
Abstract
Purpose
To introduce a new model of telescopic intramedullary rod (TIR), evaluate its effects on treating patients presenting with moderate and severe osteogenesis imperfecta (OI) and to compare the findings with those of other telescopic rods.
Methods
A total of 21 patients (nine girls and 12 boys; mean age at first operation, 6.6 years, 1.52 to 13.18) who underwent 52 femoral operations were monitored during a mean of 9.96 years (3.39 to 14.54). Patient characteristics, telescoping rod capability and its complications were examined.
Results
According to the Sillence classification, we investigated one patient with type I, nine with type III and 11 with type IV OI. Revision rates at up to five years (36%) were inferior to those found for the Fassier-Duval rod (46%). The main cause of revision was fracture (15 patients), followed by rod migration (nine), and infection (two). The rod exhibited higher telescopic capacity in boys than girls. Type III most commonly required an operation; the age group with the highest number of procedures was five to ten years. Male migration was the main cause of rod migration.
Conclusion
The TIR has a satisfactory cost-benefit ratio with less complication rates and low production costs. The TIR is a feasible alternative to the commonly used Fassier-Duval rod.
Level of Evidence
IV
Introduction
Osteogenesis imperfecta (OI) is the clinical manifestation of a genetic disorder that, in most cases, modifies the production of type I collagen. Patients present with critical structural skeletal modifications that progress to recurrent fractures and/or expressive deformities of long bones and the axial skeleton. Medical treatment includes the use of bisphosphonates, which improve bone density and decrease the risk of fracture. However, fracture deformities often require surgical correction and intramedullary rods are the most commonly indicated treatment.
The first intramedullary rod technique developed to treat patients with OI was created by Sofield and Millar 1 . The technique corrects long bone deformities through multiple osteotomies, sub-dividing the bone into several fragments and subsequently fixing it by inserting a fixed-size rigid rod. The main limitation of this technique is that the rod cannot follow bone development, thus, affected children require several re-interventions throughout their development2–6. To circumvent this issue, Baley and Dubow created a two-component rod that enabled telescopic modification3,7–11. Since then, various rods (fixed/telescopic) have been developed; the Fassier-Duval (FD) rod is currently the most used worldwide2,12–15. Following the principles established by Sofield and Millar and Baley and Dubow, a telescopic intramedullary rod (TIR) specifically designed for treating fractures and deformities in patients with OI was developed at the Santa Casa de São Paulo Hospital in 2000. Our TIR, similar to other telescopic rods, is designed to follow bone growth; it is applicable in younger children with narrower and more cannulated medullary canals.
Objectives
We aimed to evaluate the effects of treatment with TIRs in patients with moderate and severe OI and compare the findings obtained with the results of other telescopic rods reported in the literature.
Patients and methods
Between 2000 and 2015, the orthopaedic service of the Santa Casa of São Paulo Hospital used TIRs in the femurs of 21 patients (nine girls and 12 boys) with a mean age of 6.6 years (1.52 to 13.18). According to the Sillence classification 16 , we observed one patient with type I OI, nine with type III and 11 with type IV OI. Since this study aimed to evaluate moderate and severe forms of OI, the patient with type I was excluded from the comparative analysis.
These patients received 52 femoral TIRs, 28 for the right limb and 24 for the left limb.
Clinical and radiographic records were evaluated in all patients. Further, data were discarded from the study whenever a patient required replacement of synthesis material by another synthesis or rod type. As a follow-up parameter, the initial time was defined as when the patient underwent the first operation for TIR implantation, and the completion time was when the patient underwent TIR removal or when the study was completed.
Characteristics of the TIR and surgical technique
The TIR technique was pioneered by the senior paediatric orthopaedist Dr. Claudio Santili. The rod was comprised of two pieces that could be attached and slid along each other, enabling it to be telescopic and made with 316L stainless steel. It was manufactured in our engineering room, which is no longer in operation. The TIR developed at our hospital is different because it is cannulated interiorly. This enables surgeons to align a temporary fragment using a guidewire. The smallest rod diameter of the proximal piece – the sleeve component – is 4 mm, which enables its use in younger children (Fig. 1a). The second piece, the obturator component, is also cannulated, has a 3.2-mm internal diameter, fits inside the first piece and its distal end has a 13-mm long thread to distal attachment. The external piece also has two proximal holes for fixation using transchondral sutures on the greater trochanter (Fig. 1b). The use of a complete rod (sleeve and obturator components) requires a canal diameter ≥ 4 mm.
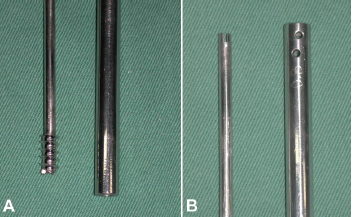
Telescopic intramedullary rod: (
Surgical techniques change depending on the indication for rod implantation – rod migration, fracture or deformity – which could consist only of repositioning in a case of migration; reduction and fixation in case of fractures; or single/multiple corrective osteotomy depending on the level of bone deformity. The rod length was calculated during surgical planning based on preoperative radiographs and the standard length was 14 cm to 20 cm. We had six different TIR sizes starting at 4 mm and finishing with a 9-mm diameter for the female component.
After the edge rusted and the medullary canal permeability was verified, the initial internal rod (the obturator component) was positioned through the entry of the fracture or osteotomy site, and the rod was passed retrograde until it emerged through the trochanteric portion and gluteus region. This stage is performed with a flexed limb and adducted hip, avoiding lesions in structures such as the sciatic nerve. In patients with canal impermeability, light drilling was performed using appropriate tools (Fig. 2). With the rod placed in the proximal fragment, bone realignment was performed using a guidewire to permit distal progression of the threaded rod until it was as centrally positioned as possible in the distal epiphysis. This second stage prepares the femur for receiving the external rod – the sleeve – which permits the component's telescopic movement. It was introduced into the femur by antegrade coupling to the proximal system, next to the great trochanter and transchondral suturing of the great trochanter was performed as soon as the rod reached its final position. This technique was performed in most patients.
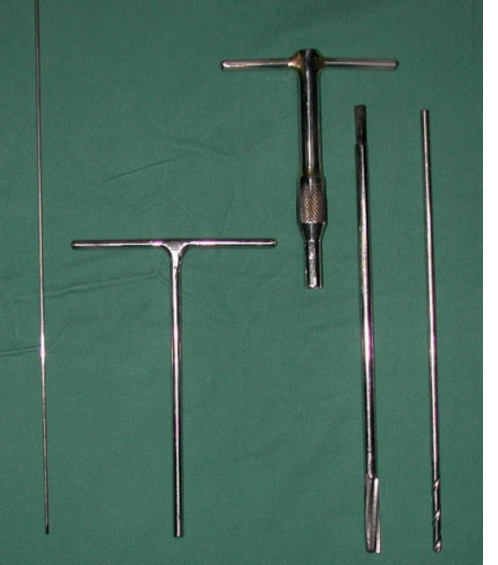
Instrumental tools for telescoping intramedullary rod installation.
Radiographic analysis
Specific aspects of treatment using TIRs were analyzed through imaging examinations (radiographs): male or female rod migration, the permanence period, most common locations of adjacent fracture and aspects related to telescopic or non-telescopic TIRs. Regarding the last parameter, imaging examinations were analyzed by comparing radiographic findings obtained on the first postoperative day when the rod was implanted and those obtained preoperatively before its removal or exchange. The evaluated parameter was the distal thread length (13 mm), which enables proportional size comparisons independently of the adopted radiographic technique that was used – printed or digital radiographs (real size or not) – through a simple rule of three to infer the length in centimetres. Of the 52 initially evaluated rods, only 35 had the required aforementioned data to be included in the radiographic analysis.
Statistical analysis
Data analysis was performed using Epi-info 7.2 version software (CDC, Atlanta, Georgia), which uses the chi-squared test and analysis of variance equations to evaluate whether data are statistically significant. Values were considered significant when p < 0.05, with a 95% confidence interval.
Results
We implanted 33 rods in boys and 22 rods in girls. The mean follow-up time was 9.96 years (3.39 to 14.54). Most patients were monitored for more than ten years. By the end of data collection, an average of 90% of subjects in our series still had at least one TIR. Patients were surgically treated for introduction and/or revision of approximately 2.5 rods, with the implantation of at least one and a maximum of five rods per patient. Fracture was the main surgical indication for rod implantation in 35 patients (67.31%), followed by deformity correction in nine (17.31%) and migration revision in eight (15.28%).
The five to ten-year-old age group required the most surgical procedures (25 events), followed by the under five years group (14 events) and over ten years group (13 events). Additionally, the five to ten-year-old age group had the most revision operations with a 68% revision rate (Table 1).
Revision rates (%) per age of rod implantation

A total of 16 patients (76.19%) underwent operations in both femurs. Regarding the Sillence classification, most patients were type III and IV (Table 2). Approximately 50% of the implanted rods required revisions, and patients with type III required a higher number of operations, totalling 19 revisions of 28 rods (67.86%) (Table 3); only seven of 22 rods implanted in patients with type IV were revised (31.82%). Rods required revisions every 6.43 years (SD 3.88) on mean. Patients with type III presented with a slightly lower mean age of 5.56 years (SD 3.86) and patients with type IV presented with a slightly higher mean age of 7.13 years (SD 3.72). However, this difference was not statistically significant.
Number of rods per subtype of osteogenesis imperfecta

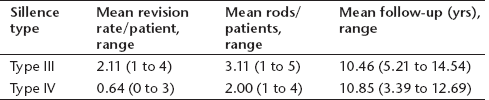
Revision rates by subtype of osteogenesis imperfecta
In 11 revisions, the rod was replaced by another TIR, whereas in seven the rod was replaced by FD rods; the remaining four rods were replaced by non-telescopic rods. Four patients did not require replacement, only removal. The causes of revision were fractures (15 rods), male or female migration (nine rods) and femur osteomyelitis in one patient (two rods) (Fig. 3). The most common place for the occurrence of a fracture was in the proximal third of the rod (five cases), followed by the middle of the rod (five cases); above the rod bone fracture occurred once, once in the lower third and once inferiorly of the rod. In five cases we could not identify the place of the fracture (lack of radiographic image).
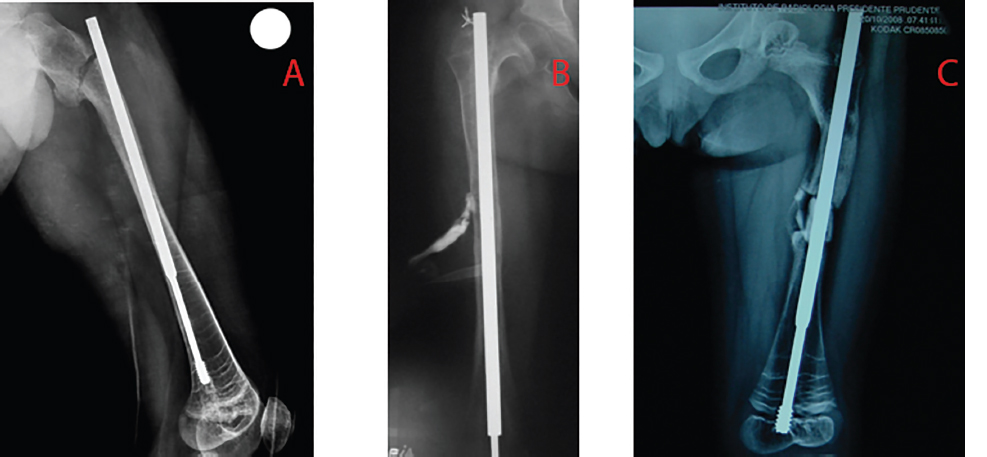
Causes of review surgery: (
To analyze the telescopic capability of the rod and its magnitude, only 35 rods of those with complete radiographic data were used. Telescoping was observed in 21 rods (60%). These data were cross-analyzed with the clinical type of OI, age and gender. Gender was the only parameter with some significance (p < 0.05), with male gender showing less risk of complications (Table 4). Regarding the telescopic magnitude, the mean percentage growth of the rods was 23.57% (SD 6.97), and the mean absolute number was 4.83 cm (SD 3.06) (Fig. 4). The main reason for telescopic absence was male migration, representing 50.00% of all patients (seven rods), followed by the absence of bone growth due to skeletal maturity in three of four patients (28.58% of all patients); one patient required rod revision at less than one year postoperatively. One patient had female migration, one had male and female migration and one had synthesis material failure, each accounting for 7.14% of patients.
Telescoping capability of the rod by gender
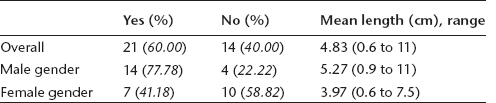
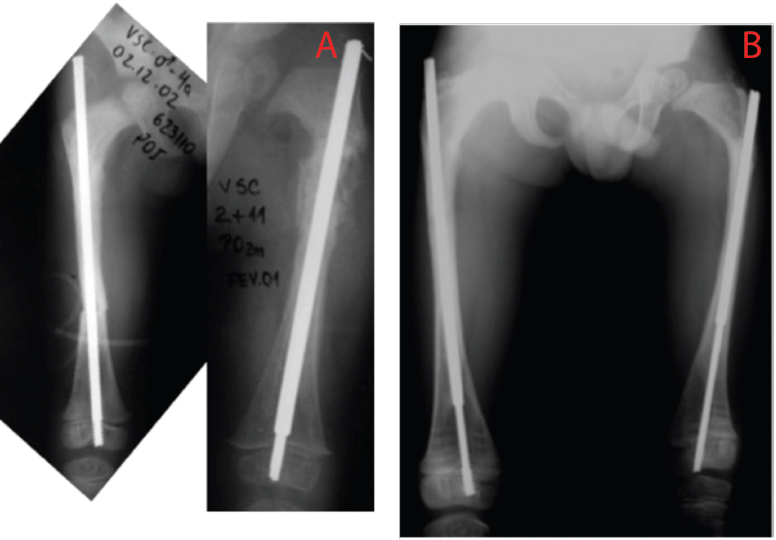
Effective telescopic capacity: (
Mid-term TIR results were evaluated from the data of 13 patients monitored for more than ten years. Among these, seven were classified as Sillence type IV, five as type III and one as type I. Five patients did not require revision operations; however, three required one TIR revision, three required revisions for two rods, two required revisions for three rods, and one required revisions for four rods, totalling 17 revision operations. Surgical indications included fracture in ten patients, migration in five, and infection in two, resulting in a 47.22% revision rate. The lifespan of each rod in these patients was 6.93 years (SD 4.22).
Discussion
Initially, OI must be clinically treated using bisphosphonates to increase bone resistance and mineral density17–24. In moderate and severe cases where children present with excessive fractures or deformities, surgical treatment using intramedullary rods is recommended3,10,25–27,which aids in correcting these problems and facilitates the possibility of walking in severely affected patients, thus improving their quality of life2,6,10,13,27–31. Telescopic rods have evident advantages, as they require fewer surgical interventions in response to children's growth compared with non-telescopic rods because of their ability to adapt to bone growth, serve as an internal template and prevent deformities3,9,32–35. Various telescopic rods have been designed; the TIR (designed, produced and first used in 2000) and FD rod (first reported in 2004) are notable examples.
Recent literature recommends the FD rod since studies have reported lower complication rates and a higher permanence period2,12–14,26. In our study, we verified that the TIR had lower revision rates for up to 36 months of rod permanence than the FD rod.12–14 In 2006, Fassier et al 12 analyzed the first patients with a minimum six-month follow-up and Birke et al 14 published a one-year follow-up study in 2011. Both studies found a 14.6% complication rate; the TIR had complications rates of 3.85% during the first six months (two rods) and 12.46% during the first 12 months (seven rods) (Table 5). Regarding permanence, the literature28,36 suggests that the results are satisfactory when at least 77% of the telescopic rods have at least three years of permanence, which the TIR is able to achieve (permanence rate for this period: 78.85%). The complications observed in our patients are consistent with those reported in the literature; fracture and migration are complications inherent to the disease's evolution and the use of rods.4,6,10,12,14,25,28,29,31,36–41 The role of the fracture, as the main complication, is more evident if only rods monitored for more than ten years are analyzed. We agree with Azzam et al 31 who reported that non-surgical patients have a higher fracture rate.
Complication rate (%) of each type of rod by follow-up period

TIR, telescoping intramedullary rod; FD, Fassier-Duval rod
By analyzing the effectiveness of rods in patients with Sillence type III OI, we observed more complications and an increased requirement for revisions compared with other patients; the same was observed by Lee et al, 25 Escribano-Rey et al, 27 and Boutaud et al. 32 These findings lead to the question of whether rods are more efficient for patients with type IV OI or whether the complication rate is related to the clinical severity among these patients.
The evaluation of complications among TIR groups, distributed by age, have showed that most revision operations were required in patients that had surgery between five and ten years old (Table 1). We were unable to identify characteristics of this age group that could be isolated as the main complication factor. Patient distribution per Sillence subtype among all ages was similar, as was the rod monitoring period for the other age groups: less than five-years-old (5.32 years, SD 3.33) and five to ten-years-old (5.04 years, SD 3.33).
A TIR-related limitation is that it was developed only for femoral operation since it requires a distal epiphysis sufficiently long for permitting fixation of the internal component's thread, which is 13 mm long and thus limits its use in the tibia. The main limitation with both components (sleeve and obturator) of telescopic rods is the presence of a narrow medullary canal, as the TIR also requires a minimum diameter for the medullary canal (3.2 mm) for both components to be used as a telescopic system. 31
Regarding the failure rate related to telescoping, it ranges from 2.7% to 33% for the FD rod and is 3.5% for the Baley-Dubow rod;9,12,14,19,36,38 however, these studies do not present quantitative data. Besides, the Baley-Dubow rod has an intra-articular distal femur entry point, which is a disadvantage.
The ability of telescoping rods to lengthen with bone growth is one of their main characteristics and advantages, and one of the most important variables for evaluating their success as an internal template for immature skeletons. If a minimum stretch is considered, from which it behaves similarly to a common non-telescopic rod, we may obtain another important parameter for comparison with the current literature and other rods. However, these data were not found previously, which hindered the analysis of an ideal interval from which the rod would be considered as non-telescopic. Moreover, previous studies have not described growth percentage and its absolute value; we attribute this to the significant difficulty in obtaining fixed parameters that may be compared throughout the follow-up period.
Our study found a significant difference in the telescoping rate between boys and girls. In boys, 14 rods telescoped and four did not, whereas in girls, only seven of 17 rods telescoped. These data may be subjectively correlated with bone density, which is greater in boys than in girls,42–44suggesting improved rod fixation and lower rates of screw migration from the epiphysis.
The major cause of non-telescoping rod is female migration; 7% to 36% of Baley-Dubow rods, 13% to 41% of FD rods and 3.3% of rigid rods had migration of the female component.9,12,14,25,36,39Our study identified a higher number of obturator component migration cases, as 57.14% rods did not telescope because of male migration of this component and 14.28% cases were caused by the sleeve component migration proximally. We attributed this difference to specific characteristics of other rods, which presented, in some cases, as robust fixation mechanisms on the distal portion, including intra-articular fixation of the knee; the same mechanism was not present for proximal fixation.14,25,37,38The TIR involves transchondral suturing for proximal fixation and a thread for distal fixation.
The mean follow-up period in this study (9.96 years) is superior to those found in previous studies describing the use of telescopic and non-telescopic rods for OI. At the end of the follow-up, > 90% of our patients still had at least one TIR.
A distinct characteristic of our TIR in relation to other described rods is its cannulation of both components, which is particularly useful during positioning. Another factor is that in our experience, solid rods may break under mechanical stress in cases of defective material, whereas cannulated rods tend to bend, which facilitates their removal, if necessary.
Our data demonstrated the effectiveness of TIRs2,12–14,31 for patients with OI. The TIR has a lower complication rate than the FD rod, which is most supported by the literature. The increased cost of the FD rod is compensated by the reduced need for revisions. 40 We obtained similar results using the TIR at costs < 1% of the FD. Thus, this is an extremely feasible option.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.