
Abstract
Objective
To investigate the relationship between child and adolescent obesity, and parental weight status.
Methods
Height and weight were measured in Chinese children and adolescents aged 6–17 years old. Information was collected concerning parental weight and height, and possible covariates, using a questionnaire. The body mass index (BMI) of each study participant and their parents was calculated. On the basis of the BMI, parents were categorized as normal, overweight or obese, and children and adolescents were categorized as normal or obese.
Results
Of the 5 041 participants included in the study, 6.82% were obese. Child or adolescent obesity was significantly associated with parental obesity. When both parents were obese, there was a 3.62-fold increased risk of obesity compared with those whose parents were of normal weight. Obesity in fathers was associated with a heightened risk of obesity in female children, whereas obesity in mothers was associated with a heightened risk of obesity in male children.
Conclusions
Parental obesity was a predictor of obesity in children and adolescents. It is therefore of key importance to prevent obesity in children who have one or more obese parents.
Introduction
Obesity among children and adolescents is a major public health problem that is growing in magnitude worldwide and which has reached epidemic proportions in recent years. 1 Although health problems associated with obesity are less common in childhood, children who continue to be overweight into adulthood are more likely to develop numerous associated complications, compared with children who continue to be of normal weight.2,3
As a key aspect of the family context, parental weight status has been shown to be an important predictor for the development of obesity in children and adolescents.4–6 However, the relative contribution of parental weight status is still controversial.
The present study was a large-scale cross-sectional epidemiological survey to investigate the potential relationship between parental weight status and obesity in children and adolescents (6–17 years old) residing in rural North China. Other potentially interacting or confounding sociological and demographic variables were also investigated.
Subjects and methods
Study population
Chinese children and adolescents (age range, 6–17 years) were recruited from 12 schools in rural areas of Shenyang, Liaoning Province, China, between July 2010 and January 2011.
Written informed consent was obtained from the parents or legal guardians of the participants. The study protocol was approved by the Committee on Human Experimentation of China Medical University, Shenyang, Liaoning, China.
Parental weight status
Information on the weight and height of each study participant’s mother and father was provided from a questionnaire completed by the parents. The body mass index (BMI) was calculated and was used to categorize parental weight status as normal (BMI < 24), overweight (24 ≤ BMI < 28) or obese (BMI ≥ 28). 7
Child and adolescent weight status
Height and body weight were measured by trained personnel using standard protocols; study participants were barefoot and wore only light underclothes. Height was measured using a portable stadiometer and was rounded to the nearest 0.5 cm. Body weight was measured using a professional scale and was rounded to the nearest 100 g.
Participants were categorized as obese or not obese, on the basis of the recommended cut-off values for the child or adolescent’s age and sex, as reported by Cole et al. 8
Covariates
Information concerning potentially interacting or confounding covariates was collected in the parental questionnaire, including the age, sex and race of the child or adolescent, the parents’ educational status and the number of people in the house. 9
Statistical analyses
The χ2-test was used to evaluate differences in the percentage of obese children and adolescents according to parental weight status. Logistic regression models, using parental weight status as the independent variable (model 1) and with added covariates of age, sex, parents’ education level, number of people in the house and ethnicity (model 2) were created; odds ratios for obesity in children or adolescents were calculated. In addition, the dependent variable in model 1 was adjusted for the sex of the child or adolescent. A P-value of <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 19 (SPSS Inc., Chicago, IL, USA).
Results
A total of 5 665 Chinese children and adolescents aged 6–17 years old were recruited to the study. The final study population consisted of 5 041 participants (2672 males; 2369 females), giving a response rate of 89%. The mean ± SD age of the male study participants was 10.92 ± 2.67 years and that of the female study participants was 10.88 ± 2.70. Participants with incomplete data were excluded from the study.
Parental weight status and child and adolescent obesity
Obesity in 5 041 Chinese children and adolescents (aged 6–17 years), according to parental weight status.
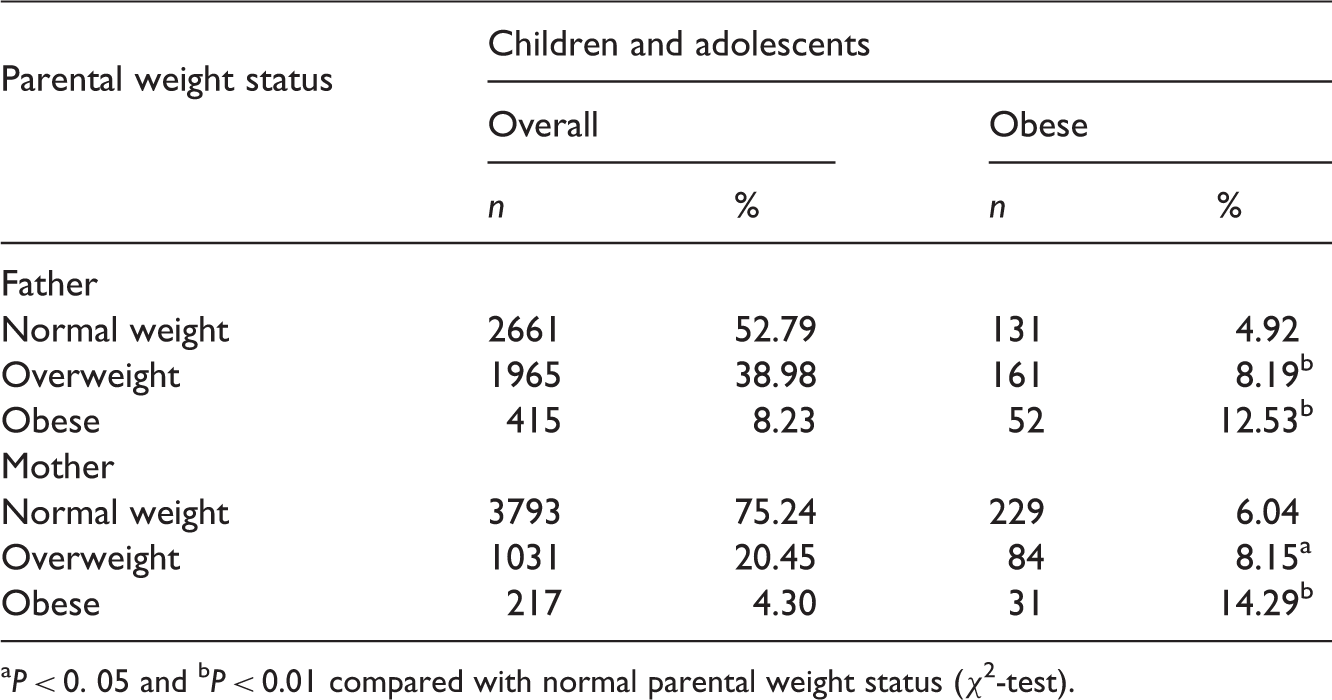
P < 0. 05 and bP < 0.01 compared with normal parental weight status (χ2-test).
Obesity in 5 041 Chinese children and adolescents according to the number of parents affected by obesity.
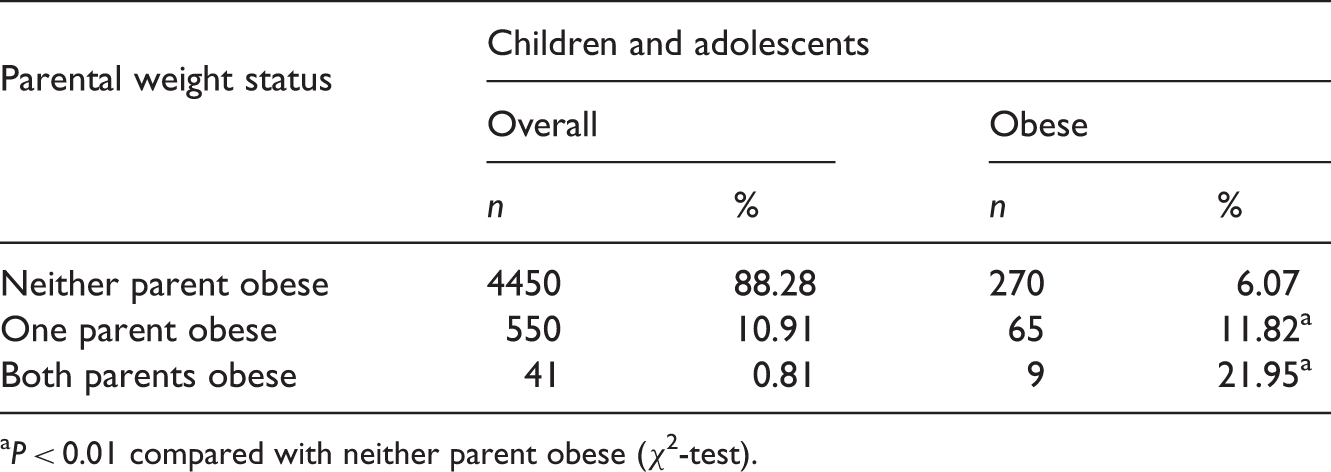
P < 0.01 compared with neither parent obese (χ2-test).
Logistic regression analyses of the association between parental obesity and child or adolescent obesity.

Independent variable was parental weight status.
Independent variables adjusted for parental weight status, parental education level, age, sex and race of child/adolescent, and number of people in the house.
CI, confidence interval.
Logistic regression analysis of the association between parental obesity and child or adolescent obesity adjusted for sex.

CI, confidence interval.
Discussion
In the present cross-sectional study, the overall child and adolescent obesity rate was high, at 6.82%, and was shown to increase significantly with increased parental weight status. The obesity rate in children and adolescents whose parents were both obese (21.95%) was 3.62 times the rate compared with children and adolescents whose parents were of normal weight (6.07%). Furthermore, the obesity rate of children and adolescents had a significant association with the obesity rate of their parents (P < 0.01). These results suggest that obesity in parents has an important influence on children’s BMI. Even unilateral obesity in parents was associated with an increase in child and adolescent obesity; however, maternal obesity was shown to be more of a risk factor than paternal obesity.
A number of studies have shown that childhood and adolescent obesity has an obvious familial aggregation, which is a result of the interaction of genetic and environmental factors.10–12 Obese parents, either through genes or sharing the same environment with children, can increase the risk of child or adolescent obesity. For young children, daily energy consumption depends to a large extent on their parents. In addition, children imitate others; thus, parental eating habits and lifestyle have a great influence on children’s behaviours. Unhealthy parental eating habits (such as the consumption of sweet, fried and fast foods), or bad lifestyle habits (such as lack of exercise and prolonged television watching) can lead to obesity in both themselves and their children.10–12
In the present study, maternal weight status had a stronger influence on obesity prevalence in children and adolescents than paternal weight status. This may be due to mothers being more involved with activities such as food choice and preparation. It has been reported that the diet of children is more similar to their mother’s diet than to their father’s diet.13–15 In the present study, obesity in male children or adolescents was more strongly correlated with maternal weight status than with paternal weight status. Conversely, obesity in female children or adolescents was more strongly correlated with paternal weight status than with maternal weight status. This suggests that obese fathers had a greater impact on their female children, whereas obese mothers had a greater effect on their male children.
Improvements in social environments, and changes to the type of food available, have been associated with obesity becoming a serious public health problem in many countries. Research shows that, although there are short-term consequences of adolescent obesity, 16 the greatest risk is related to the significant association with adult obesity. 17 Obese adolescents have a higher than normal risk of metabolic disorders, diabetes and hypertension, compared with adolescents of normal weight, and this risk increases as they develop into obese adults. 18 Early intervention and control of adolescent obesity could prevent adult obesity and its associated complications.
The use of BMI to assess parental weight status may be a limitation of the present study, as the BMI does not always reflect a person’s body fat percentage and does not take into account waistline circumference. According to the 2004 guidelines for the prevention and control of overweight and obesity in Chinese adults, 7 a BMI ≥ 24 is designated overweight and a BMI ≥ 28 is designated obese, but in addition a male waist circumference ≥85 cm or a female waist circumference ≥80 cm should be considered obese. 7
In conclusion, the present study demonstrated a significant association between child or adolescent obesity and parental obesity, showing that obesity in parents is an important risk factor for obesity in children or adolescents. The World Health Organization has repeatedly proposed that it is not sufficient to simply intervene in the lives of overweight or obese adolescents in order to reduce the adolescent obesity rate.19–21 The present study results suggest that overweight parents, or obese children or adolescents, should not be seen in isolation as the major target population for preventing obesity. Instead, children and adolescents and their parents should be encouraged to join together, to improve the eating habits and lifestyle of the entire family.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.