
Abstract
Back pain is a relatively common complaint in children and adolescents. The pediatric patient presenting with back pain can often be challenging, and there are many well-known organic diagnoses that should not be missed. In younger children, an organic cause of back pain can often be found. However, back pain in older children and adolescents is often “non-specific.” The differential diagnosis of back pain in children includes neoplasms, developmental, and inflammatory conditions. Basic steps should include an in-depth anamnesis, a systematic physical examination, and standard spine radiographs (anteroposterior and lateral). Nevertheless, advanced diagnostic imaging and laboratory studies should be included when indicated to avoid missing or delaying a serious diagnosis. If other types of imaging tests are necessary (magnetic resonance imaging, computed tomography, bone scan, or single photon emission computed tomography), they should be guided by diagnostic suspicion.
Keywords
In recent years, consultations for back pain in pediatric patients have become increasingly recurrent. 1 What was previously considered a rare condition that suggested a serious disease, usually due to an organic cause, has become a more frequent reason for consultation. Currently, scientific evidence suggests that it is not only organic disorders that give rise to these symptoms but that it is increasingly common at certain ages to find benign or idiopathic (“non-specific) causes for back pain. 2 Gathering relevant information during anamnesis and performing a complete physical examination is of great importance in these situations to determine the origin of the pain. If findings from the history and physical exam suggest an underlying pathology, simple imaging is initially indicated; advanced imaging techniques and laboratory studies may be needed for further evaluation in certain circumstances.
Introduction
Back pain is a relatively common complaint in children and adolescents; however, it is not as frequent as in the adult population. The literature suggests that significantly more children have back pain than the number who seek medical attention. Care is sought in less than one-third of cases, 3 making it difficult to calculate the exact prevalence. The reported annual incidence of back pain in adolescents ranges from 11.8% to 33%. 4 Kjaer et al. 3 found a prevalence of 28% to 48% in school-aged children, with increasing incidence in older adolescents. More than 50% of children experience some type of back pain by 15 years of age, 5 and up to 36% of school-age children suffer episodes of low back pain. 6 Sedentary lifestyle, obesity, and increased backpack weight are possibly related with a substantial increase of non-specific back pain in children and adolescents. 7
Until recently, children presenting with back pain were thought to usually have an organic origin for their pain. 6 Diligent investigation with extensive evaluation using imaging and lab work was recommended for every child who complained of back pain to avoid missing a possible underlying cause. 8 In younger children, an organic cause of back pain can often be found. However, back pain in older children and adolescents is often “non-specific.” 9
Back pain in children should be assessed carefully, yet most children will only require a detailed anamnesis, a thorough physical examination, and standard spine radiographic evaluation (anteroposterior (AP) and lateral) without the need for advanced imaging. 10 An accurate history and complete physical exam are key for establishing a definitive diagnosis of the cause of back pain in most cases. Both, anamnesis and physical examination, must be rigorous and systematic to obtain as much information as possible. Nevertheless, advanced diagnostic imaging and laboratory studies should be included when indicated to avoid missing or delaying a serious diagnosis.
Patient history
An in-depth, detailed anamnesis provides essential information when evaluating children with back pain. The patient history is often the most critical part of determining the etiology of the patient’s pain.
Biopsychosocial factors should be considered when gathering information. Family history of herniated disk, spondylolisthesis, or kyphosis should be documented. Patient’s level of activity should also be established, including any sports they participate in and frequency. It is important to assess the child’s baseline activity and degree of sport participation. Changes in activity or athletic participation require careful assessment. The examiner should ask both the patient and parents how the pain conditions the child’s daily activities.
Certain activities entail risks for injury. Adolescents who are involved in sports that require repetitive axial loading, extension, or twisting have higher rates of back pain.11,12 Competitive gymnasts have a relatively high incidence of spondylolisthesis.
In school-aged children recent illness, remote trauma history, non-accidental injuries or previous episodes of back pain should also be documented. Previous bacterial or viral infections may be the origin of discitis or vertebral osteomyelitis. The presence of back stiffness in the morning or a family history of rheumatologic disorders suggest spondyloarthropathy. 13 Back pain associated with pain in other joints relieved by non-steroid anti-inflammatory drugs (NSAIDs) can also be related to an underlying rheumatologic disorder.
Szita et al. 14 detected relationships between back pain and age >12 years, family history of back pain, spending >2 hours per day studying or watching television, an uncomfortable school desk, widespread pain, and sleep problems. Regarding “heavy weight” backpacks, evidence is mixed on their relationship with back pain. 15
Age
The cause of back pain is tremendously varied (Table 2) and changes with the age of the patient. In infants (<5 years old), there is a higher probability of back pain being caused by an infection or neoplasm. Hematologic malignancies should be considered in a young patient with back pain without a clear diagnosis. Non-accidental injuries should be ruled out in non-ambulatory patients with signs of a traumatic injury.
During childhood (5–10 years old), infectious disorders (vertebral osteomyelitis and discitis) should still be considered in the differential diagnosis of back pain. In this age group, possible neoplasms include leukemia, lymphoma, eosinophilic granuloma, neuroblastoma, and astrocytoma 16 with an increasing risk for bone neoplasms, such as osteoid osteoma, and osteoblastoma. Rheumatologic causes also present in this age range and should be taken into consideration if there is a strong family history.
In older children (>10 years old) and adolescents, trauma (acute fracture) or overuse syndromes (muscle strains and stress fractures), spondylolysis, spondylolisthesis, Scheuermann kyphosis, herniated disk, or slipped vertebral apophysis are more probable causes of back pain. Scheuermann kyphosis is the most common cause of thoracic back pain in teenagers. Spondylolysis and spondylolisthesis are the most common causes of “organic” lumbar back pain in adolescents. 17 However, infectious, neoplasms, and rheumatologic causes remain in the differential diagnosis in this age group. Osteoblastoma, osteosarcoma, and lymphoma occur in these older ages.
Pain characteristics
Anamnesis should include questions regarding nature, timing (onset, duration, and frequency), location (including radiation to the extremities), and severity of pain. Factors that aggravate or relieve the pain should also be documented.
Nature. The examiner should ask if the pain is sharp or dull. Short-term mild pain after practicing sports is usually caused by muscle strain.
Onset/duration/frequency. The clinician should establish if the onset of pain was sudden or gradual. Acute pain (<24 hours) after a previous trauma event suggests structural injuries, such as fractures, sprains, herniated disks, or slipped vertebral apophysis. Slow-onset, long-lasting pain is usually associated to low back strain, Scheuermann kyphosis, and tumors. The examiner should also question about the duration of pain (weeks, months, or years). It is also relevant to establish if the pain is constant or intermittent. Persistent, unremitting pain and night pain are more likely due to tumors and infections. It is important to determine pain frequency (every day, week, and month). The relation with physical activity should also be documented. Recurrent pain associated with specific activities is more likely to be caused by spondylolysis, spondylolisthesis, Scheuermann kyphosis, or a herniated disk. Patients should be specifically asked about night-time back pain because this is indicative of certain etiologies. Night pain is a significant symptom to identify. A child who wakes in the middle of the night with pain and is unable to return to sleep suggests a neoplastic or inflammatory condition.
Location/radiation. The examiner should ask about distribution (lower back, thoracolumbar region, or thoracic area) and radiation of the pain. Localized back pain may be caused by spondylolysis or tumors. Pain in the lumbar region is associated with spondylolysis, whereas thoracic pain may be caused by Scheuermann kyphosis. Pain that radiates to the buttocks and/or posterolateral aspect of the thigh and leg suggests a lumbosacral level lesion and may indicate a lumbar disk herniation, slipped vertebral apophysis, epidural abscess, or intraspinal tumor. 10 Pain that radiates to the front of the abdomen, suggests a thoracolumbar level lesion; and to the front of the chest, a thoracic level lesion. Inflammatory processes and overuse syndromes usually result in a more diffuse or generalized pain that is felt over a wide anatomic area. 10
Severity. It is crucial for the clinician to establish if the pain is severe, moderate, or mild. It is also relevant to determine if the pain is severe enough to force the patient to rest or even miss school. A child who self-limits enjoyable activities because of pain requires a thorough evaluation.
Aggravation/Alleviation. The examiner should ask about factors that increase or relieve the pain. Alleviating and aggravating factors must be addressed specifically. The relationship of pain with a certain activity is relevant. Sport activities that entail repetitive hyperextension of the lumbar spine place shear forces across the vertebrae and increase the risk of spondylolysis and spondylolisthesis. 10 Frequent participation at a high level of intensity in sports activity can cause stress fractures or overuse syndromes. 18 Rest usually alleviates pain caused by spondylolysis, spondylolisthesis, Scheuermann kyphosis, muscle strain, or overuse syndromes. The examiner should question if the pain is aggravated by coughing, sneezing, or Valsalva maneuver. It is important to establish if the pain responds to NSAIDs. Pain promptly relieved by NSAIDs may be related to an osteoid osteoma. Back pain caused by spinal neoplasms is persistent and progressive and does not change with activity; pain may be worse at night when the patient is supine and is not relieved by rest.
Coexisting symptoms
Patients should be questioned about neurologic symptoms, such as numbness, weakness, or gait abnormalities. These symptoms must be carefully documented, as they are uncommon in benign conditions in children. 16 Particular attention should be given to numbness felt over the medial aspects of the legs or loss of bowel/bladder function because these are indicative of cauda equina and conus medullaris syndromes.
Similarly, it is important to note constitutional symptoms of weight loss, fever, chills, lethargy, malaise, or anorexia as back pain may be a sign of systemic malignancy or infection.
Anamnesis should finally include a general review of systems (neurologic, gastrointestinal, dermatologic, genitourinary, and psychiatric) to ensure that the patient does not have other medical issues known to have comorbidity with back pain.
Physical examination
For an adequate physical examination, the patient should undress completely except for underwear. Socks need to be removed so feet can be examined.
Evaluation of a child complaining of back pain will slightly differ based on his or her age. Physical exam is challenging in young children, so managing environment, tone of voice, and examiner-patient interaction is particularly relevant. At these younger ages, it is important to look for subtle clues that may reveal discomfort localized in their back. In this age group, examination of posture and gait assessment is extremely useful. Palpation and other specific tests will be performed as the last step as it may stress the child.
In older children, a systematic and protocolized examination is crucial. The examiner should start the physical exam by observing the patient’s gait, general body build, posture, and movement. The spine examination will include inspection, palpation, and range of motion (ROM). Combined with a thorough neurologic examination and specific orthopedics tests all will offer the clinician the best chance to objectively identify a cause for pain.
Gait assessment
Gait assessment should include heel and toe walking, and single-leg stance and hop. This allows the examiner to gather information regarding lower limb strength, balance, and coordination, and may assist in establishing the mechanism of onset of lumbar pain. Subtle changes in gait may reflect an underlying neurologic disorder. Children with discitis may refuse to walk. The examiner should look for claw toes, foot deformities, Trendelenburg gait, and muscle atrophy of calves or thighs. Spasticity, ataxia, and instability suggest spinal cord pathology or muscular dystrophy.
Visual inspection
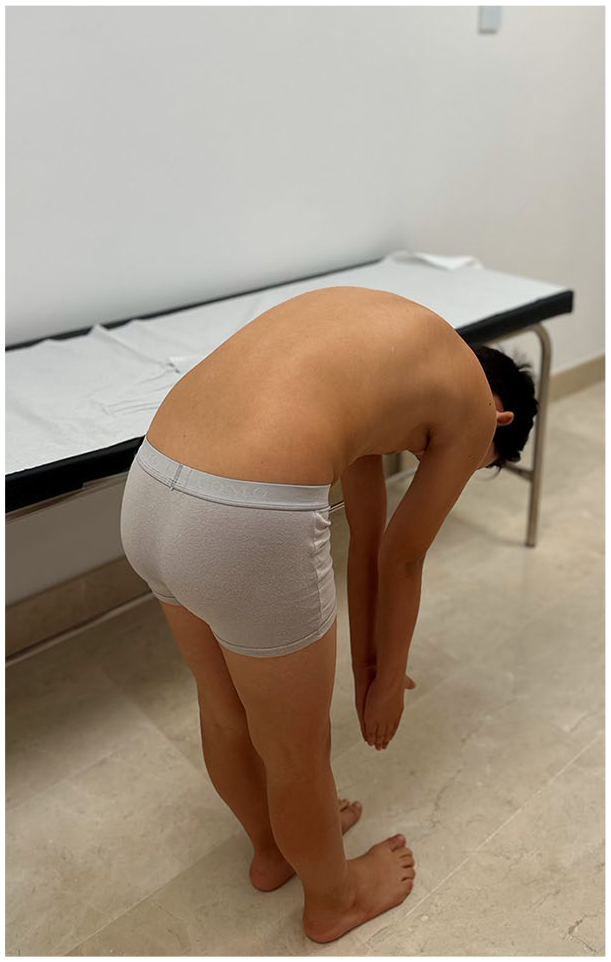
The next step is visual inspection of the back, standing posture and spine alignment. The examiner should inspect the patient from the back, front and side with the patient standing and then bending forward (Adam’s test). A forward bending test is helpful to evaluate the patient for deformities, such as kyphosis and scoliosis (Figure 1).

A forward bend test is helpful to evaluate the patient for spine deformities, such as scoliosis and kyphosis.
Inspection should include an evaluation of the patient’s spinal curvatures in the sagittal plane, judging thoracic kyphosis and lumbar lordosis. Hypokyphosis may suggest scoliosis, whereas hyperkyphosis may indicate Scheuermann disease. The examiner should assess shoulder, scapular, and pelvis level (iliac crests and superior iliac spines) and flank symmetry. The patient should be assessed for pelvic obliquity in the standing position. Leg length discrepancies <2 cm is considered normal and usually not symptomatic. 19 Any rotation of the vertebrae (rib or lumbar paravertebral hump) should be documented. Spine compensation should as well be evaluated in the coronal and sagittal plane. Trunk shift may indicate an underlying pathologic process, such as a disk herniation or neoplasm.
Range of motion
Following visual inspection of the spine, the examiner should assess its ROM and flexibility in flexion-extension, side bending, and rotation. Usually, ROM is measured actively, paying attention to which movements reproduce the patient’s symptoms. Stiffness or leaning over during this exam is highly suggestive of an underlying cause for back pain. Pain as the patient flexes (Figure 2) indicates either a problem in the anterior elements of the spine (vertebral body and intervertebral disk) or pain due to low back soft tissues (muscles, ligaments, fascia). Pain with extension (Figure 3) is more common when the problem is related with spine posterior elements (facet joints, pedicles, and spinous processes). With side bending and trunk rotation, pain on the same side suggests a bone-related problem. A child with discitis will bend his or her knees, rather than bend over at the spine, to pick up an object from the floor.
The examiner should assess the range of motion of the spine in flexion documenting pain, stiffness, leaning over, or inability to touch the floor with the fingers without bending the knees.
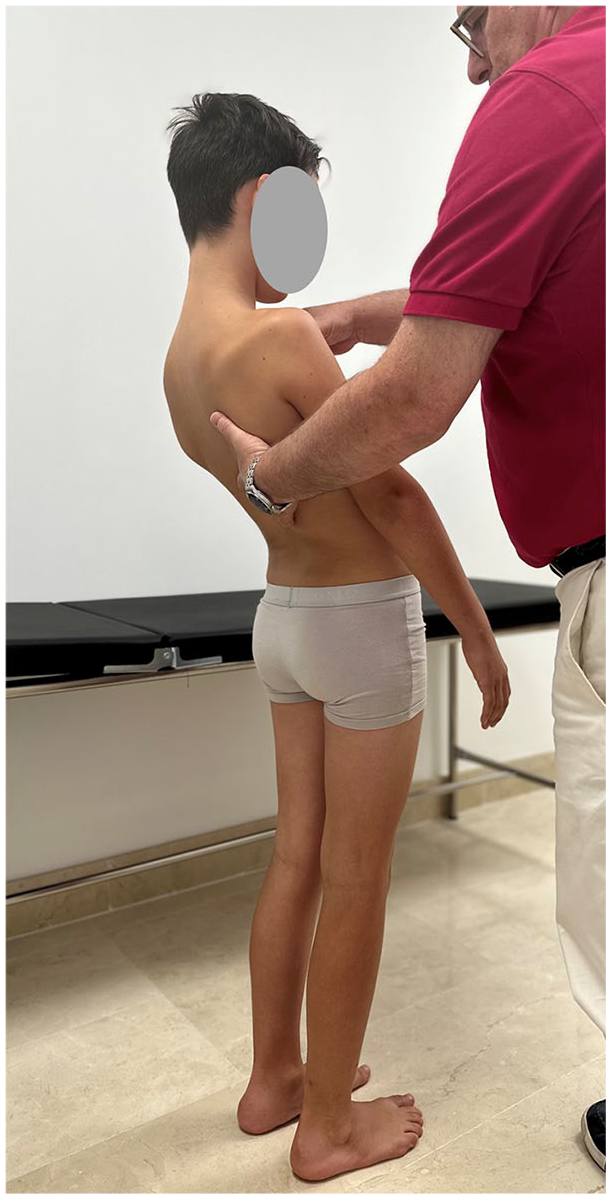
The examiner should assess the range of motion of the spine in extension documenting pain and stiffness.
Finally, it is also important to evaluate the ROM of the hips, knees, ankles, and feet. The examiner should rule out hamstring tightness as it is a known cause of spine mechanics disturbance. Hamstring tightness may be detected as inability to touch the floor with the fingers without bending the knees or an increased popliteal angle (Figure 4). Normal values for this angle are <30°. Inflexibility is associated with spondylolysis and typically worsens as children progress to adolescence20,21 leading to increased thoracic kyphosis.

Hamstring tightness may be detected as an increased popliteal angle.
Hip flexor tightness can be assessed with the Thomas test. With the patient supine, the examiner brings one knee to the chest. The test is positive if the contralateral leg lifts off the table.
Palpation
Next, the examiner should proceed with careful palpation of the entire spine and trunk musculature. Palpation is helpful to further delimitate the patient’s pain. The back should be palpated for midline, paraspinal and/or sacroiliac joint tenderness, muscle contractures, palpable masses, and anatomic irregularities, such as a step-off in the posterior elements. Examination should be performed with the patient standing on both legs and then on one leg at a time.
Beginning with soft tissues, the clinician should palpate the paraspinal muscles for signs of spasm (prominent and rigid muscle). Marked paravertebral muscle spasm reduces physiologic lordosis. Afterwards, the examiner should gently palpate the supraspinous and interspinous ligaments looking for tenderness. Next, the examiner should feel the bones. The spinous processes should be palpated looking for local tenderness, enlargement, or step-offs. Palpation of the spinous processes may elicit tenderness in children with spondylolysis, malignancy, or infection. Spinous process enlargement may indicate the existence of aneurysmal bone cyst or osteoblastoma. Any step-off between L5-S1 or L4-L5 spinous process suggests spondylolisthesis. A defect between the lamina suggests spina bifida. The examiner should then gently press over the facet joints and the transverse processes laterally. Following, the posterior aspect of the sacrum, sacrococcygeal region, posterior iliac spine, sacroiliac joints, and iliac crests should be felt. Pain at the iliac crest may occur with apophysitis. 22 Next, the clinician should palpate the greater sciatic notch and the sciatic nerve. The examiner should afterwards perform a pelvic compression test by pushing the iliac bones toward each other with the palms of the hands.
Finally, the abdomen, inguinal area, and symphysis pubis should be palpated. As renal pathology can cause low back pain, palpation and percussion of the kidney region should be performed.
Skin abnormalities
The patient’s back should be inspected for midline skin abnormalities that may indicate intraspinal malformations. Midline cutaneous defects (dimples, sinuses, hemangiomas, lipomas, or hair patches), suggest underlying congenital spinal lesions. If the examiner observes 5 or more café-au-lait spots, neurofibromatosis should be ruled out and the patient referred to neuropediatrics, ophthalmology, and dermatology to screen for the disease. Midline skin cysts may indicate spinal cord abnormalities or dysraphism. Other skin signs include eczema, which can be related to arthritis, and bluish coloration in the lumbosacral area, which can be sign of spinal dysraphism.
Neurologic assessment
Next, a thorough neurologic assessment should be performed in all patients. A complete neurologic examination is essential and should include evaluation of motor and sensory function, deep tendon and abdominal reflexes, and upper motor neuron signs.
Strength testing of the hips, knees, and ankles may detect weakness related to pain or neuropathy. The examiner should establish motor strength according to neurologic level. Strength of L2-S2 nerve roots: The examiner will assess strength by asking the patient to flex and extend hips, knees, and ankles, as well as invert and evert the feet. (a) S1-S2 levels: Peroneus longus and brevis (S1), gastrocnemius-soleus (S1-S2); (b) L5 level: Extensor hallucis longus and extensor digitorum longus and brevis; (c) L4 level: Tibialis anterior; (d) T12, L1, L2, and L3 levels: Iliopsoas.
Sensitivity can be evaluated with test sensation to touch and pinprick according to the neurologic level. Sensation should be tested through all lumbar and sacral dermatomes. Dermatomal numbness and paresthesias suggest a nerve root lesion. (a) S1 level: Determine sensation on the plantar and lateral sides of the foot and over the lateral malleolus; (b) L5 level: Test sensation on the dorsum of the foot and lateral aspect of the leg; (c) L4 level: Test sensation on the medial aspect of the thigh; (d) L1-L3 levels: Anterior aspect of the thigh (L3-above the knee, L4-middle two-thirds of the thigh, and L2 just below the inguinal ligament).
Afterwards, the deep tendon reflexes should be tested. The Achilles tendon reflex or ankle jerk determines status of S1, whereas the patellar tendon reflex or knee jerk is a function of L4.
Next, the abdominal reflexes should be performed. The superficial abdominal reflex is tested by stimulating each quadrant of the abdomen with a sharp object. The umbilicus moves toward the side being stimulated (Figure 5). The lower abdomen is innervated by T10 to L4 and the upper abdomen by T7 to T10.
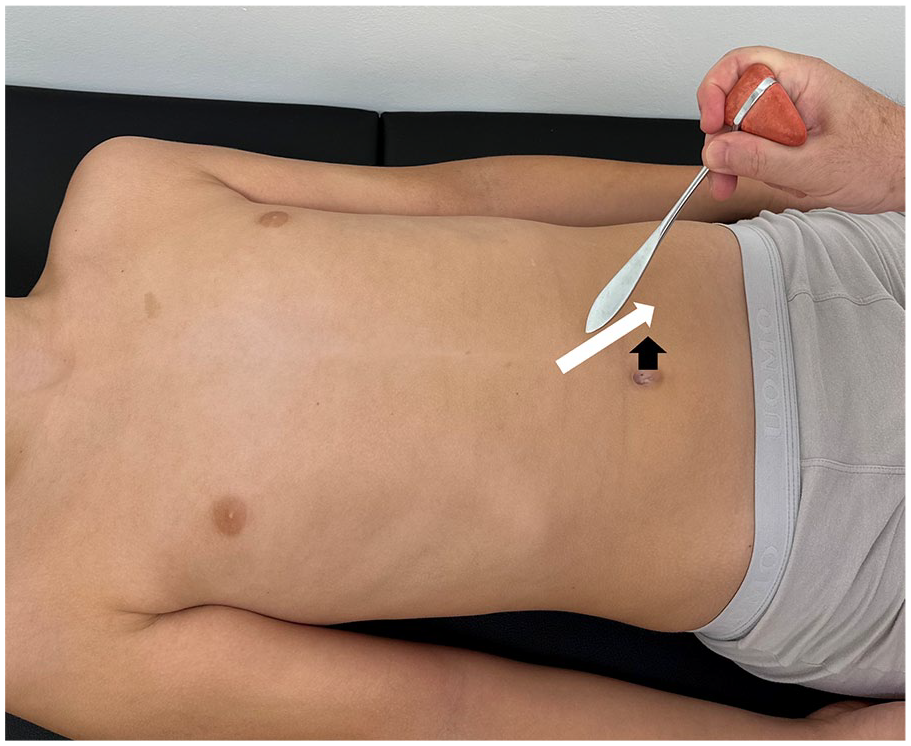
The superficial abdominal reflex is tested stimulating each quadrant of the abdomen with a sharp object.
The Babinski test is useful to evaluate for upper motor neuron injury.
Specific orthopedic tests
Several tests should be performed to guide our diagnosis toward more specific conditions.
Slump test
The patient is seated on the exam table with hands placed behind the back and legs hanging. The patient is asked to flex the spine into a slumped position (curve their spine into a global kyphosis). Reached this position, the examiner passively flexes the patient’s neck, placing the chin close to the chest. The patient’s leg is then actively extended at the knee. Last, the patient’s ankle is actively dorsiflexed (Figure 6). A positive test is elicited pain with any of the provocative maneuvers and suggests neural tension as the cause of patient’s back pain.

Slump test: the patient is seated on the exam table with hands placed behind the back and legs hanging.
Straight leg raise test
The patient is placed in the supine position with both legs completely extended. The patient’s leg should passively be raised 20°–30°, while maintaining extension of the knee. When the test is positive, it reproduces back pain with or without radiation to the posterior thigh or distally to the leg and foot. A positive test suggests a neurologic cause of patient’s back pain.
The slump test and straight leg raise test evaluate for sciatica; pain radiating to the gluteal area or down the leg indicate a positive test. The slump test is considered more sensitive than the straight leg raise test.
Schober test (modified)
The patient stands with the back to the examiner. The spinous process of the L5 vertebrae is identified and marked. A mark is made 5-cm inferior and 10-cm superior to this vertebra. The patient then bends forward to touch the floor with his fingers. The distance between the upper and lower points is measured while in complete flexion. A <5 cm increase between the upper and lower points is considered a positive examination. A positive test indicates decreased flexion ROM of the lumbar vertebral bodies and suggests ankylosing spondylitis.
Stork test
This test is performed with the patient in a one-legged stance with the other leg flexed at the knee. The patient is then asked to extend the lumbar spine (Figure 7). It should be repeated with the other limb. A positive test occurs when there is ipsilateral or bilateral lumbar back pain. A positive test suggests an injury to the posterior elements of the spine, in particular, the pars interarticularis (spondylolysis), although the sensitivity and specificity are low. 20

Stork test: this test is performed with the patient in a one-legged stance with the other leg flexed at the knee.
FABER test
This test is performed to determine sacroiliac pathology. The patient is placed supine with one leg flexed, abducted, and externally rotated, with the heel placed on the contralateral knee. The other lower limb remains extended. The examiner then uses a gentle force to place the leg further into external rotation and abduction. A positive test is pain elicited in the back or groin. Pain reproduced in the back is indicative of pain from the sacroiliac joint. Pain in the groin is suggestive of intra-articular hip pathology.
General physical assessment
Finally, a general physical examination is performed to rule out non-orthopedic conditions, which may cause back pain: urinary, gynecologic, cardiac, pulmonary, and gastrointestinal disorders.
Potential “
Imaging
The anamnesis and physical examination findings should guide the clinician to which diagnostic studies are appropriate (Figures 8–15).
Lateral lumbar spine radiograph suggests L4 spondylolysis.
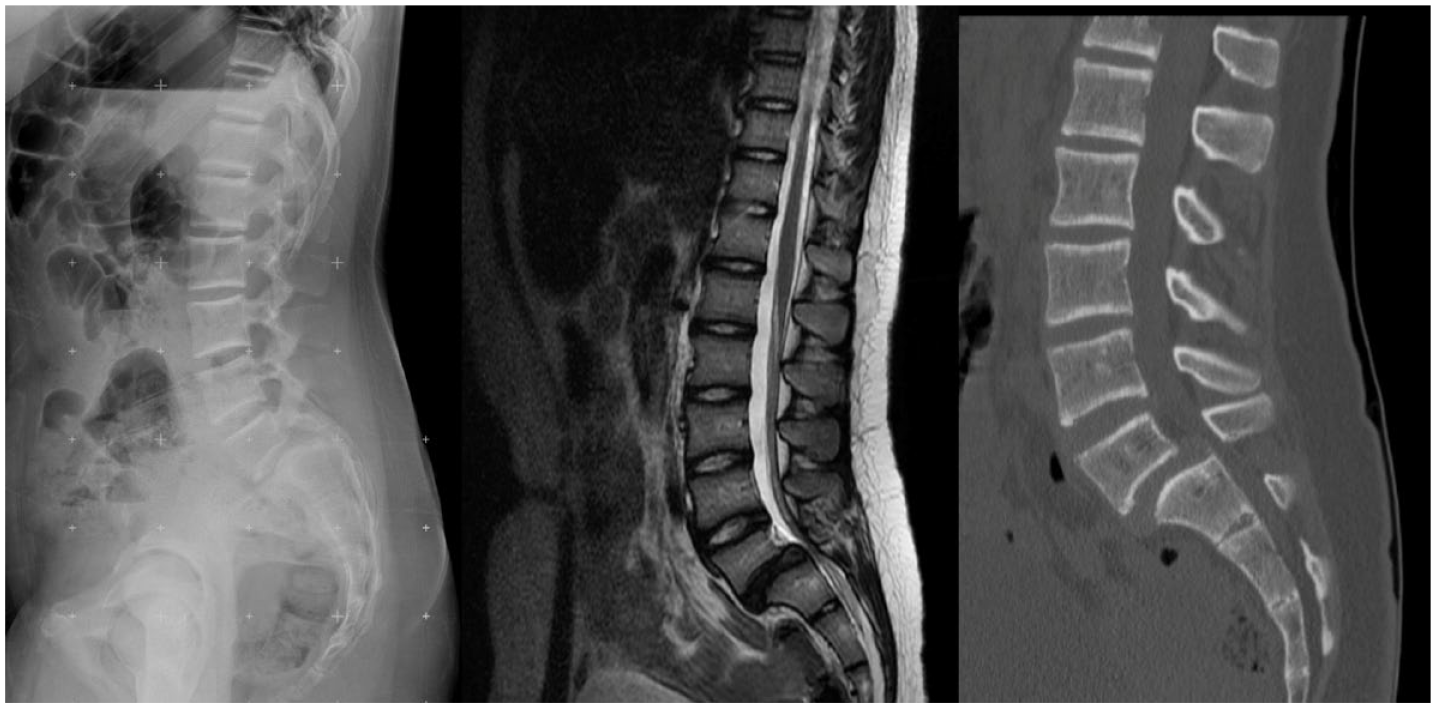
Lateral complete spine radiograph showing L5-S1 grade 2 spondylolisthesis.
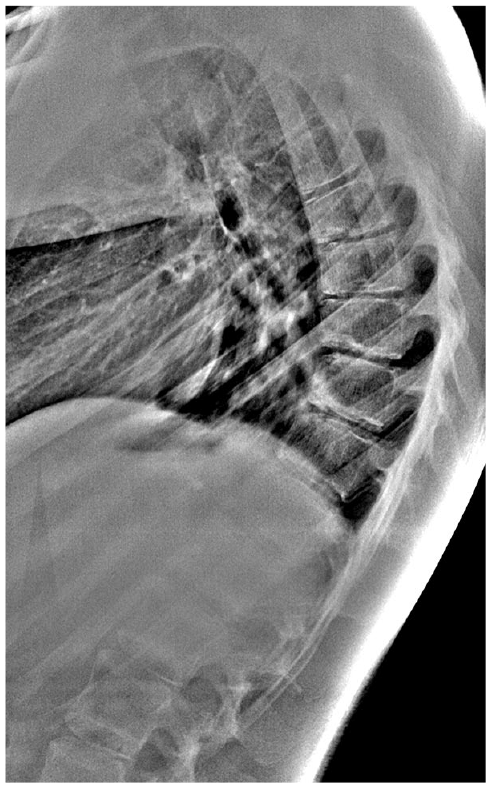
Lateral thoracic spine radiograph showing Scheuermann kyphosis criteria (three or more consecutive vertebrae wedged >5°).
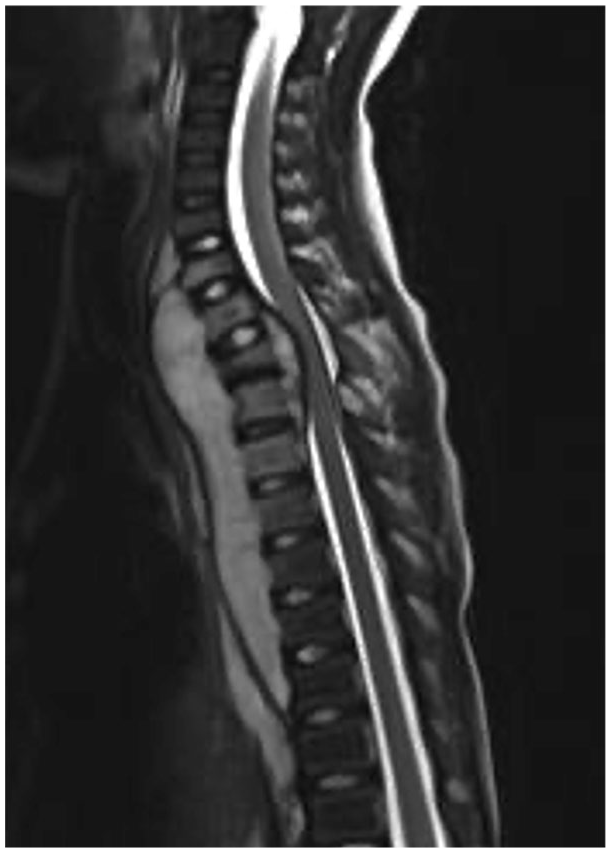
MRI image of vertebral osteomyelitis.
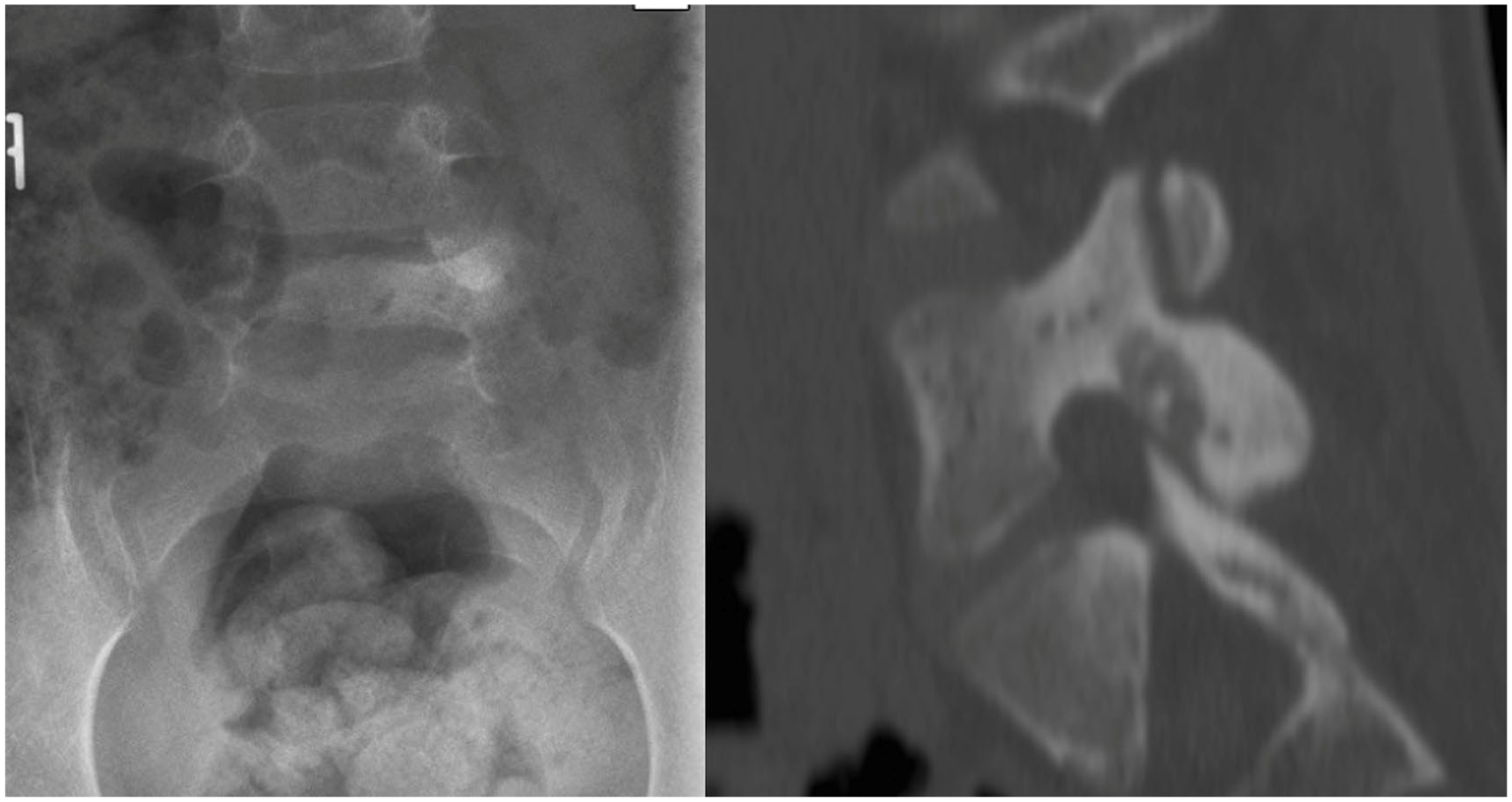
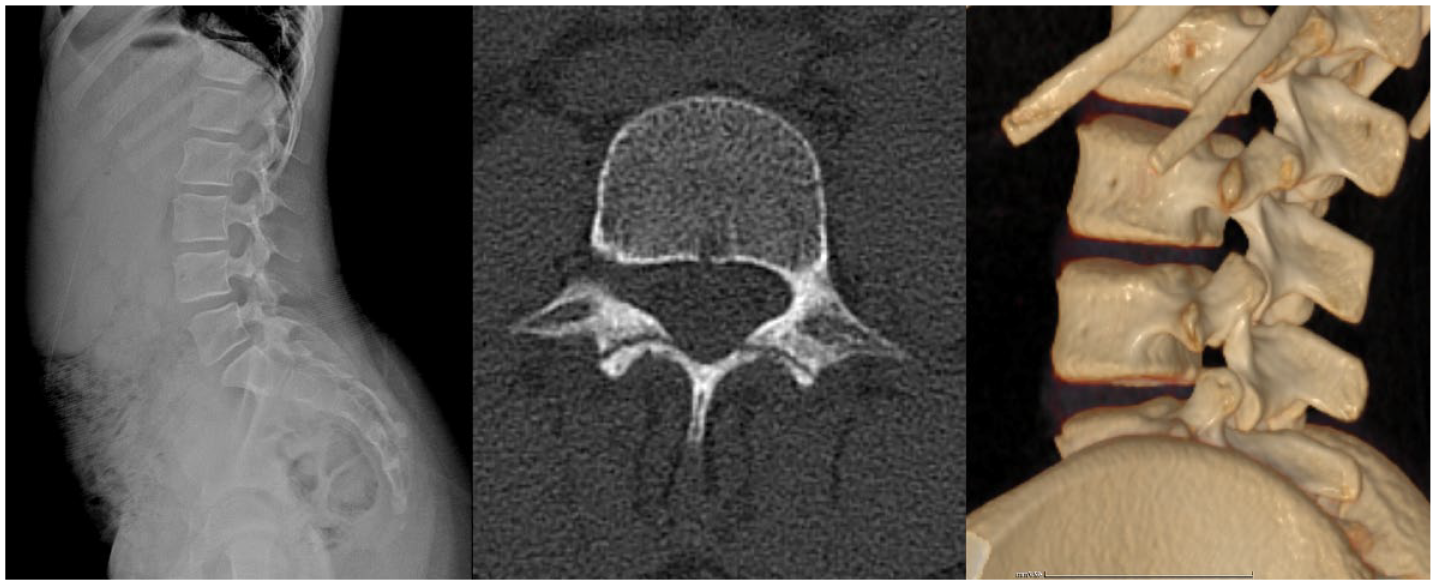
Standard lumbar AP radiograph showing an osteoid osteoma located in the posterior elements of L5.
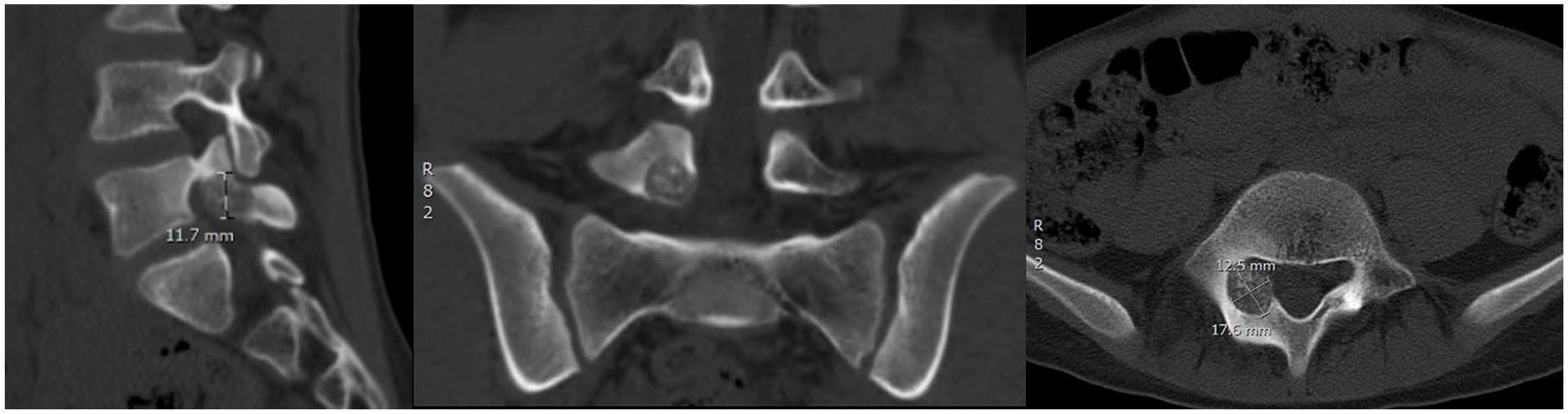
CT scan image of osteoblastoma located in posterior elements of L5.
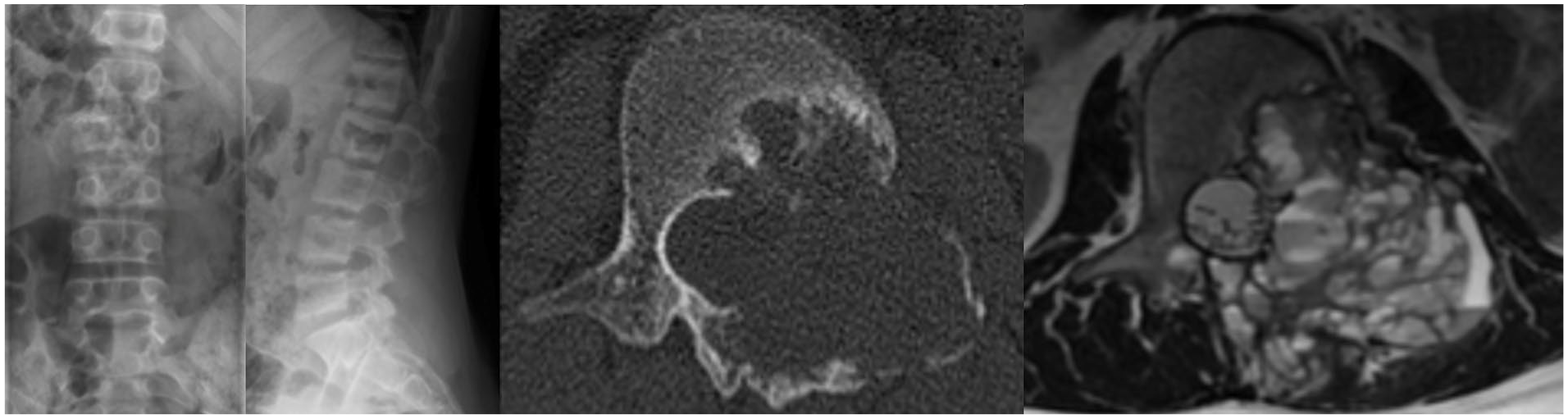
Standard spine radiograph showing “blow-out” radiolucent lesion, outlined by a shell of new periosteal bone formation compatible with aneurysmal bone cyst.
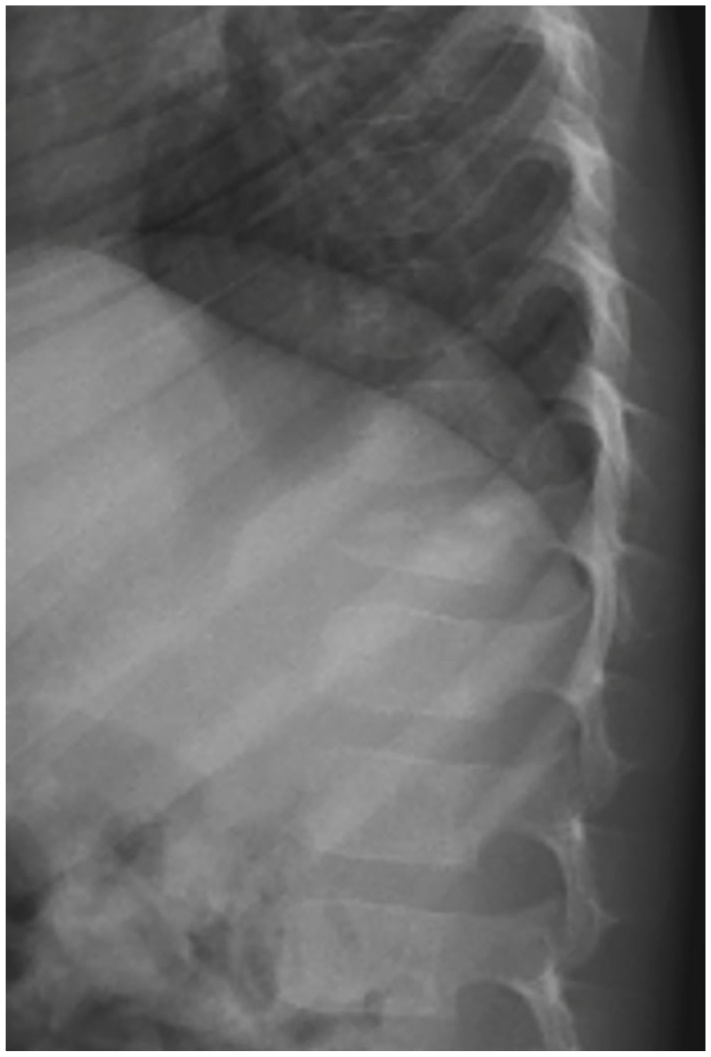
Standard lateral spine radiograph showing eosinophilic granuloma in T11 causing partial vertebral body collapse.
Radiographic evaluation
Radiographic evaluation should begin with standard standing AP and lateral views of the spine. AP and lateral views are often sufficient and seem to be the best diagnostic screening test for children with back pain, even when considering spondylolysis. 24 According to the American College of Radiology, imaging in children and adolescents may be delayed unless the patient has abnormal neurologic findings or pain that occurs at night, radiates, or persists >4 weeks. 25 Ramirez et al. 26 indicated an abnormal neurological examination as a strong predictor for an underlying pathologic condition. Standard radiographs should also be considered for all children <4 years of age with back pain or when the child has coexisting constitutional symptoms. Simple radiographs allow to observe vertebral alignment, narrowing of intervertebral disks, vertebral endplate irregularities, vertebral scalloping, lytic or blastic lesions, as well as stress-related injuries or reactions in relation to the sacroiliac joint. Oblique views classically indicated for detecting spondylolysis double the radiation exposure and do not significantly improve sensitivity, and currently are not recommended. 27 Feldman et al. 28 communicated an algorithm for evaluation of pediatric back pain. Advanced imaging was indicated for patients with abnormal plain films, constant pain, night pain, radicular pain, or an abnormal neurologic examination. The finding of scoliosis requires in-depth examination of the apex of the curvature on the convex side that may reveal a bony lesion, with the spine deviating away from the irritating process. 10
When standard radiographs do not lead to a certain diagnosis, advanced imaging tests should be requested.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is useful for patients with neurologic signs or symptoms when soft tissue lesions are suspected, or for persistent pain despite appropriate treatment. MRI is extremely helpful in diagnosing spinal cord tumors, syringomyelia, tethered cord, and disk herniations. It is indicated in cases of localized pain, even when no findings are seen in standard radiographs. MRI allows to differentiate soft tissue lesions, which cannot be evaluated through standard radiographs. Besides, it can be useful in cases where pain is related to tumors, infections, disk lesions, or can assess for edema in the pars interarticularis, which is consistent with acute spondylolysis.26,27
Computed tomography
Computed tomography (CT) is useful to more precisely define bone pathology (tumors or fractures) previously detected in standard spine radiographs or other imaging tests. CT shows bony architecture and soft tissues but unfortunately does not show marrow elements. It is not considered as a spine screening tool, even though it provides the best images of bone structures. CT can be performed rapidly and usually does not require sedation, but it may expose children to significant ionizing radiation. 29
Bone scan
Bone scan is uncommonly indicated nowadays although is a useful tool if MRI findings are inconclusive or in children with diffuse (non-localized) and persistent back pain. Bone scan is very sensitive in detecting pathologic conditions affecting bone metabolism (infection, benign and malignant tumors, and stress fractures). These lesions appear as areas of increased uptake of the radioactive material. However, bone scans lack specificity in establishing the precise nature of a lesion. Bone scans also are useful assessing the healing capacity of established lesions, as spondylolysis or stress fractures. Unfortunately, bone scans cannot detect lesions that do not stimulate bone metabolism and therefore may miss serious conditions as tumors or infections.
Single photon emission CT
Single photon emission computed tomography (SPECT) may be indicated when bone scans are non-diagnostic or equivocal. 10 SPECT has shown an increased sensitivity in assessing diseases affecting the lumbar spine compared to traditional bone scans. 30 SPECT is also a more precise imaging test for diagnosing spondylolysis and stress fractures in the lumbar spine compared to CT. 31
Lab work
Laboratory tests are indicated in all young children (<5 years) with back pain, especially if long-lasting, patients with night-time pain, and any child with coexisting constitutional symptoms. In these cases, a complete blood count (CBC) with differential and peripheral smear, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) should be obtained initially, even though CRP-specific value in patients with back pain has not been established. Conditions as infections, lymphomas, leukemia, and inflammatory disorders can be diagnosed. Although an increased ESR (>20 mm per hour) and/or CRP level (>1–2 mg per dL) is nearly 95% sensitive for osteomyelitis, the specificity is low (60%). 32 If a rheumatologic disorder is suspected, an evaluation by a pediatric rheumatologist should be warranted. The clinician should be cautious ordering rheumatologic specific tests, as their sensitivity and specificity are relatively low. 10 The presence of HLA-B27 is strongly associated with seronegative spondyloarthropathy (ankylosing spondylitis, reactive arthritis, and spondylitis associated with psoriasis and inflammatory bowel disease), but because of high false-positive rates, testing should be reserved for highly suspicious patients (morning stiffness, night pain, or sacroiliac pain). Axial spondyloarthropathy should be considered if clinical symptoms occur and MRI findings are negative; this condition is associated with elevated ESR and/or CRP levels in approximately 40% of cases. 33
Differential diagnosis
The differential diagnosis of back pain in children, in contrast to adults, more often includes neoplasms, developmental, and inflammatory conditions (Table 1). An accurate history, thorough physical examination, appropriate imaging techniques and specific lab work will guide the clinician to establish a definitive diagnosis of the cause of back pain in most cases (Table 2).
Most frequent causes of back pain in children and adolescents.
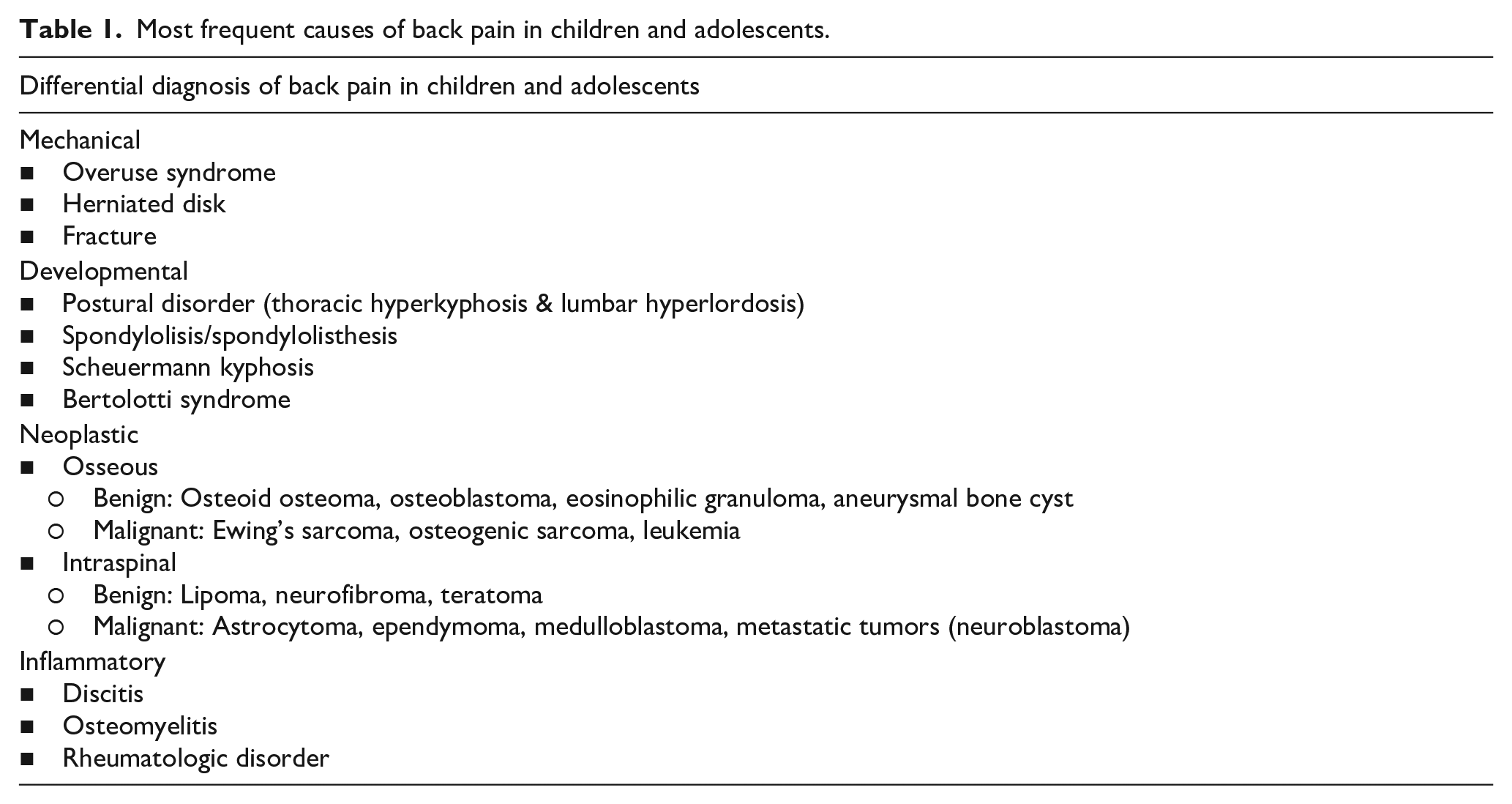
Characteristics (origin/epidemiology, anamnesis, physical examination, and imaging/lab work) of most conditions causing back pain in children and adolescents.
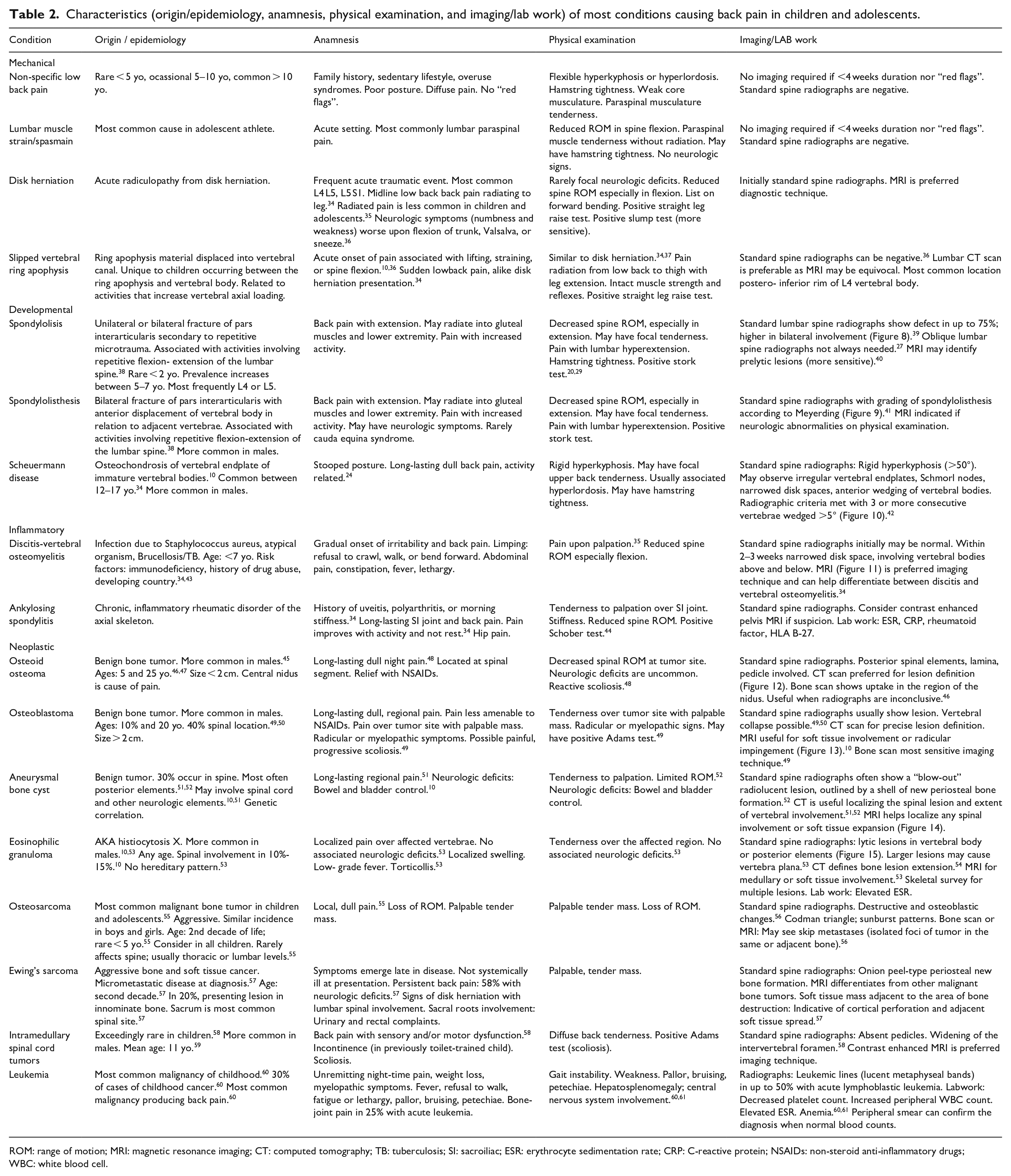
ROM: range of motion; MRI: magnetic resonance imaging; CT: computed tomography; TB: tuberculosis; SI: sacroiliac; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; NSAIDs: non-steroid anti-inflammatory drugs; WBC: white blood cell.
Conclusion
Back pain in children and adolescents is becoming more frequent, and non-specific back pain in this age group has become more prevalent, especially among adolescents. The pediatric patient presenting with back pain can often be challenging, and there are many well-known organic diagnoses that should not be missed. Basic steps should include an in-depth anamnesis, a systematic physical examination, and standard spine radiographs (AP and lateral). If other types of imaging tests are necessary (MRI, CT, bone scan, SPECT), they should be guided by diagnostic suspicion. It is important to keep in mind the differential diagnoses according to age, symptoms, and findings. Pain that alleviates with NSAIDs, night-time pain, and systemic symptoms should raise concerns of neoplasms; young children with poorly defined back pain should raise suspicion of malignant hematologic conditions. Gait abnormalities are the most common sign in discitis following back pain, and spondylolysis is the most common organic cause of back pain in adolescents.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231215860 – Supplemental material for Clinical examination and imaging resources in children and adolescent back pain
Supplemental material, sj-pdf-1-cho-10.1177_18632521231215860 for Clinical examination and imaging resources in children and adolescent back pain by Ana León-Domínguez, Rocío Cansino-Román, Jose M Martínez-Salas and David M Farrington in Journal of Children’s Orthopaedics
Footnotes
Author contributions
All authors have contributed to the research process for this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Animal welfare
This article does not contain any studies with human or animal participants. There are no human participants in this article and informed consent is not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.