
Abstract
Purpose:
Telescoping intramedullary rods have transformed the management of long bone deformity and fragility fractures in children, yet complications and revision surgery remain common. This systematic review synthesizes outcomes across telescoping systems to evaluate complication and revision rates, telescoping success, and design evolution to guide implant selection and surgical decision-making in pediatric orthopedics.
Methods:
A search was conducted through July 2025 following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Studies reporting outcomes of telescoping rods in pediatric patients were included. Due to heterogeneity, results were synthesized descriptively and presented as weighted means per operated bone.
Results:
Thirty-three studies (861 patients; 2054 rods) were included. Weighted mean complication and revision rates were 49.6% and 25.7% for Bailey-Dubow rods, 61.1% and 24.5% for Sheffield rods, 37.1% and 30.5% for Fassier-Duval rods, 14.9% and 9.0% for corkscrew-locking rods, and 46.7% and 6.7% for distal-female rods. Telescoping success was 48% for Bailey-Dubow, 74% for Fassier-Duval, 94% for corkscrew, and 100% for distal-female designs. Variation in follow-up duration and definitions of complications contributed to differences in reported rates.
Conclusions:
Modern telescoping rods have reduced migration and mechanical failure compared with earlier designs, yet complication and revision rates remain substantial. Newer systems show encouraging early results but require longer follow-up for validation. Differences in bone anatomy and biomechanics strongly influence implant performance, underscoring the need to tailor rod selection to individual bones.
Significance:
This review consolidates published complication and revision rates across telescoping rod designs, establishing a foundation for comparison as newer implants are introduced and long-term outcome data become available.
Level of Evidence:
III.
Keywords
Introduction
Pediatric long bone deformities and recurrent fractures are common in bone fragility disorders, such as osteogenesis imperfecta (OI) and congenital tibial pseudarthrosis. Children present unique surgical challenges, as their bones are smaller, softer, and continually growing. Conventional fixation methods risk damaging the physis or requiring frequent revision as the child grows. Intramedullary fixation has therefore become central in pediatric orthopedics, offering stabilization along the length of the bone while preserving growth potential. 1 Intramedullary (IM) rodding has evolved significantly since Sofield and Millar 2 first described IM fixation with multiple osteotomies in 1959. Early non-telescoping solid rods provided mechanical support but were plagued by complications such as migration, frequent revisions, and failure to accommodate growth.3–5 These limitations necessitated the development of growth-accommodating implants, setting the stage for telescoping rod technology.
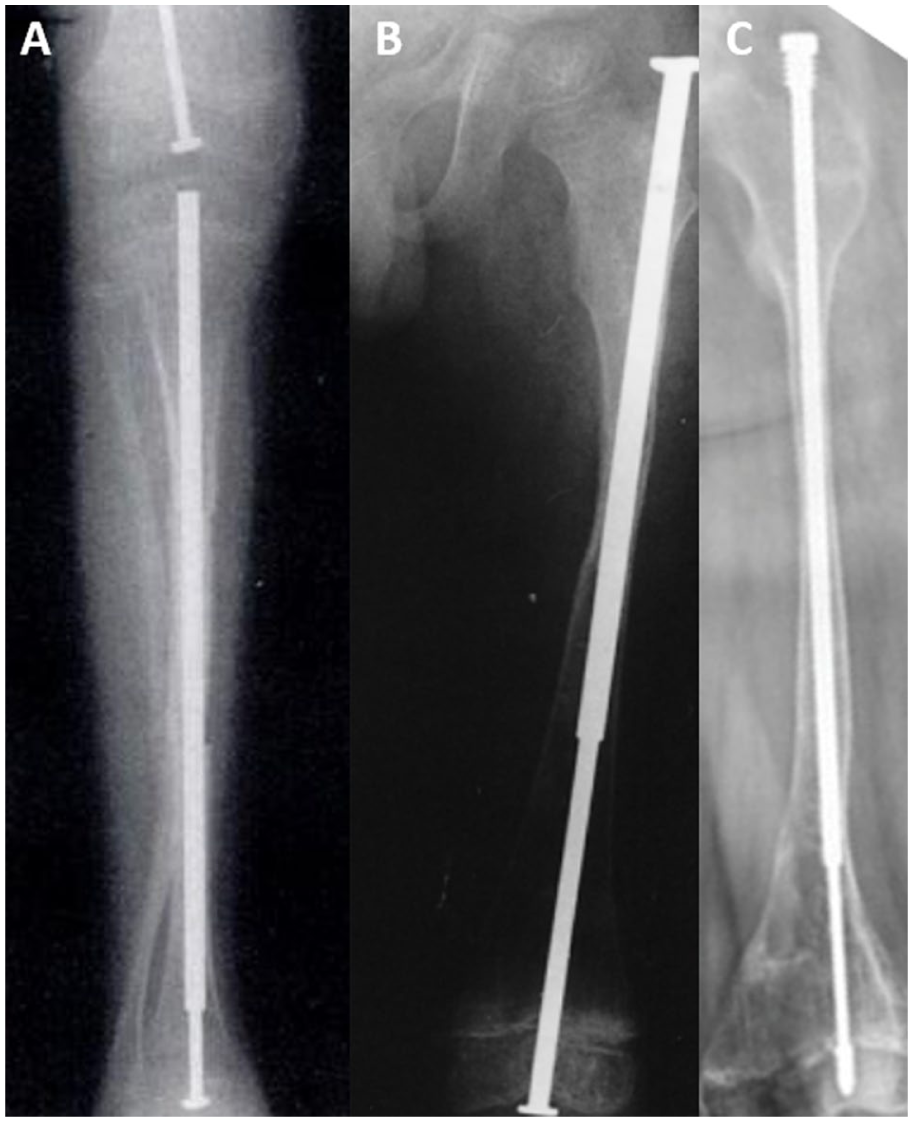
The first telescoping rod, the Bailey-Dubow (BD) rod, was introduced in 1963 by Robert Bailey and Harold Dubow. 6 It featured a male T-shaped rod sliding within a female cylinder, providing epiphyseal-to-epiphyseal fixation and lengthening with growth (Figure 1(a)). 1 However, the design required arthrotomies and often led to complications such as T-piece detachment and rod migration.7,8 In response, the Sheffield rod was developed in the late 1980s to overcome the limitations of the BD design, incorporating design changes, such as fixing the T-piece on both ends to prevent disconnection and migration (Figure 1(b)). 9 While the Sheffield system reduced certain complications, it still required revision surgeries due to rod-related failures. 9 The most significant advancement came in 2001 with the Fassier-Duval (FD) rod, developed by François Fassier and Pierre Duval (Figure 1(c)). This system enabled minimally invasive percutaneous insertion, sparing joint cartilage, and provided adjustable intraoperative sizing, leading to its widespread adoption and recognition as the standard of care in many centers. 1
Despite improvements, complications, such as migration, rod disengagement, and the need for revision surgery, persist with the FD system. 1 To address these, newer telescoping designs have been developed, including different distal locking mechanisms, like a corkscrew 13 (Figure 2(a)), or different biomechanical principles, like inserting the female part distally (Figure 2(b)). 14 In addition, lower-cost modifications of the FD rod have been reported in resource-limited settings, highlighting efforts to balance innovation with affordability and accessibility.15,16

Although telescoping rodding has transformed pediatric limb deformity management, significant challenges remain. Reported complication rates remain high, outcomes are variable, and there is no universal consensus on an optimal implant. Reported outcomes and complications are highly variable in the literature, with few randomized controlled trials or high-quality comparative studies available. As new designs continue to emerge, there is a pressing need to synthesize the evolving evidence. This systematic review aims to map the current landscape of telescoping rods in pediatric orthopedics, summarize innovations and complications, and identify gaps to guide future research and clinical practice.
Methods
Search strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A comprehensive literature search was executed during July 2025 using Ovid MEDLINE, Embase, and Scopus. The search strategy combined MeSH terms and text words, including telescoping rod, elongating rod, intramedullary nail, orthopedic surgery, bone deformity, and pediatric orthopedics. Boolean operators (or, and) and asterisks for truncation were used to optimize the search results. References of relevant studies were also reviewed.
Eligibility criteria
Studies were included if they met the following criteria: (1) randomized controlled trials, cohort studies, and case–control studies, (2) pediatric populations, (3) telescoping rods used in long bones, and (4) provided outcomes related to a specific telescoping rod.
Studies were excluded if they (1) were abstracts, case reports, cadaver studies, animal studies, (2) involved spinal rods, (3) used rods for limb lengthening (i.e., external fixation or magnetic rods), (4) combined data with solid rods, (5) lacked sufficient detail regarding the type of rod used, or (6) were not available in English or French.
Literature screening and data extraction
Search results from all databases were uploaded to Covidence, and duplicates were automatically removed. Titles and abstracts were screened in reviewer pairs to identify studies meeting the inclusion criteria. Full texts of eligible articles then underwent further screening. Disagreements were discussed between the two reviewers to reach a consensus, and conflicts were resolved by the senior author, a pediatric orthopedic surgeon.
Data were extracted by two reviewers using a standardized sheet created for this review. Extracted information included study characteristics (i.e., author, year), study design, population demographics (i.e., sample size, age, sex, follow-up, diagnosis, bones, ambulatory status, bisphosphonate use), surgical indications, rod type, complications, rod survival/revision rate, telescoping rate, functional outcomes, radiographic outcomes, and other key findings. The extracted data were stored in a Microsoft Excel spreadsheet.
Results
Study selection
A total of 33 studies met the inclusion criteria and were included in the final analysis (Figure 3). In total, 712 studies were excluded for reasons such as irrelevance to the research question, lack of extractable data, wrong study design, and unavailability of the full text.
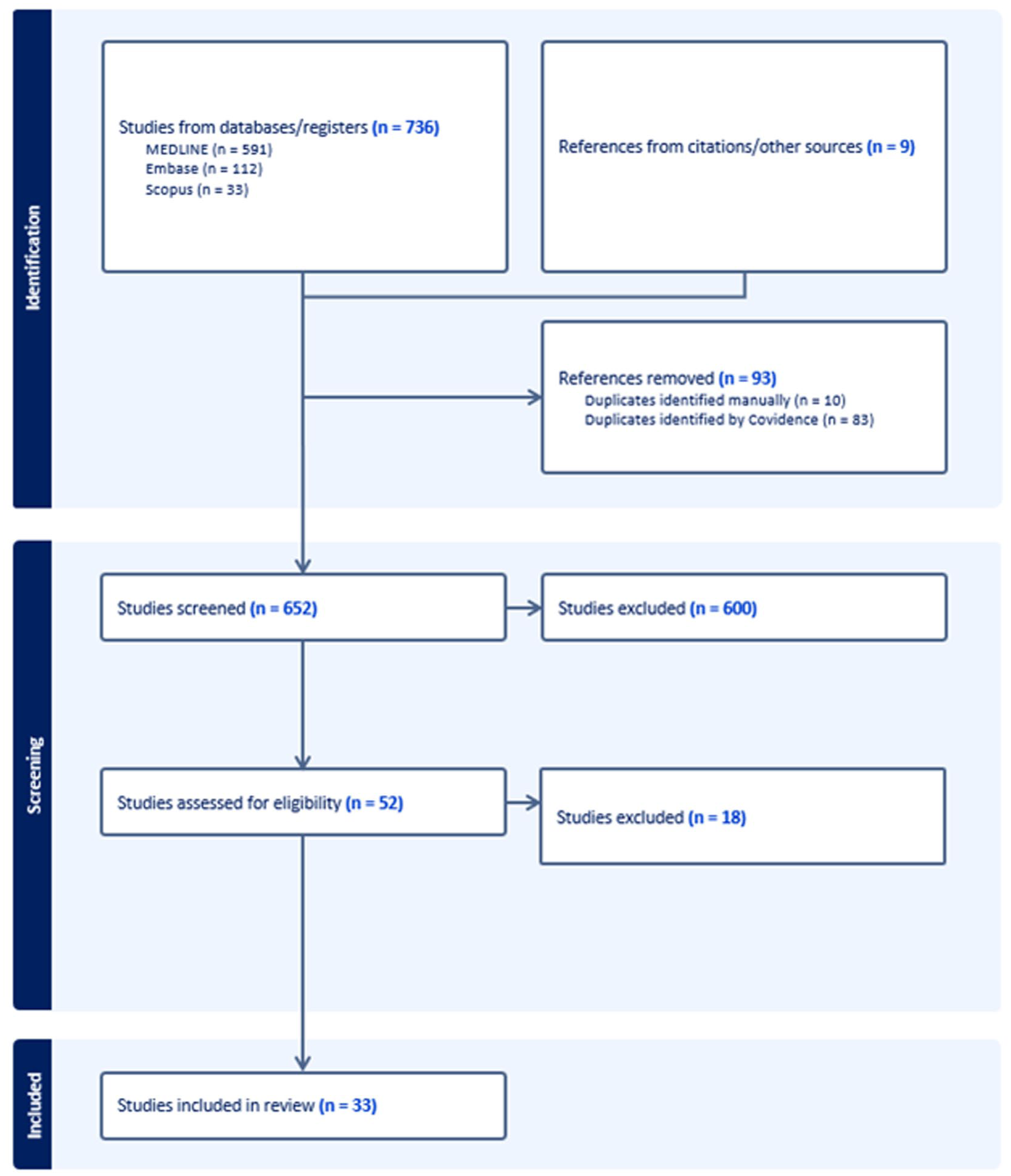
PRISMA flow diagram illustrating the study design.
All included studies were retrospective in design. The primary surgical indications reported across studies were limb deformity and fracture management. Reporting of patient ambulatory status and bisphosphonate use was inconsistent. A summary of study characteristics is presented in Table 1.
Study characteristics.
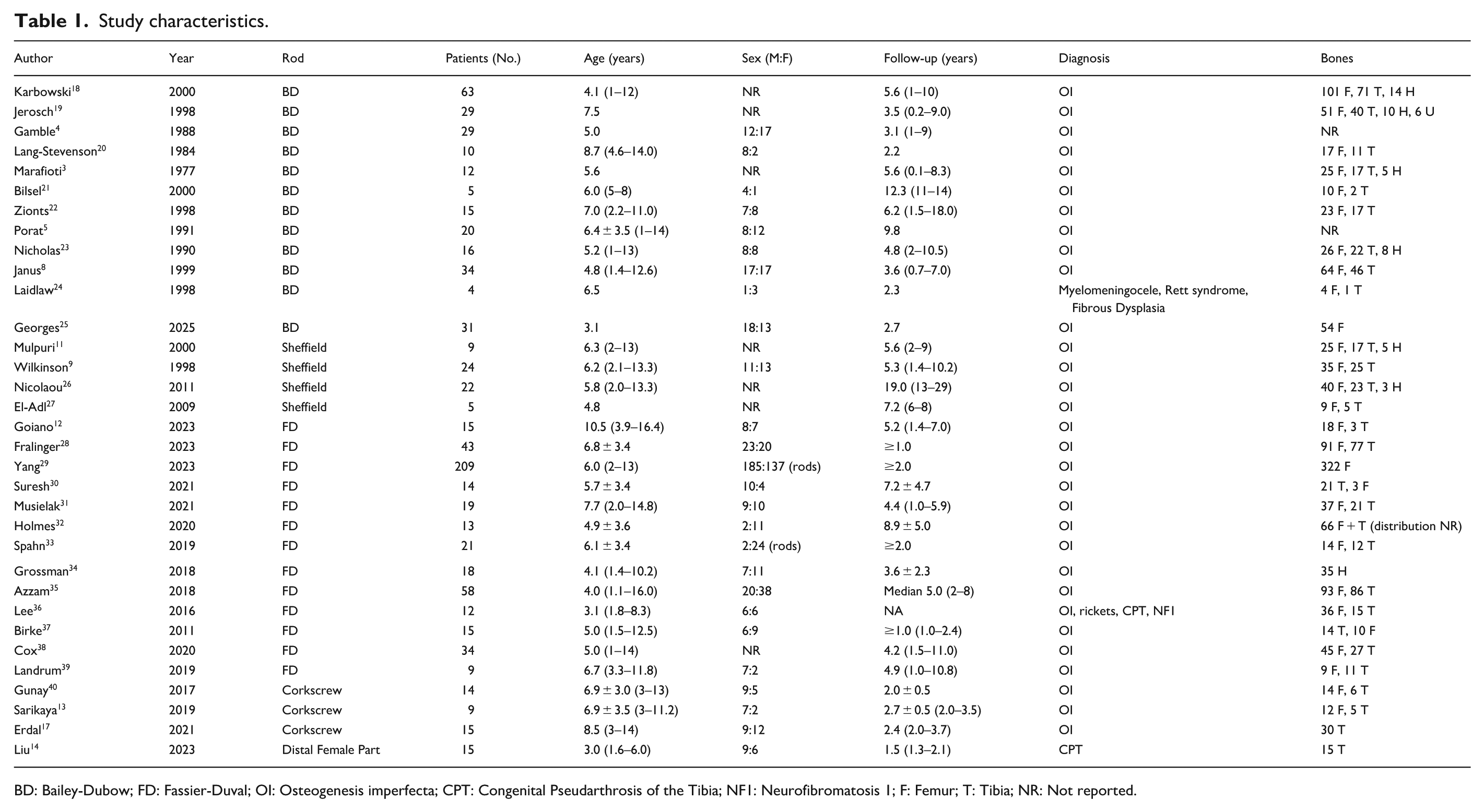
BD: Bailey-Dubow; FD: Fassier-Duval; OI: Osteogenesis imperfecta; CPT: Congenital Pseudarthrosis of the Tibia; NF1: Neurofibromatosis 1; F: Femur; T: Tibia; NR: Not reported.
The 33 included studies comprised 861 patients and 2054 rods. Studies were separated into 5 groups according to the type of telescoping rod evaluated: 12 studies on BD rods, 4 studies on Sheffield rods, 13 studies on FD rods, 3 studies on corkscrew locking rods, and 1 study on rods with a distal female segment. Intraoperative challenges, overall complication rates, specific complications, revision rates, and telescoping rates are summarized for each rod type. Considerable heterogeneity was present in the reporting of these outcomes, particularly revision rates and telescoping success, which were strongly influenced by variability in follow-up duration across studies. Telescoping success was defined as any increase in length across studies.
Bailey-Dubow rod
Twelve articles were identified discussing the Bailey-Dubow rod. Across these studies, 268 patients were included with a weighted mean age of 5.5 years at the time of surgery and a weighted mean follow-up of 5.0 years. Among those reporting on sex, 48.9% (n = 65) were male, and 51.1% (n = 68) were female. Most patients (98.3%) had a diagnosis of OI, while the remaining 1.7% presented with myelomeningocele, Rett syndrome, or fibrous dysplasia. Ten studies specified the treated bones. Among a total of 645 Bailey-Dubow rod insertions, there were 375 femurs, 227 tibias, 37 humeri, and 6 ulnas. Reported outcomes varied across studies, with complications, revisions, and telescoping rates summarized in Table 2. The weighted mean complication and revision rate per operated bone were 49.6% and 25.7%, respectively (Table 7).
Summary of reported complications, revision rates, and telescoping rates in studies of the Bailey-Dubow telescoping rod.
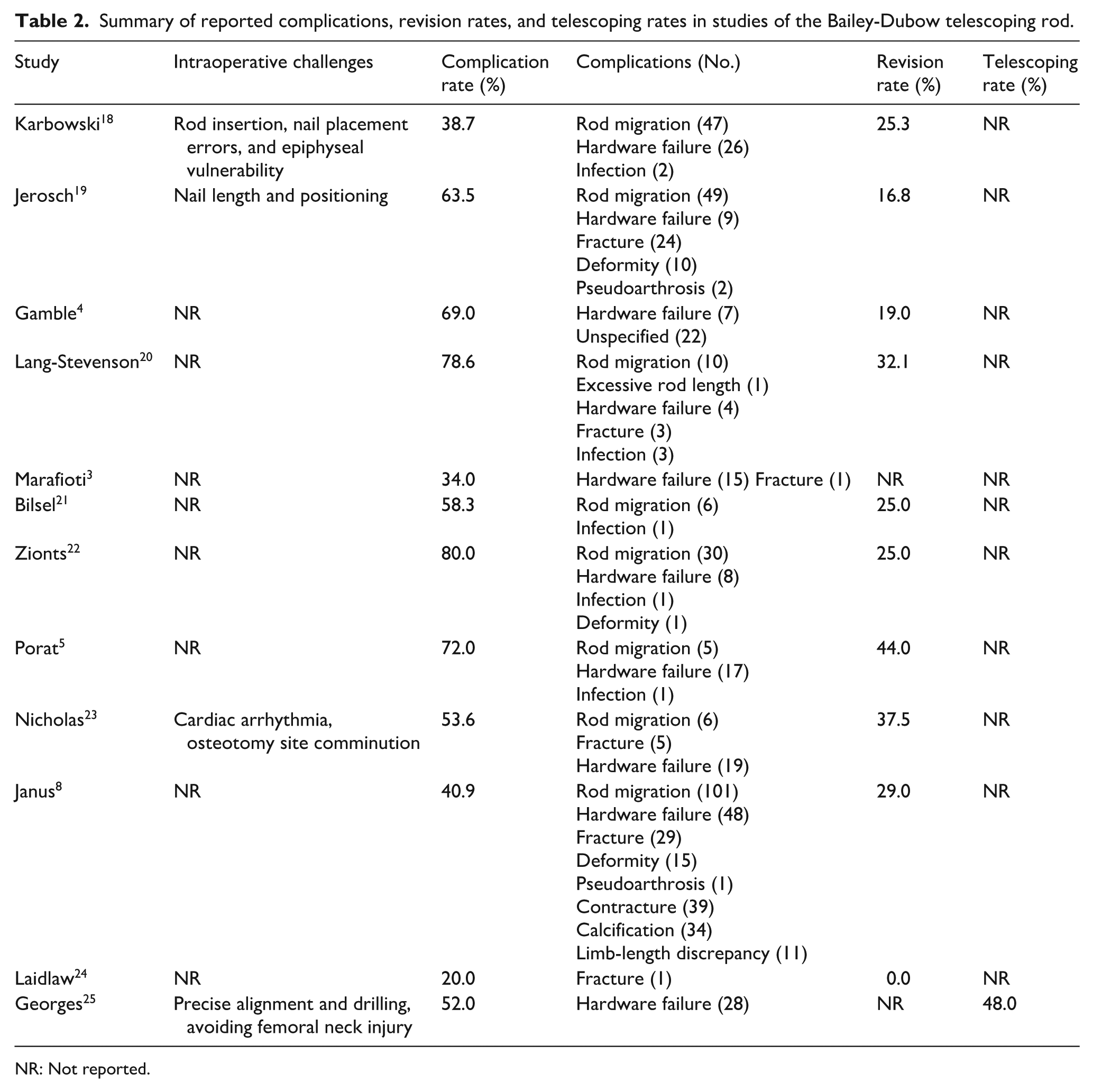
NR: Not reported.
Sheffield rod
Four articles examined the Sheffield telescoping rod, including a total of 60 patients with a weighted mean age of 6.0 years and a weighted mean follow-up time of 10.5 years. Sex was only reported by Wilkinson et al., and 54.2% (n = 11) were female. All patients (100%) had a diagnosis of OI. Across all studies, Sheffield telescoping rods were inserted into 187 bones, including 109 femurs, 70 tibias, and 8 humeri. Complication, revision, and telescoping rates for the Sheffield rod are summarized in Table 3. Per operated bone, there was a weighted mean complication rate of 61.1%, and a weighted mean revision rate of 24.5% (Table 7).
Summary of reported complications, revision rates, and telescoping rates in studies of the Sheffield telescoping rod.
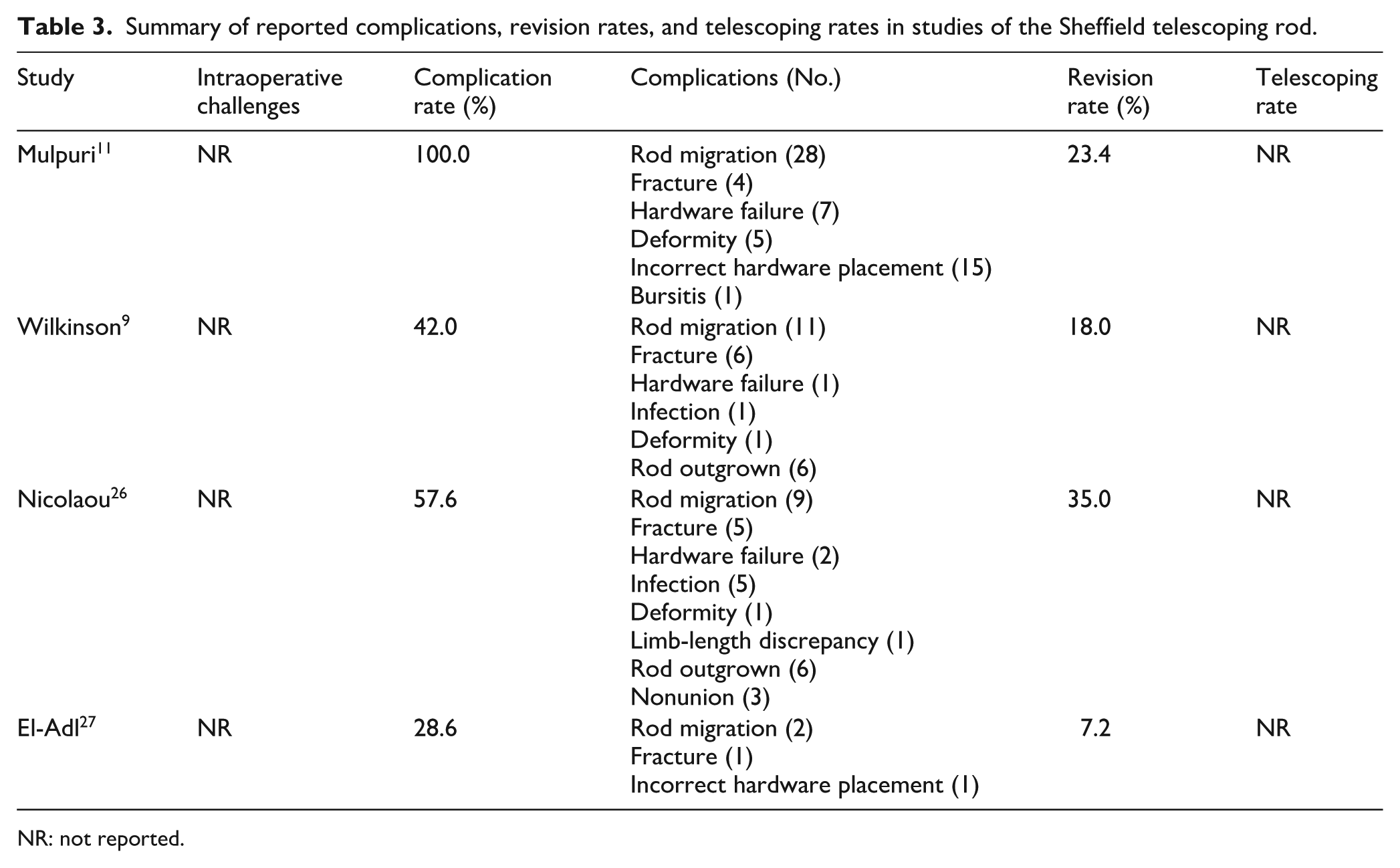
NR: not reported.
Fassier-Duval rod
Thirteen articles used the FD rod, including a total of 480 patients with a weighted mean age of 5.8 years and a weighted mean follow-up of 5.1 years. In 12 studies, all the patients had OI, while the remaining study included patients with OI, rickets, congenital pseudarthrosis of the tibia (CPT), and neurofibromatosis. Across the 13 studies, a total of 1066 FD rods were reported, including 678 femurs, 287 tibias, and 35 humeri. An additional 66 rods were placed in either the femur or tibia, but were not further specified. Data for each study are found in Table 4. The weighted mean complication rate per operated bone was 37.1%, while the weighted mean revision rate per operated bone was 30.5% (Table 7).
Summary of reported complications, revision rates, and telescoping rates in studies of the Fassier-Duval telescoping rod.
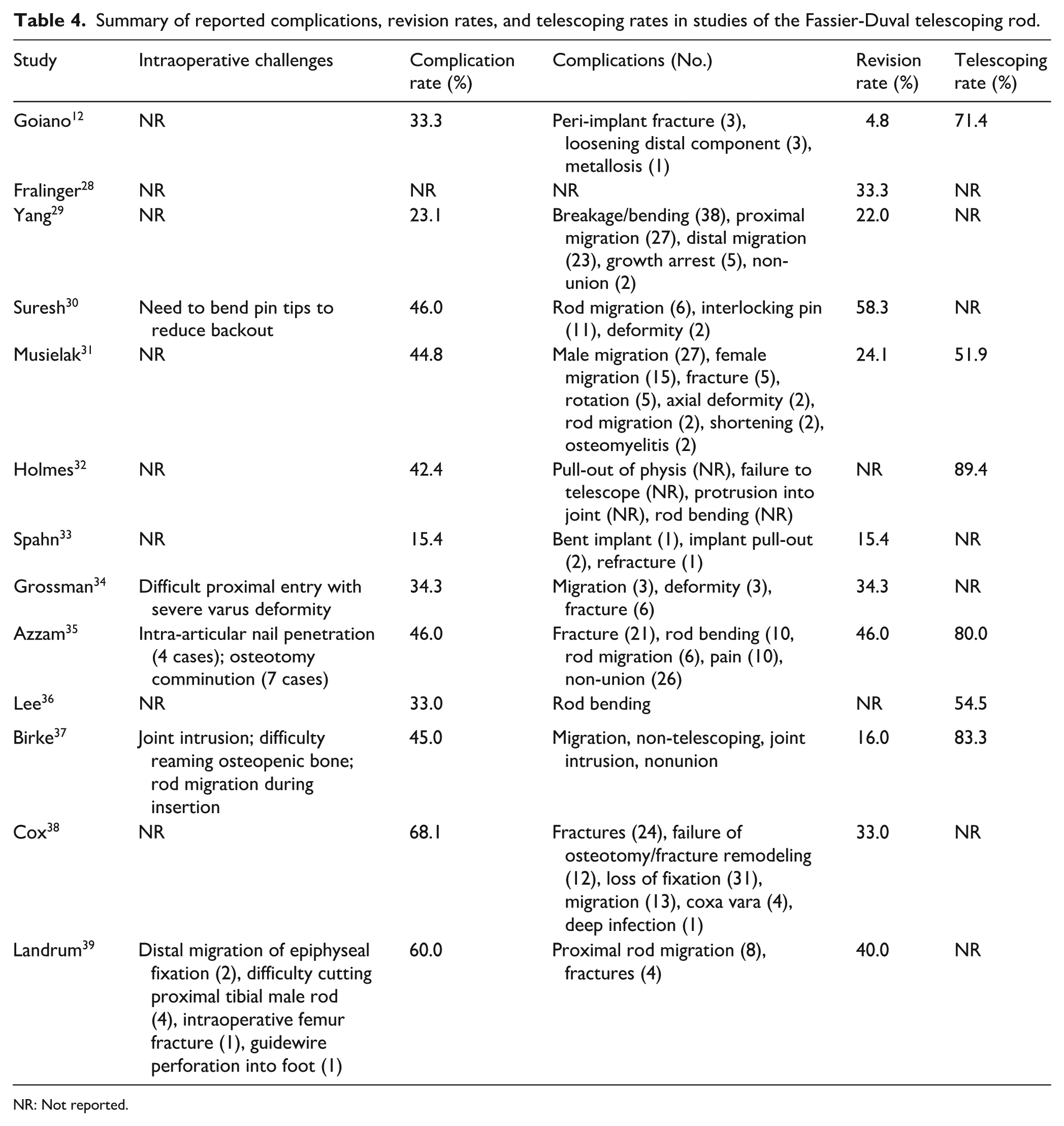
NR: Not reported.
Corkscrew rods
Three articles reported on the use of corkscrew rods, including a total of 38 patients with a weighted mean age of 7.8 years and a weighted mean follow-up of 2.4 years. All patients had a diagnosis of OI. Across all studies, 67 corkscrew rods were inserted, comprising 26 femurs and 41 tibias. Data for both studies are shown in Table 5. The weighted mean complication rate was 14.9%, while the weighted mean revision rate was 9.0% (Table 7).
Summary of reported complications, revision rates, and telescoping rates in studies of corkscrew telescoping rods.
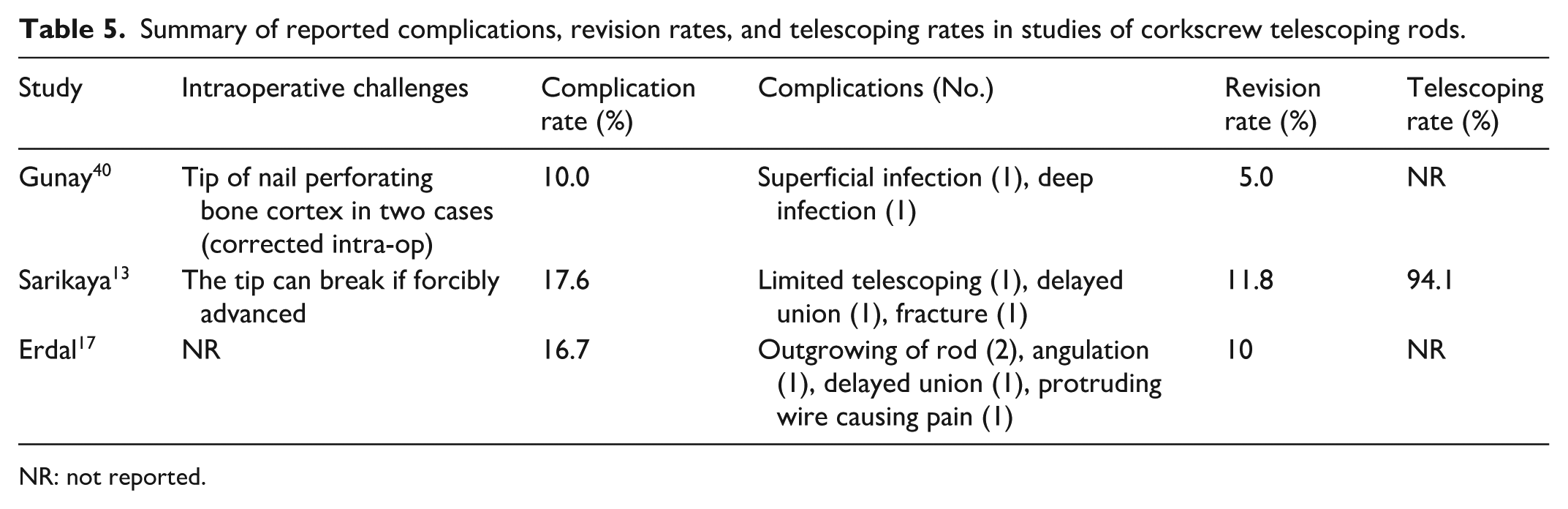
NR: not reported.
Distal female segment rods
At the time of our search, one study described a telescoping rod with a female distal segment. This study used 15 rods in 15 patients with a mean age of 3.0 years and a mean follow-up of 1.5 years. All patients were diagnosed with unilateral Crawford type 4 CPT, and all rods were inserted in the tibia. Outcomes are described in Table 6.
Summary of reported complications, revision rates, and telescoping rates in studies of distal female segment telescoping rods.

NR: not reported.
Summary of outcomes for each rod.
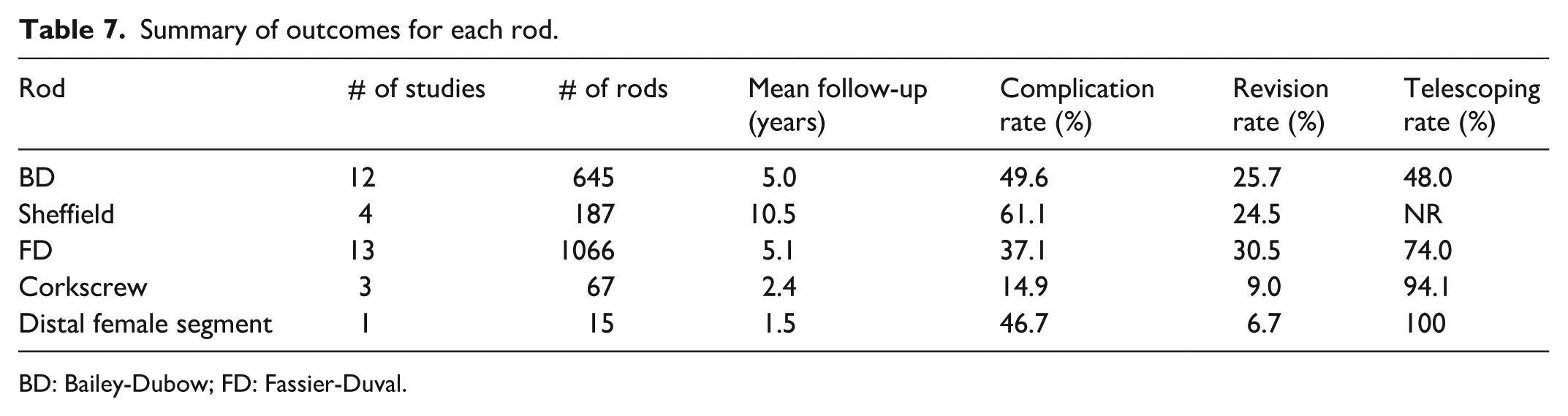
BD: Bailey-Dubow; FD: Fassier-Duval.
All of the Sheffield and corkscrew rods were used in patients with OI, and all of the distal female segment rods were used in patients with CPT. There was one study in each of the BD and FD rod groups, which included patients with diagnoses other than OI. Analyzing the complications, revision, and telescoping rates in these groups, excluding the mixed studies, gives similar results. For BD rods, in patients with OI, the complication rate is 49.8%, the revision rate is 25.9%, and the telescoping rate is 48.0%. For FD rods, in patients with OI, the complication rate is 37.3%, the revision rate is 30.5%, and the telescoping rate is 76.8%.
Discussion
The development of telescoping intramedullary rods was driven by the need to reduce repeated surgeries in children with OI and other bone fragility disorders. Non-elongating devices frequently require replacement as the child grows, leading to multiple hospitalizations and increased surgical risk. Over time, several designs have been introduced, aiming to improve stability, ease of insertion, and long-term durability. For example, various distal fixation tip designs have emerged and continue evolving across the different generations of implants (Figure 4). Current evidence shows wide variation in outcomes across systems, reflecting the ongoing refinement of implant technology and surgical technique. Although some of the challenges seen with earlier devices have improved, there is still room for optimization.
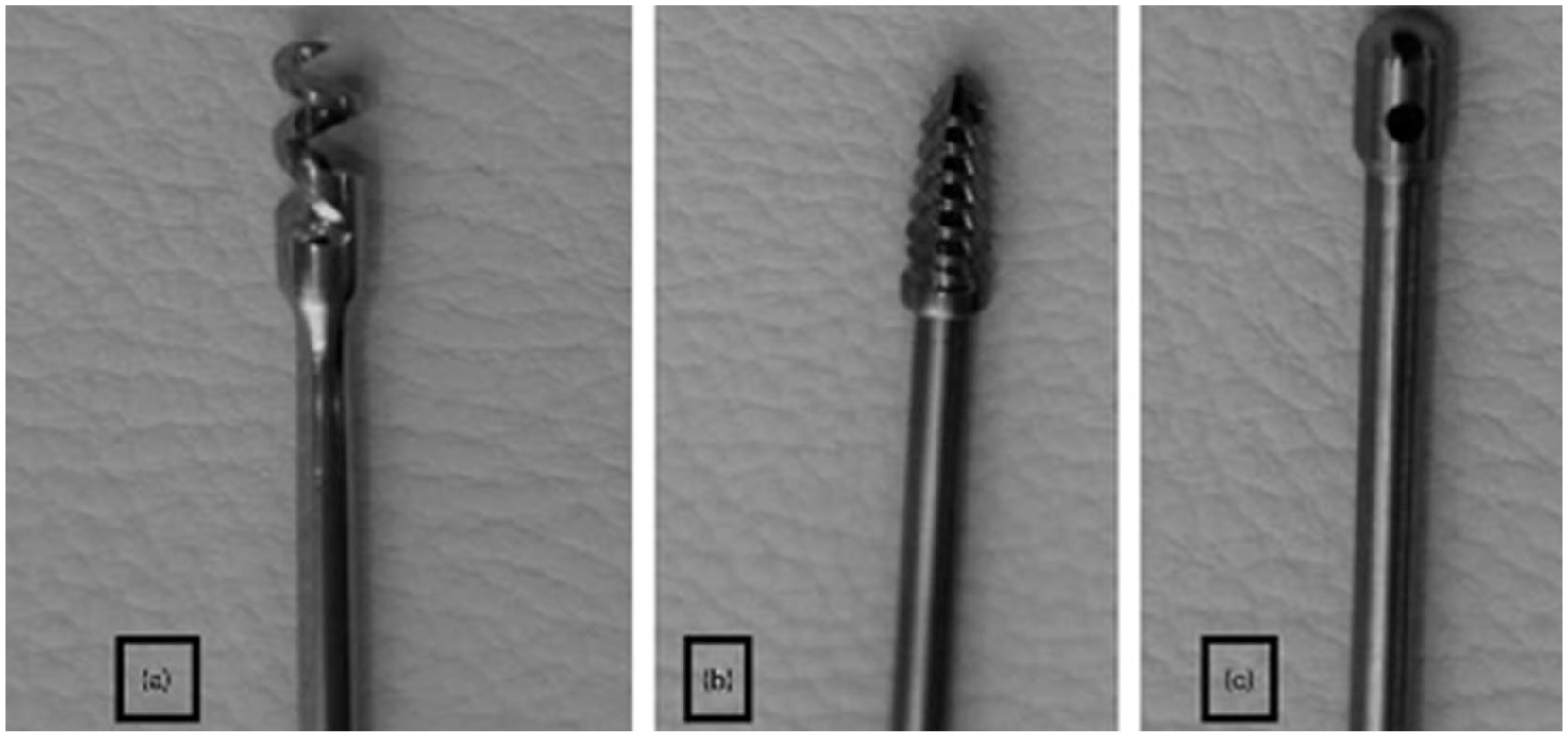
Examples of distal fixation tips in telescoping intramedullary rods: (a) corkscrew, (b) threaded, and (c) non-threaded designs. 13
When comparing outcomes between the rods, clear differences emerge between earlier and more recent designs. The BD and Sheffield rods, which represented important early advances, are consistently associated with high complication rates, including rod migration, component disengagement, and hardware failure. The FD rod is currently the most widely used telescoping rod and demonstrates lower rates of complication compared to its predecessors. Nonetheless, rod failures due to bending, migration, and failed telescoping remain present (Figure 5). Newer designs, such as corkscrew locking rods and rods incorporating a distal female segment, have been developed to address these challenges and to accommodate the wide variability in long bone deformities seen in these populations, but follow-up times remain shorter than those of the other rods, so complication and revision rates should be interpreted accordingly.
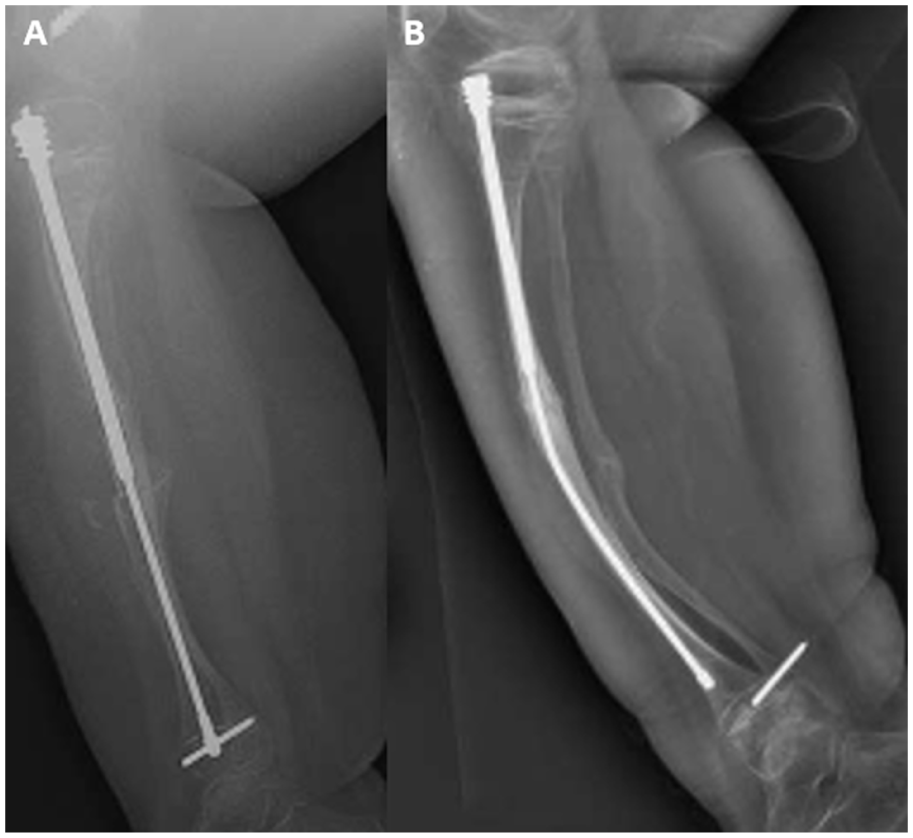
Radiographs demonstrating rod outcomes: (a) Immediately postoperative, showing appropriate alignment and fixation; (b) four years later, with rod bending, loss of distal fixation, and arrest of telescoping. 36
Traditionally, identical telescoping rod designs have been applied to both the femur and tibia, despite important anatomical and biomechanical bony differences. The tibia, which is subcutaneous and subjected to greater bending forces, is more prone to severe angulation and recurrent deformity, whereas the femur demonstrates more rapid longitudinal growth. These distinctions suggest that bone-specific design features may be advantageous: a distal female segment may improve tibial stability by reducing the risk of recurrent deformity and hardware failure, while a stronger distal locking mechanism, such as the corkscrew design, may better accommodate the femur’s faster growth. Clinical data for these systems, however, remain limited. To date, only three studies have reported outcomes for the corkscrew rod, and a single study has described a distal female rod of unspecified design. No large peer-reviewed series exists for either design. Recently, the Rodeo™ nail (OrthoFix, Lewisville, TX, USA) and the TST™ nail (TST Medical Devices, Istanbul, Turkey) have been introduced as next-generation telescoping rods designed to address the shortcomings of earlier systems. The Rodeo™ nail, which recently received FDA approval, is a telescoping rod that incorporates a distal female segment inserted from below, whereas the TST™ nail features a distal corkscrew locking mechanism intended to enhance stability and reduce migration. The clinical performance of both systems will become clearer as peer-reviewed outcomes begin to emerge.
In addition to the five groups of telescoping rods included in this review, other designs have been developed in resource-limited studies while adopting the same telescoping concept. Rangasamy et al. 16 described a novel, low-cost telescopic nail constructed from a modified Küntscher nail as the female component and an ulnar square nail as the male component, with additional modifications to allow both proximal and distal locking (Figure 6(a)). The interlocking geometry of the square profile within the cloverleaf Küntscher nail was intended to provide rotational stability. The device was used for intramedullary fixation of the femur and tibia in children with OI. With an estimated cost of approximately $25 USD compared to $200–240 USD for other telescopic nails available in the Indian market, a key advantage of this system was its affordability, 16 However, the authors reported technical issues, including difficulty with the telescoping mechanism, attributed to non-uniformity in the cut ends of the components. Similarly, Rosemberg et al. 15 reported on a telescopic intramedullary rod developed and manufactured locally in Brazil for use in patients with moderate to severe OI (Figure 6(b)). The device consisted of two stainless-steel components, with proximal fixation achieved through transchondral sutures at the greater trochanter and distal fixation provided by a threaded male component. In their series of 21 patients undergoing 52 femoral procedures with nearly 10 years of follow-up, they found revision rates were lower than those reported for the FD rod at comparable intervals. Fracture and rod migration were the most common causes of failure. Importantly, the results were obtained using a rod at costs less than 1% of the FD rod. 15 Although both of these systems remain limited to small institutional experiences, they demonstrate how locally engineered solutions can expand access to telescoping technology in low- and middle-income countries.
The FD rod remains the most widely used telescoping system and continues to serve as the benchmark against which newer devices are measured. Its design has mitigated many of the problems seen with early implants, yet revision and complication rates are still far from negligible. Emerging options, including corkscrew-locking rods and rods with a distal female segment, are promising innovations. Yet, their true value will only become evident with longer follow-up and larger series. For now, implant selection should be individualized, considering the bone involved, the degree of deformity, and the available resources. Large, prospective, multicenter studies are needed to assess complication rates, revision rates, and functional outcomes. This review provides a foundation for further development by highlighting both the strengths and shortcomings of current devices. With better data and continued design refinements, telescoping rods have the potential to reduce the number of required operations and improve long-term function in children with OI.
Limitations
All included studies were retrospective and primarily consisted of small, single-center series, increasing the risk of selection and reporting bias. There was considerable heterogeneity in definitions of outcomes such as “complication,” “revision,” and “telescoping success,” making direct comparisons between rods challenging. Variability in follow-up duration also likely influenced reported complication and revision rates, as studies with longer observation periods naturally capture more cumulative events. In addition, functional outcomes, such as gait performance or standardized mobility scores, were rarely reported, limiting assessment of the true clinical impact of each implant type. Hence, these factors should be considered when interpreting the findings and highlight the need for prospective, standardized multicenter studies in the future.
Conclusion
Telescoping intramedullary rods have transformed the surgical management of children with OI and other bone fragility disorders by offering a means of reducing repeated operations during growth. The evolution from early systems, such as the BD and Sheffield rods, to the more widely adopted FD design reflects steady improvements in stability, ease of use, and clinical outcomes. Newer concepts, including corkscrew-locking rods and rods with a distal female segment, aim to address persistent challenges such as migration and recurrent deformity. Nonetheless, these innovations require long-term validation before widespread adoption. With more options now emerging, treatment should be tailored to the bone involved and its biomechanical demands.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261423059 – Supplemental material for Evolution and outcomes of telescoping intramedullary rods in pediatric bone fragility disorders: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521261423059 for Evolution and outcomes of telescoping intramedullary rods in pediatric bone fragility disorders: A systematic review by Peter Joseph Mounsef, Jack Legler, Dev Patel and Reggie Hamdy in Journal of Children's Orthopaedics
Footnotes
Author contributions
Data availability statement
No new data were created or analyzed in this study. All data used in this systematic review were obtained from previously published studies cited within the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article is a systematic review of previously published studies and does not contain any studies with human participants or animals performed by any of the authors. Therefore, ethical approval and informed consent were not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.