in any patient. One patient complained about ankle irritation due to a protruding interlocking wire. The wire was shortened in the third postoperative month. One patient experienced a delayed union. He was allowed to bear weight by 17 weeks when the callus formation was completed.
Ten patients underwent concomitant TN for either femur (six cases) or humerus (four cases). One patient underwent a revision surgery through the suprapatellar incision after two years of follow-up due to a fall from high and angulation of the tibia to 10° together with the nail inside. Two other patients were operated for revision TN after getting taller during three years of follow-up. All were revised with the retro-patellar approach without compromise. None of the other patients were operated again for a tibial or any other long bone fracture or deformity during the follow-up.
Two of the patients who had been non-ambulatory became ambulatory with variable support after tibial nailing. Two patients showed progression from ambulatory with support to ambulatory with less support. Out of four patients who were able to stand with support, two cases became ambulatory with support. Other patients (seven cases) remained ambulatory with support during follow-up after tibial TN.
Discussion
The study aimed to introduce the retro-patellar approach as another method of TN in children with OI. Our results showed that the technique was safe and effective.
TNs have long been the preferred implants in the treatment of deformities or fractures in children with OI.13,14 There have been many types of TN that share a common structure, such as an obturator and a sleeve whose ends are fixed to both physes of a long bone.2,4,6,15 We have been using a TN with a corkscrew tip (D-scope) for the last six years and have recently published the results of our patients. 16 All patients, except one case, showed complete union and a successful telescoping effect.
Tibial nailing using a parapatellar approach through or beside the patellar tendon is accepted as the standard method for both rigid tibial nailing and TN.3,5,16–18 However, this technique has some drawbacks, such as difficulties with maintaining fracture or osteotomy alignment, obtaining an optimal trajectory of the nail and fluoroscopic imaging during the operation.9–11,19 Recent articles7,9–11 reported that these risks were eliminated with a retro-patellar or suprapatellar approach, and the authors recommended it in the treatment of adult tibial fractures with tibial nails. The risk of an increase in deformity secondary to excessive knee flexion for the nail entry with the classical approach was mentioned in the article by Eastman et al. 9 These authors concluded that retro-patellar nailing with a semi-extended position of the knee (especially 15° to 20° of flexion) facilitated nail entry, reduction maintenance and fluoroscopic imaging. Garnavos 10 defined the surgical technique for complex tibial plateau fractures and reported the results of the pilot study. The author mentioned the common problems of classical tibial nailing, which were difficulty with intraoperative imaging, maintaining fracture reduction, and the need for leg support during the procedure. The author concluded that these problems were solved with the retro-patellar technique. Jones et al 11 published the results of their two groups of adult patients treated with either retro-patellar or infrapatellar tibial nailing. These authors reported that the accuracy of reduction and nail insertion were significantly better with the retro-patellar approach, without any increase in the operation time, fluoroscopy requirement, or articular injury.
After the introduction of the retro-patellar approach for tibial nailing, its safety was questioned and cadaveric studies were conducted.8,20 In their study on adult cadavers, Bible et al 8 reported that the retro-patellar technique was a safe alternative with no meniscal or cruciate ligament injury – as in the parapatellar approach – and less inter-meniscal ligament injury. In their cadaveric study, Eastman et al 20 reported that the injury risks to the inter-meniscal ligament and the medial meniscus, which are comparable with the classical approach, could be prevented by avoiding excessive medial entry. The patellofemoral joint remained intact with the technique. A smaller portal for entry of a thin TN in OI might also decrease the risk of intraarticular damage, as expected. On the other hand, the function of the inter-meniscal ligament is still debated and its injury was not shown to affect the anatomic integrity of the joint.20,21 Some other studies included pre-nail and post-nail arthroscopies of adult patients treated with tibial nailing. 19 The authors of these studies report some chondromalacia in the patellofemoral surfaces but these findings neither correlated with clinical nor MRI findings. In our cohort, we did not detect any complication related to an injury to the patellofemoral or intraarticular structures of the knee.
To our knowledge, this is the first paper on the retro-patellar technique for tibial nailing in children. In addition to the abovementioned difficulties with classical tibial nailing, the relatively small size of an OI patient and patella alta or possible other deformities of the tibia may result in a smaller orifice for the nail insertion, which might hinder nailing. Difficulty with nail alignment may also cause bending and loss of telescoping feature of a TN, considering that these nails are composed of two straight components, obturator/male and sleeve/female, as the major part of their elongating feature. Because of the inability to give a proximal bend to the TN (contrary to rigid tibial nails), its insertion through a parapatellar approach might cause difficulty. With the retro-patellar approach, we did not experience any difficulty in TNs, such as tibial malalignment or nail bending during or early after the operation. In adult cases, the operation equipment may include a longer soft-tissue protector sleeve for a longer path inside the body. In paediatric cases, however, there was not any need for equipment revision because of the small size of OI patients in our study.
Possible complications after anterior tibial physeal damage in children have concerned physicians. Tibial slope changes or recurvatum deformity due to anterior physeal damage after intramedullary nailing of the tibia in skeletally immature children was reported by Cruz et al 12 and it is currently avoided in immature children. 17 On the other hand, Court-Brown et al 18 reviewed their paediatric cases of intramedullary nailing of tibial fractures. Although they did not observe any malalignment or growth disturbance, their cohort consisted of adolescent patients who had only limited growth potential left. Considering the very young age at the time of operations for OI, concerns about growth disturbances cannot be eliminated based on available evidence. With the retro-patellar approach, the nail can be inserted just at the junction of the anterior and middle thirds of the tibial slope, which coincides with the centre of the tibial medullary canal. Because this point is more central than the classical approach, it might eliminate tibial slope changes in the follow-up. Likewise, we did not detect any change in tibial slope with the new approach during our follow-up.
Because of its retrospective design and the recent introduction of the technique, this study has some limitations. The follow-up period of our cohort is short, considering the young age of the patients and possible future complications related to the OI disease. However, early postoperative results after a mean of 27 months were considered sufficient to present the surgical technique. The number of cases might be higher. After verifying the effectiveness and safety of the exposure, the number of cases was considered adequate to introduce the technique to paediatric orthopaedic care. However, we did not perform any postoperative knee MRI or a knee arthroscopy to control the knee joint for any possible subclinical damage to the articular structures, which might be a limitation of our study. Lack of a comparison group operated on with the standard approach was another limitation. A comparative study with longer follow-up would certainly give more convincing results. We utilized the technique with one type of TN, which increases the homogeneity of our cases but cannot claim results for other types. Because the main shared property of a TN is its composition from two pieces gliding on each other, other nail types are expected to give similar results with the retro-patellar technique. Another possible limitation of this technique is the fact that we revised only three TN after a retro-patellar approach before submission of this paper, which will be required for other patients in a couple of years due to continuing growth. We managed to replace them through the suprapatellar approach easily. However, Garnavos 10 reported one case of tibial nail removal from an adult case, which required a transpatellar approach. In children with OI, revision through the retro-patellar approach would not be difficult by using fluoroscopy and with the knowledge of the thickness of the nail preoperatively to prepare fitting equipment. Another limitation of the study is the fact that we were unable to perform a comparison between classical and retro-patellar techniques for the development of recurvatum deformity during follow-up, although none of our patients experienced such a deformity. Additionally, tibial slope measurements are usually nonideal in this patient group because of complex deformities of the tibia. For the follow-up, an independent physician measured tibial slopes using the same technique, which might increase the value of tibial slope measurements of our cohort.
In conclusion, our report shows that the retro-patellar approach for tibial TN in patients with OI is safe and effective especially in aligning the nail to the neutral or corrected tibial axis and avoiding anterior physeal injury, while preserving articular structures.
Footnotes
BG: Data analysis and interpretation, Drafting, Critical revision, Manuscript production.
IS: Data analysis and interpretation, Drafting, Critical revision, Manuscript production, Analysis
MI: Senior author, Design, Data analysis, Drafting, Critical revision, Manuscript production, Guidance.