
Abstract
Abstract
Purpose
Proximal tibia impaction fractures are specific injuries, usually caused by trampolining. They may associate with later growth disturbances. There is sparse understanding about their recent epidemiology, in particular the changing incidence. Their typical radiographic findings are not completely known.
Methods
All children, aged < 16 years, who had suffered from proximal tibia fracture in Oulu Arc and Oulu between 2006 and 2017 were enrolled (n = 101). Their annual incidence was determined using the official population-at-risk, obtained from the Statistics Finland. The specific characteristics and risk factors of the patients and their fractures were evaluated. Radiographic findings were analyzed, in particular the anterior tilting of the proximal growth plate, due to impaction.
Results
The annual incidence increased two-fold from 9.5 per 100 000 children (2006 to 2009) to 22.0 per 100 000 (2014 to 2017) (difference: 12.5; 95% confidence interval 5.1 to 20.3 per 100 000; p = 0.0008). The mean annual incidence of trampoline impaction leg fractures was 15.4 per 100 000 children. In 80% of the cases multiple children had been jumping together on the trampoline. Anterior tilting (mean 7.3°, SD 2.5°, 6.1° to 19.1°)) of the proximal tibial plate was seen in 68.3% of the patients. Satisfactory bone union was found in 92.7% during follow-up. Isolated patients presented delayed bone healing.
Conclusion
The incidence of trampoline leg fractures has increased 130% during the 12 years of the study period. Many of these injuries could have been prevented by avoiding having several jumpers on the trampoline at the same time. Anterior tilting of the growth plate was a common finding and should be recognized in the primary radiographs.
Level of evidence
IV
Keywords
Introduction
Trampoline-related fractures have increased dramatically during the last 15 to 20 years, as the popularity of backyard trampolines has increased. 1 The increase in injuries has been well described in North America, 2 Europe,3–5 Australia 6 and Asia. 7 Most (95%) trampoline injuries are slight and do not require any hospital treatment.8,9 Male predominance and the mean age of 11 years among all patients with a trampoline injury has been reported. 10 Trampoline injuries usually occur at home on the body of the trampoline, while falling off the trampoline has not been common since safety nets have become more popular.8,11
Proximal tibiae impaction fractures are special paediatric injuries, which are usually caused by trampoline jumping. 12 There is typically a particular mechanism: as children often do not jump alone on the trampoline, there is a risk that the smaller child lands on the upward moving trampoline mat, and a great upward kinetic force, as a consequence of the heavier jumper's jump, is applied to the descending child's leg.13,14 With knees held in hyperextension, compressive force is directed to the anterior cortex and distracting force to the posterior cortex. As a result, a transverse hairline impaction fracture of the proximal tibiae with the anterior buckle occurs. Anterior tilting of the proximal growth plate may accompany. The primary radiographic findings may be slight, in which cases diagnoses may be missed. However, the fractures may result in disturbed growth.15,16
There is a lack of current literature concerning trampoline fractures of the proximal tibia. To our understanding, no longitudinal population-based evidence of the recent epidemiology of typical trampoline leg fractures is available, while much recent research has focused on the more severe trampoline injuries.9,17,18 Taking into account that the proximal tibia physis is still one of the most vulnerable bones in the entire skeleton,15,16,19–21 trampoline leg fractures should not be overlooked.13,22 We, therefore, aimed to study the annual incidence and its potential changing trend, risk factors and clinical and radiographic characteristics of trampoline-related proximal tibiae fractures in children.
Patients and methods
The study population comprised all children < 16 years of age with a proximal tibiae impaction fracture caused by trampoline injury. For patient recruitment, we first reviewed all patients with a diagnosed upper tibiae fracture, according to the International Classification of Diseases (ICD-10) (https://icd.who.int/browse10/2016/en) by using the codes S82.1 and S82.8 to S82.9 for screening. All injury characteristics were reviewed from hospital journal charts to confirm that injuries were caused in trampoline jumping. If the injury history was unclear, the case was excluded. The study was performed in the Oulu University Hospital, between 2006 and 2017 and Oulu Arc and Oulu were taken as the geographic study area. There are no other round-the-clock paediatric trauma units in the area. Furthermore, isolated children with bone fractures, who had been treated elsewhere in the public healthcare units, were admitted to the research trauma centre for their out-of-hospital follow-up and thus included. Potential patients with a trampoline leg fracture, who would have been treated in the study institution but were non-residents, were excluded. However, there were no such cases. The number of included patients was analyzed annually, and the respective paediatric population-in-risk was obtained from the official statistics by Statistics Finland (http://www.stat.fi/index_en.html). The children (< 16 years) population-in-risk changed between 51 477 and 56 920 in the geographic study area during the study period. The number of eligible patients was 101 and they formed the study population. The potential changing trend in the incidence from the beginning to the end of the study period was evaluated in time periods of four years.
Primary radiographs of all patients were re-reviewed to confirm the radiographic type of the fracture. In this study, ‘trampoline leg fracture’ was determined as a transverse hairline impaction fracture of the tibiae with or without any fracture line upward towards the growth plate. The buckle and the fissure were evaluated. Intra-articular effusion of the knee and potential tilting of the secondary ossification centre and growth plate, usually in anterior direction, were measured. 23 The normal posterior tilting of a tibial plate was taken to be 3.1° during the measurement. 23 The preceding risk factors for the injury were recognized from the journal charts, when available, e.g. the use of a safety net, adult supervision and the number of simultaneous jumpers on the trampoline. Clinical symptoms and findings upon out-of-hospital admission were analyzed and the treatment was comprehensively reviewed from journal charts and operation charts, as appropriate. Radiographic bone healing, in particular endosteal bridging callus formation and fracture line consolidation, and potential short- or long-term complications were further analyzed.
Statistical analyis
Patient age and other continuous variables were described using mean, range and sd. Dichotomous variables were analyzed using frequencies and proportions. The differences between proportions of the variables were analyzed using the Standardized Nominate Deviation (SND) test, and the distribution of the variables using the chi-squared test or Fischer's exact test for small groups. The threshold of statistical significance was taken to be p < 0.05, requiring that all analyses were two-tailed and 95% confidential intervals (CIs) were used as possible. All statistical tests were performed using SPSS Statistical Software Package, version 24.0.0.1 (IBM, New York, USA) or StatsDirect Statistical Software, version 3.2.8 (Marlow, UK).
Results
Incidence
The mean annual incidence of the fractures was 15.4 per 100 000 children, aged < 16 years, during the 12 years of the study period. The annual incidence increased two-fold from 9.5 per 100 000 at the beginning of the study period (2006 to 2009) to 22.0 per 100 000 at the end of the study (2014 to 2017) (difference: 12.5; 95% CI 5.1 to 20.3 per 100 000; p = 0.0008) (Table 1).
The annual frequencies and population-in-risk of the study population, comprised of 101 patients with a proximal trampoline-related impaction fracture
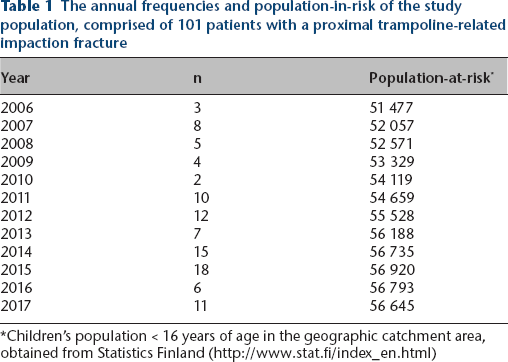
Children's population < 16 years of age in the geographic catchment area, obtained from Statistics Finland (http://www.stat.fi/index_en.html)
The fractures usually occurred in May (n = 35; 34.7%), followed by June (n = 20; 19.8%). Tuesday (n = 20; 19.8%) and Saturday (n = 18; 17.8%) were the week days during which the fractures most frequently occurred.
Patient characteristics
There were 101 patients with a trampoline leg fracture and of these, 56 (55.4%) were boys. The mean age of the patients was three years, ten months (sd 1.6 years; 1 to 12). Altogether 91% of the patients were at most five years of age. A slight majority, 54 fractures (53.5%) were on the left side.
Radiographic findings with admission
On admission, primary radiographs presented an isolated metaphyseal fracture in 85.9%, while the fracture line reached the growth plate in 11.8% (type 2 according to Salter-Harris classification) and 2.4% were interpreted as isolated growth plate injuries (Salter-Harris type 1). The buckle of the lateral cortices was evident in 65.7% of the cases and it was found in the anteroposterior (AP) projection of the plain films. The anterior buckle was seen in one in three (28.6%) cases in lateral projection. A concomitant proximal fibula fracture was found in two cases (Fig. 1).

The primary radiographs of the trampoline-related leg fractures were re-reviewed and different types of fractures were found, as shown in these three case examples:
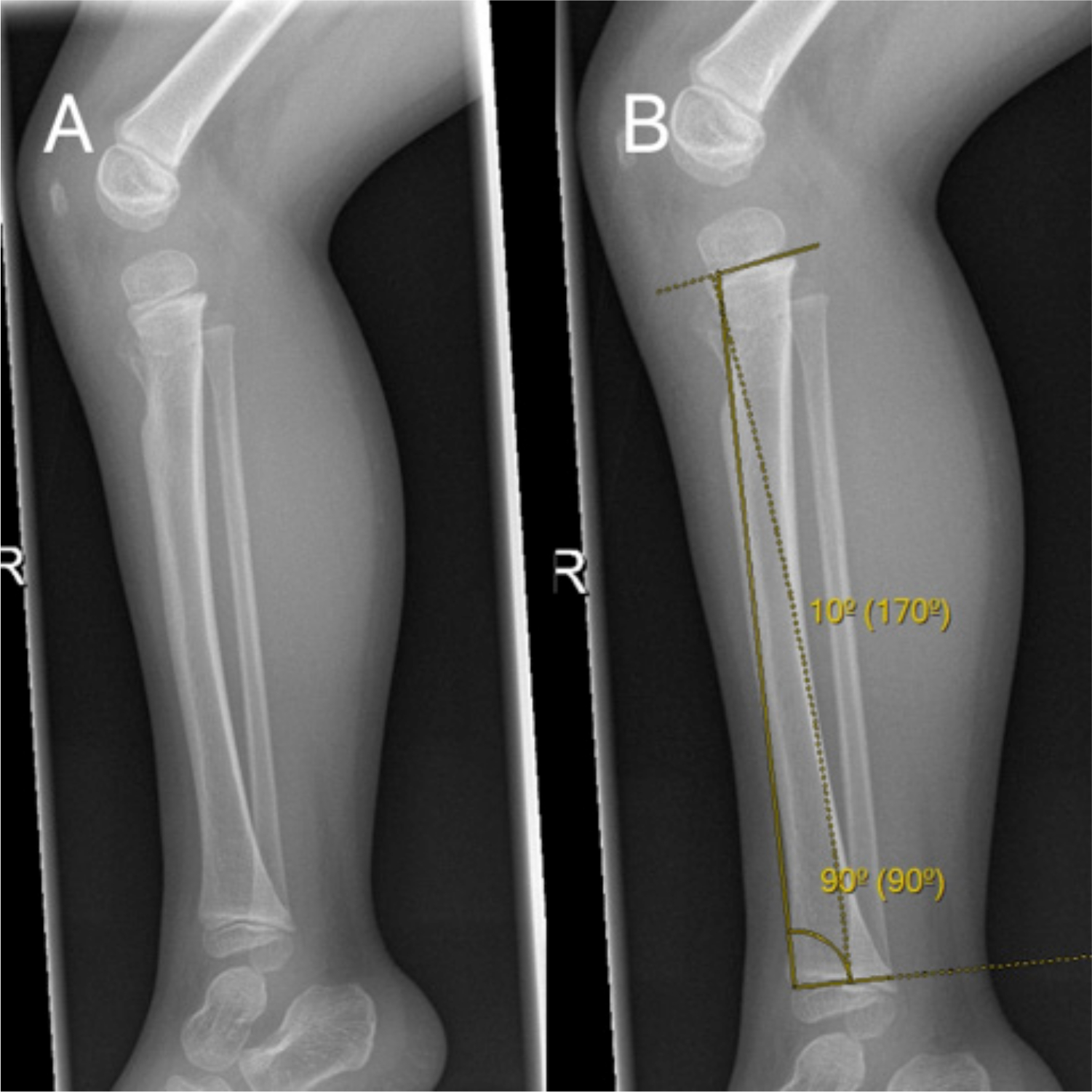
Anterior tilting of the proximal tibial growth plate was found in 68.3% of the cases (n = 69/101). Mean anterior angulation compared with the distal growth plate was 4.2° (sd 2.5°; 2.0° to 15.0°); thus, the mean deformation was 7.3° (SD 2.5°, 6.1° to 19.1°), given that normal posterior tilting of a tibial plate is 3.1° 23 (Fig. 2).
The patient had injured his right leg during trampoline jumping:
Risk factors
Four in five of the fractures (n = 48; 81.3%) occurred, when there was more than one child jumping simultaneously on the trampoline. The number of children jumping on the trampoline at the same time was registered in 59 patients. Seven injuries happened during parental supervision but the information about the adult supervision was only available in 22 cases. The information about the use of the safety net during the injury was not available from any.
Treatment and recovery
All patients but one were treated without surgery. In all, 90.1% (n = 91) were immobilized using the plaster of Paris or fibre-glass casting. The mean time of immobilization was 3.3 weeks (sd 0.8; 2 to 7). One patient treated with a cast needed a further closed re-reduction due to the worsening anterior angulation.
One patient was not examined afterwards but all other patients visited the out-of-hospital clinics for follow-up. In follow-up radiographs, good bone union with a visible callus formation in four out of four cortices was found in the majority (72.5%) of patient cases. Further, 20.2% of the cases had callus in three out of four cortices prior to the end of follow-up. Nine patients presented delayed recovery and received long-term follow-up, however, none of them required any later-stage treatment.
Discussion
The main finding of this population-based research was that the incidence of trampoline-related leg fractures of children has increased two-fold during the last decade. The patients were young with an average age of less than four years. Several children had commonly been jumping together. The great increase in the incidence is alarming but reasonable, as backyard trampolines in the area have become more popular. The explosive growth in the market for home trampolines for recreational use has been reported.24,25 Further, there is an increasing popularity in commercial trampoline parks.26,27 To our knowledge, there has been a very limited understanding of the current epidemiology of trampoline leg fractures, as more severe injuries have been the main focus of interest. Our research is the first to report the population-based annual incidences during the era of recreational home trampolines. In comparison, the recent increasing incidences of many trampoline-related upper extremity fractures such as forearm fractures are well known. 28
Of all the growth plates in children, the proximal tibiae physis is among the most vulnerable to damage and growth disturbance, in general. 29 Bearing this in mind, all bone fractures in the upper part of tibiae should be considered as clinically significant, and follow-up is recommended. 30 A particular fracture in this area is the ‘trampoline leg fracture’, which is an impaction fracture of the cortices caused by high landing force on an upward impacting trampoline mat. There are not usually any fissures that reach the physis, however, anterior depression of the physis is usual, resulting in the tilting of the growth plate. Sometimes slight anterior tilting of the growth plate can be the only sign of the fracture. Actually, anterior tilting was a particularly common finding in our cohort, with two out of three patients demonstrating an average 7.3° anterior angulation, compared with normal values in the literature. 23 Therefore, despite their usually slight clinical findings, these fractures should not be overlooked in clinics and the anterior tilting of the proximal tibial plate should always be recognized.
We found that fractures most usually occurred in spring (May), which agrees with the previous literature: physiological weakness of bones in that period may be associated with vitamin D deficiency and less physical activity in preceding winter months. 25 We also found that younger children were more prone to trampoline leg fractures than older children. This is completely in line with previous literature; Meyerber et al 8 reported that all trampoline-related tibiae fractures occurred in children younger than six years. One reason for this is that the injuries usually occur when more than one person is on the trampoline at the same time: when the kinetic energy of the heavier jumper transfers to the lighter jumper, a high impact force is generated, while the proximal part of the tibia is a characteristic point of injury. In fact, this trauma mechanism is highly particular to this injury: we found that 81.3% of the fractures occurred when several people were jumping on a trampoline at the same time. Correspondingly, it is justified to conclude that many of the trampoline leg fractures could be prevented by avoiding having multiple jumpers on the trampoline. This means that by following safety instructions that suggest only one jumper at a time, these potentially harmful fractures would no longer be so common.
This study was performed in a hospital district area that comprise both urban and rural areas. The epidemiological findings were certain in this subregion of Oulu Arc and Oulu and the enrollment was taken to be complete. The isolated fractures that would not have been recruited to this study are rare and they would not have changed our main conclusions. Radiographs of all included cases were available, and diagnoses were confirmed. The incidence was calculated annually based on the official children's population in the area and the trend was evaluated in satisfactorily long time periods. The home municipalities of all children at the time of the injury were reviewed and the isolated cases living out of the study area would have been excluded from the study population. Thus, finally, the changing trend of the incidence of fractures could be determined.
However, this study is subject to limitations. As the main weakness, this was a retrospective registry-based study and no long-term follow-up could be achieved with this study design. We were additionally interested in the potential long-term outcomes, but no such data was available. In this study, short-term outcomes were assessed based on the overall conclusions made by the treating physicians, but no significant complications were found. However, investigations were not performed similarly to all patients and no structural questionnaire was used, resulting in out-of-hospital follow-up of the individual study patients not being completely coherent between the patients. We appreciate that growth disturbances may not have become visible during a routine short follow-up and further prospective research with a longitudinal study setting is highly warranted in the future. At least several years following the injury would be required to exclude potential growth plate injuries. We in particular understand that the most harmful complication of the proximal tibiae fracture, the premature arrest of the nearest growth plate, would not have always been revealed during the short follow-up of the patients of this retrospective cohort. This, in turn, still warrants long-term follow-up research of both clinical and radiographical outcomes of trampoline leg fractures in the future, using standardized methods of imaging and clinical evaluation. As another weakness, radiographs of the contralateral, uninjured side were not available and the previously reported normal value of the proximal growth plate posterior tilting was, therefore, used as a reference in measuring.
Conclusion
Trampoline-related leg fractures have increased two-fold during the 12 years of this study period. This is an important finding, because these fractures may be associated with growth disturbance of the proximal metaphysis of the tibia. Probably many of these specific injuries could have been prevented by avoiding situations where more than one child jumps on the trampoline at the same time.
Footnotes
All other authors declare no conflict of interest.
LK: Interpretation, Writing and drafting.
SV: Interpretation, Writing and drafting.
WS: Design and drafting.
LL: Design, Writing and drafting.
JJS: Study design, Data acquisition, Analysis, Interpretation, Writing and revision of the manuscript.
Each author has approved the final version.