
Abstract
Purpose:
This is the second phase in an investigation of the psychosocial impact of orthopedic surgery on adolescents. What are the core psychosocial factors that shape the experience of adolescent patients aged 11–18 who are undergoing orthopedic surgery?
Methods:
Two 43-question surveys (preoperative and postoperative) were developed as modified versions of the survey used in phase 1. The preoperative survey was administered 2 weeks before surgery. The postoperative survey was administered 6 weeks later. Responses were collected from free-response and Likert-scale questions exploring patient–physician relationships, office visits/hospital stays, family, peers, academics, sports, and surgical expectations. The survey was administered prospectively to patients aged 11–18 undergoing limb lengthening/reconstruction, pediatric, spine, sports, or hand/upper extremity orthopedic surgery. In all, 135 patients were identified; 105 were enrolled and completed both surveys.
Results:
There were some statistically significant changes in responses to questions regarding office visits/hospital stays, patient–physician relationships, friends/community, academic performance, and expectations for surgical experience throughout the perioperative period. There were no statistically significant changes in responses to questions regarding the role of parent/family and sports. There was no statistically significant difference between the female and male genders or between age groups in any of the domains. Overall statistical significance in this study did not consistently correlate to clinical significance.
Conclusion:
Adolescents require psychosocial support from their surgeons, caregivers, and peers in addition to respect for their independence and personal needs.
Level of evidence:
Level II.
Introduction
Adolescents are in a stage of development characterized by self-discovery, psychosocial maturation, and increasing independence.1,2 The exponential growth experienced by this patient population makes them particularly vulnerable to aberrant emotional, social, psychological, and personal development if challenged by traumatic events, such as an injury or need to have surgery.3 –5
Musculoskeletal health conditions are often accompanied by pain and the need to spend time in hospitals or other foreign places. When combined with the inability to fully understand surgery and the events that accompany it, adolescents may feel a lack of control over their situation. These events put children and adolescents at risk for psychosocial sequelae such as anxiety, depression, behavior disorders, and post-traumatic stress disorder.4,6,7 In an observational cohort study, Bhandari et al. prospectively examined responses to the Medical Outcomes Study 36-item Short Form (SF-36) in patients aged 16 years and older who presented to orthopedic fracture clinics. They found that 22% of those surveyed met the criteria for a psychological disturbance. Several other reports demonstrate a correlation between orthopedic-related issues and biopsychosocial disturbances.4,6,8 –12 It becomes especially important for orthopedic surgeons to be aware of this in child and adolescent patients due to the potential permanent damage to their mental well-being.
This study is the second in a series that aims to understand the unique experiences of children and adolescents undergoing orthopedic surgery. This knowledge will enhance awareness of emotional, psychological, and social stressors related to orthopedic surgery in this patient population. It will also provide orthopedic surgeons with tools to recognize and screen for mental health disturbances throughout the perioperative period.
In phase 1 of this series, it was determined that the psychosocial needs of adolescents undergoing limb lengthening and reconstruction surgery (LLRS) fell into seven categories: patient–physician relationship, parent involvement, body image and self-esteem, peer support, hospital experience, subjective perception of the orthopedic problem, and academic performance. The authors concluded that patients undergoing LLRS procedures value psychosocial support to aid with their ability to cope. 3 The focus of this phase is to prospectively assess the challenges and psychosocial issues children and adolescents confront when undergoing an array of orthopedic treatments.
The primary aim of this study is to determine how the core psychosocial obstacles adolescents face when undergoing orthopedic treatment change during the perioperative period. The second aim is to identify patterns related to age and gender in their responses to survey questions.
Methods
Approval was obtained from the Institutional Review Board. Patient feedback and findings from phase 1 were used to create the survey for this phase. The novel survey designed for phase 1 was modified into two 43-question surveys for this study (Tables 1 and 2). One was designed to be administered preoperatively. The other was designed to be administered postoperatively. The preoperative survey was given to patients 2 weeks prior to surgery. The postoperative survey was given to patients 6 weeks after surgery. Each prompt was written as a statement, and patients were asked to select the response that reflected their experience. The responses were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.”
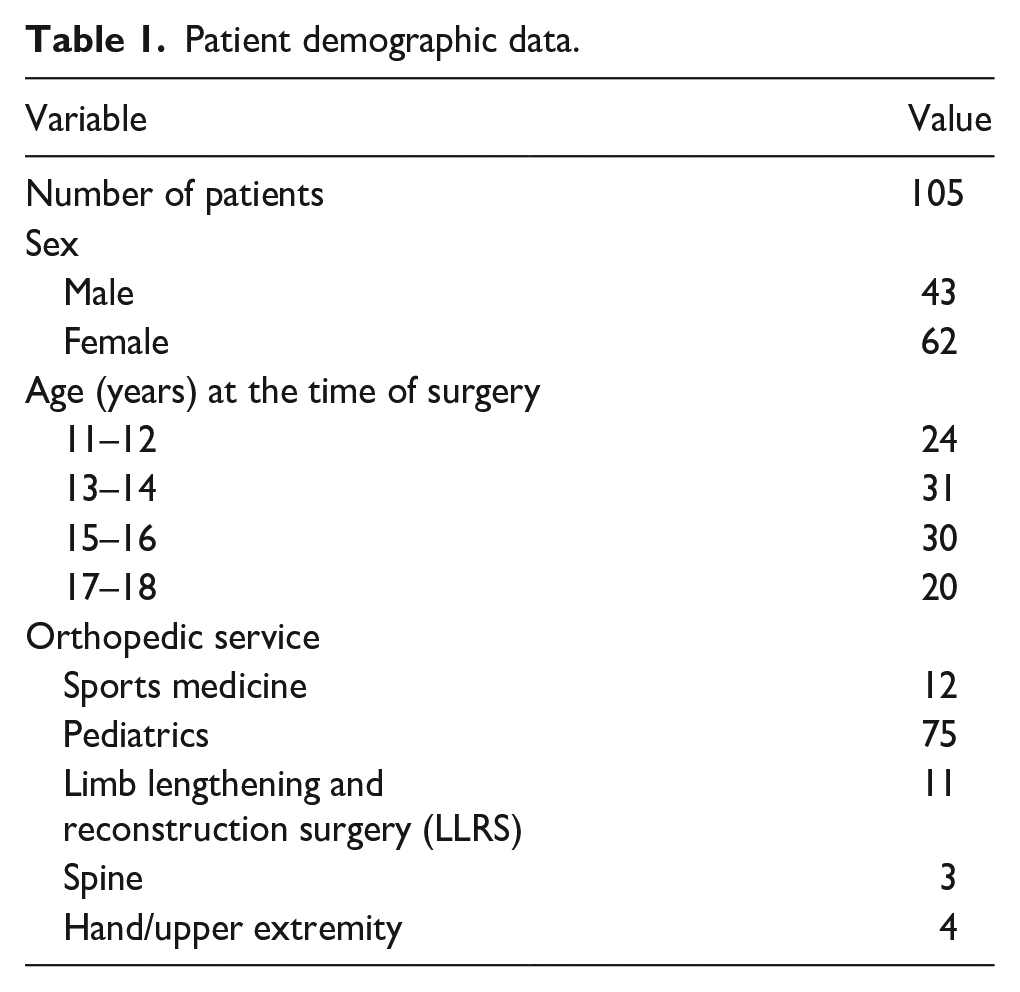
Patient demographic data.
(a) Office visits/hospital stays.
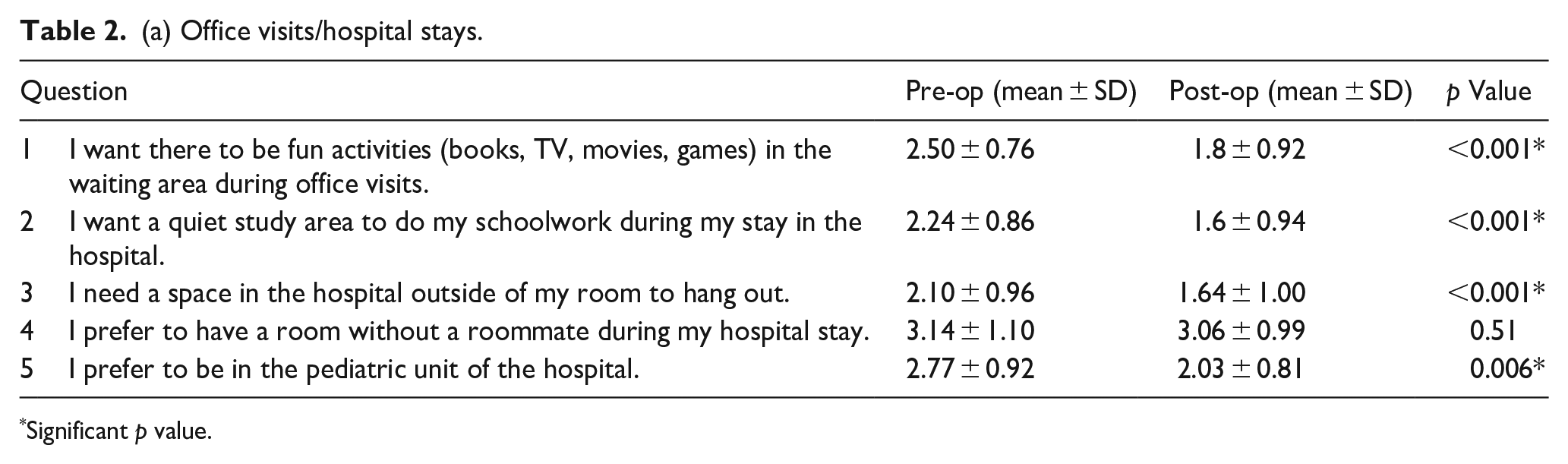
Significant p value.
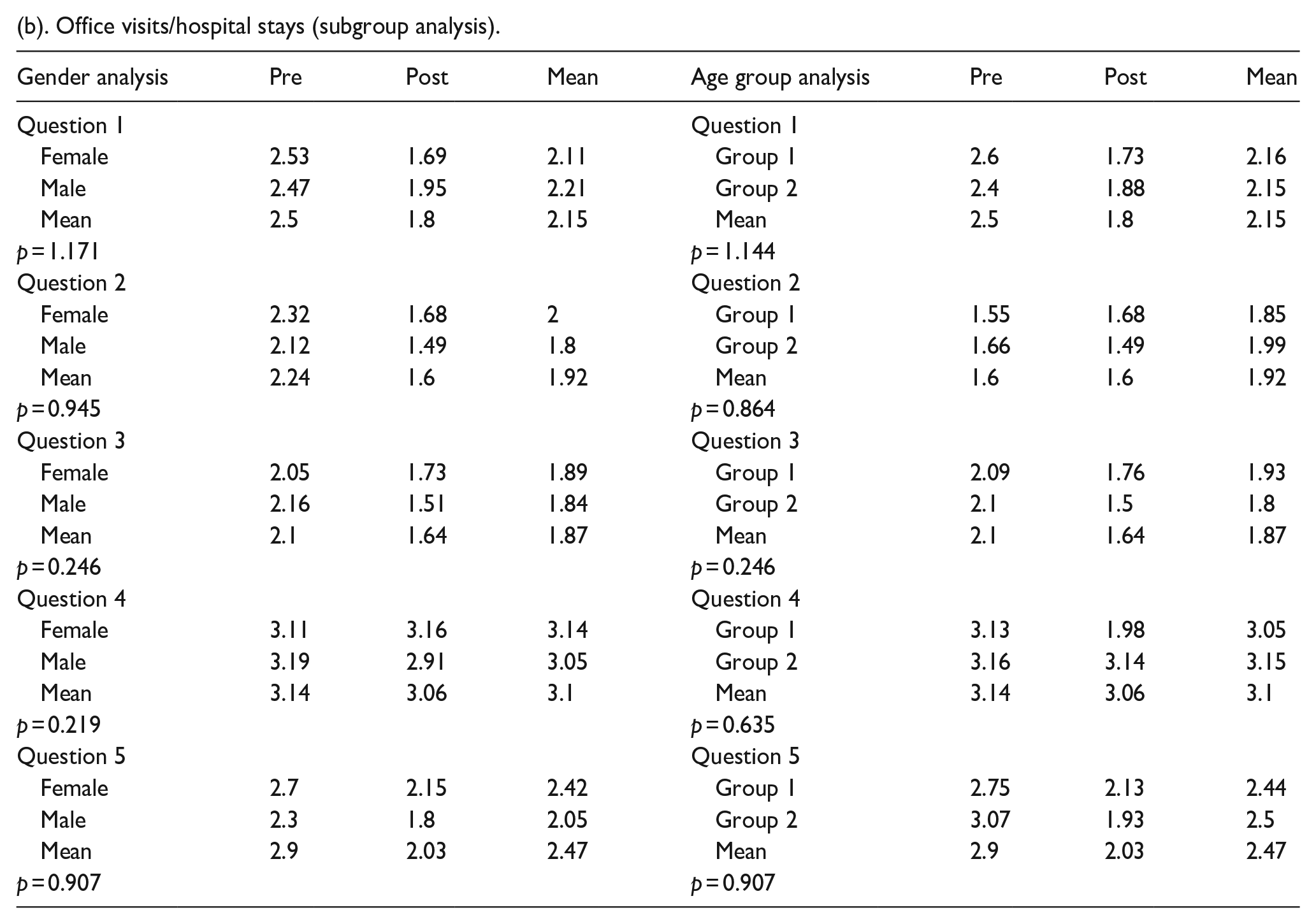
(b). Office visits/hospital stays (subgroup analysis).
A total of 135 patients were identified for the study. In all, 105 patients were enrolled and completed both the preoperative and postoperative surveys. Data from these patients were included in the data analysis.
Inclusion criteria were patients undergoing surgical treatment for an orthopedic condition at the study institution between the ages of 11–18. Patients were recruited from pediatric, spine, sports medicine, hand/upper extremity, and limb lengthening/reconstruction services. Exclusion criteria were patients who would not undergo surgery between the ages of 11–18, who were not able to read, write, or speak English, and those with developmental delays. Once patients were identified, recruitment took place during office visits and via phone or email. Consent was incorporated into the survey.
Statistical analysis
The Likert responses for questions under each domain were converted to a Likert scale score. The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. Responses to each pre-op question were compared to the corresponding post-op question using a simple T-test. Patterns related to age and gender were assessed using an analysis of variance test. The female gender was compared to the male gender for this analysis. Patients aged 11–14 (Group 1) were compared to patients aged 15–18 (Group 2).
Results
In all, 105 patients completed the surveys. The mean age of the patients who completed them was 14.4 ± 2.1 years. 40.95% of patients self-identified as male. 59.05% self-identified as female. Sixty-nine percent of the patients underwent surgery with an attending surgeon in the pediatric orthopedic surgery department at the study institution (Table 1).
The following data represent responses from the preoperative and postoperative surveys.
Office visit/hospital stay
There was a statistically significant decrease in the desire for fun activities in the waiting area during office visits (p < 0.001), a quiet study area to do schoolwork during hospital stays (p < 0.001), and the need for a space in the hospital outside of the patient room to hang out (p < 0.001). There was a statistically significant decrease in the desire to be in the pediatric unit of the hospital in the post-op period (p = 0.006). There was no significant difference in preference for the pediatric unit of the hospital (Table 2a and Figure 1). There was no statistically significant difference between the female and male genders or between age groups (Table 2b).
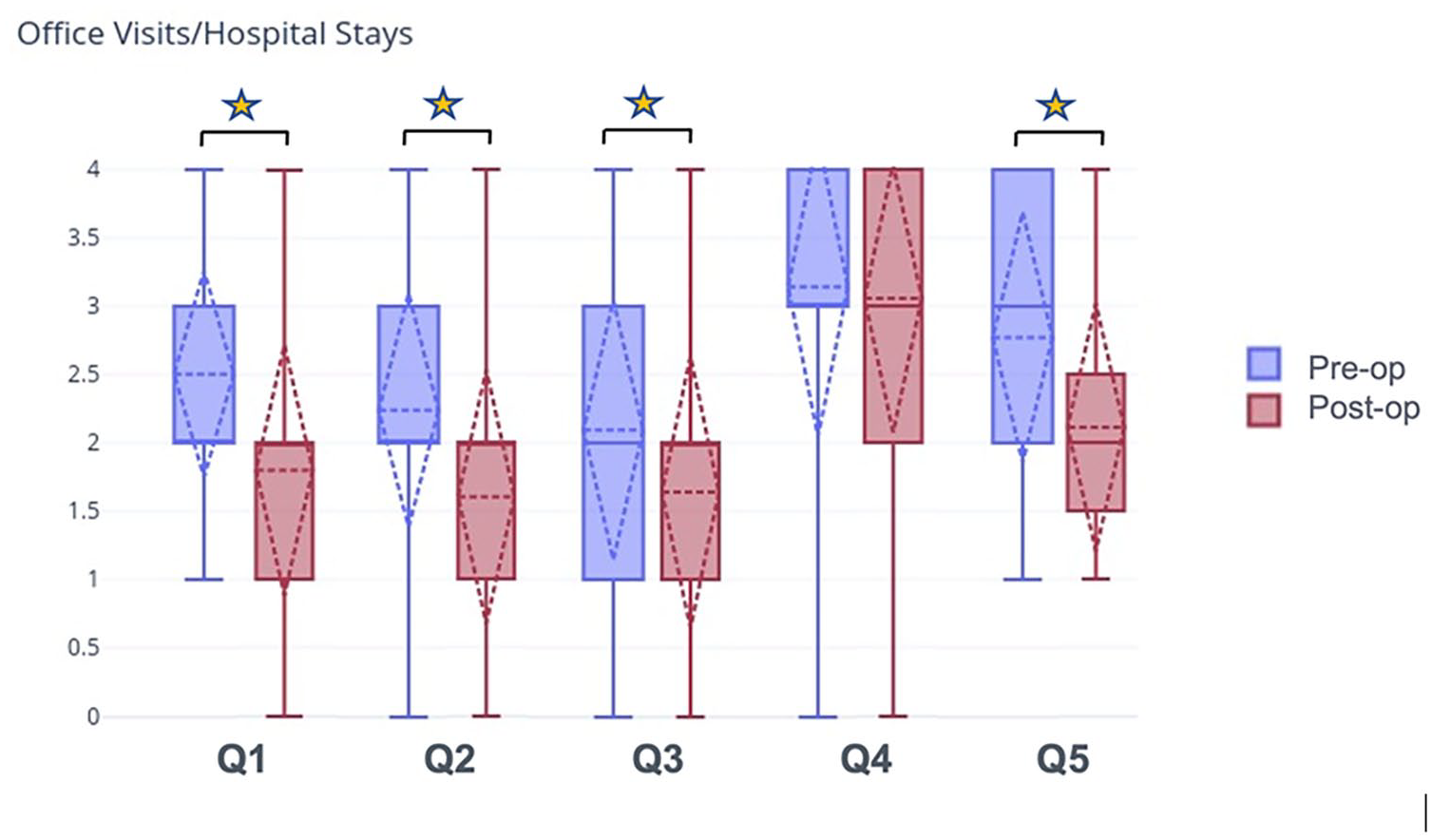
Patients were asked questions pertaining to office visits and hospital stays. The answer choices were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.” The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. N = 105. The star indicates a statistically significant change in preoperative compared to postoperative responses.
Patient–physician relationship
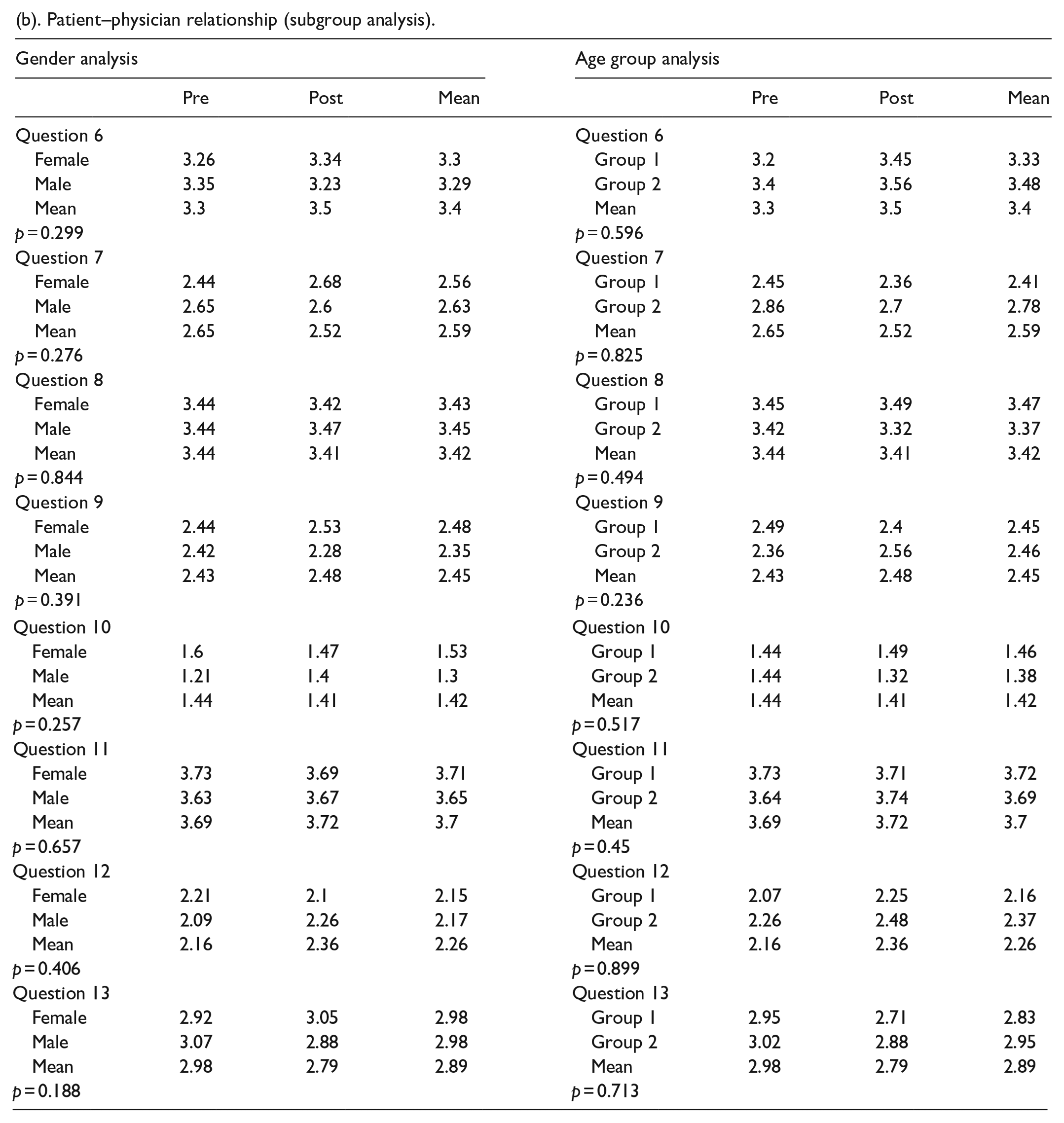
There was no statistically significant change in patient desire to have their surgeon speak to them directly, the desire to have their surgeon explain their condition and how the surgery would help, or the desire to have the surgeon discuss how surgery made the patient feel. There was a statistically significant increase in patient comfort in asking their surgeon questions throughout the perioperative period (p = 0.002). There was no statistically significant change in the desire to speak to a counselor/therapist, for an experienced surgeon, for access to success stories or before/after images, or for the ability to reach someone from the team outside of appointment times. Before and after surgery, most patients wanted to reach their medical team via email and phone (Table 3a and Figure 2). There was no statistically significant difference between the female and male genders or between age groups (Table 3b).
(a) Patient–physician relationship.
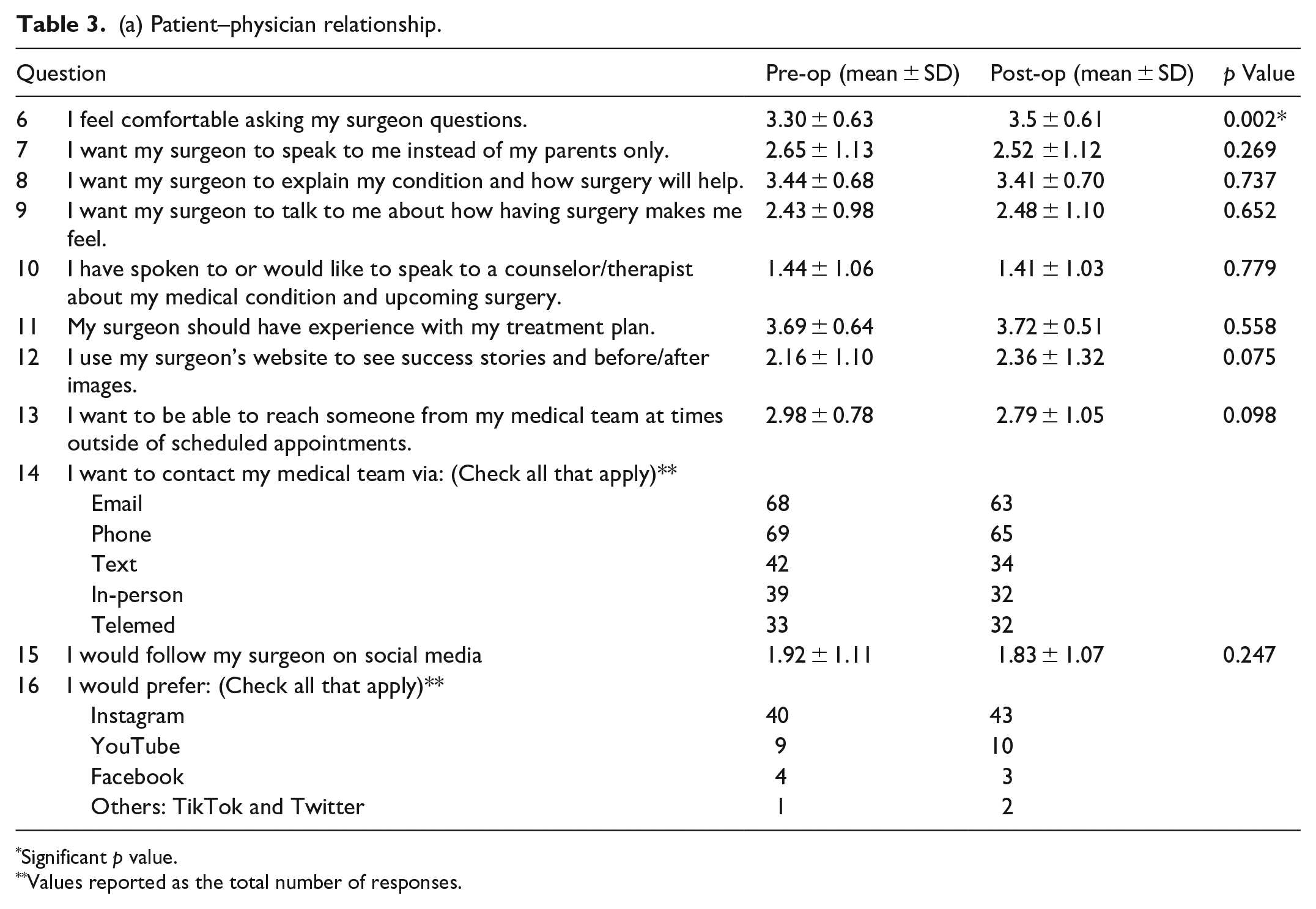
Significant p value.
Values reported as the total number of responses.
(b). Patient–physician relationship (subgroup analysis).
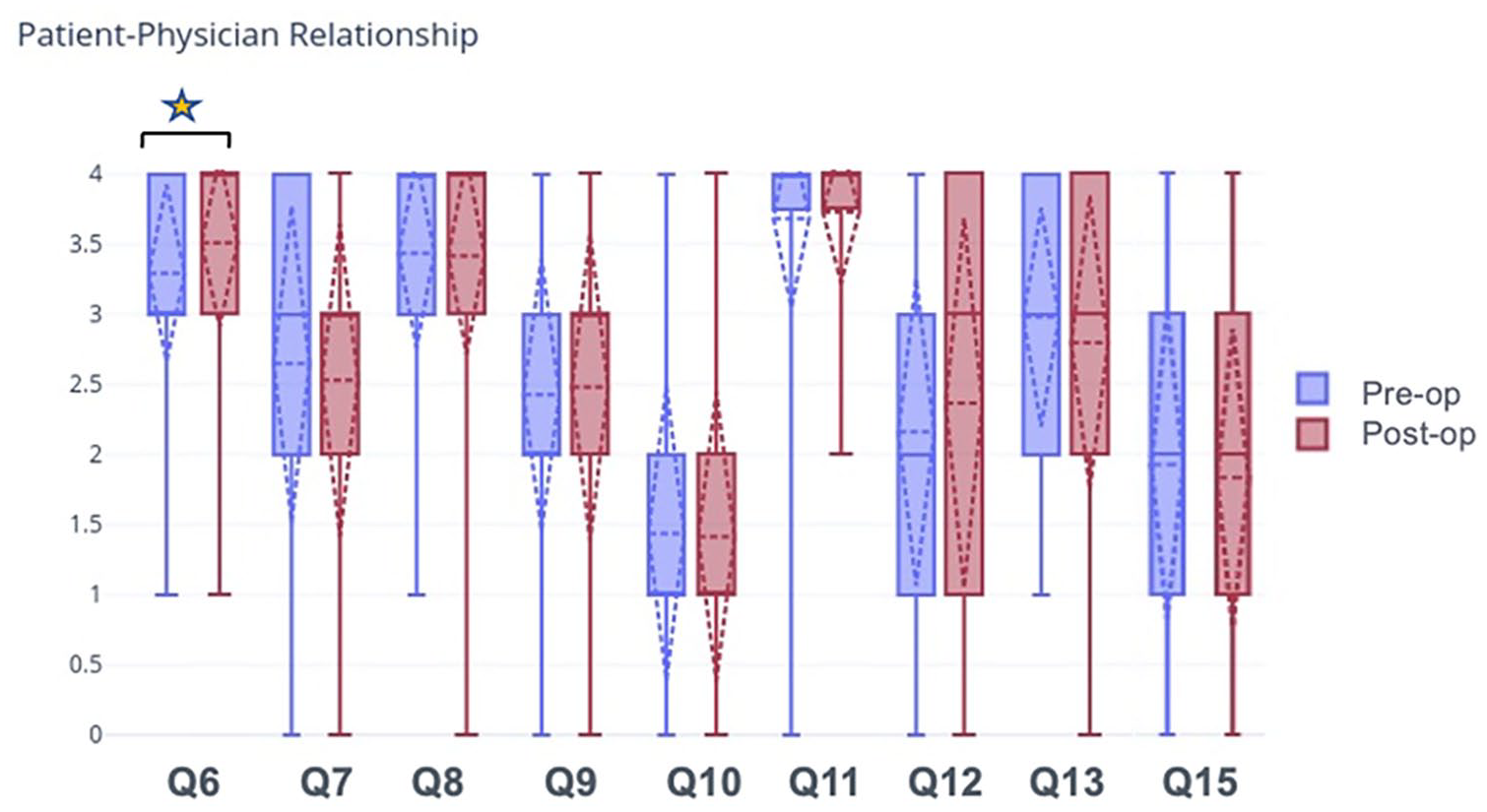
Patients were asked questions pertaining to the patient-physician relationship. The answer choices were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.” The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. N = 105. The star indicates a statistically significant change in preoperative compared to postoperative responses.
Role of parent/family
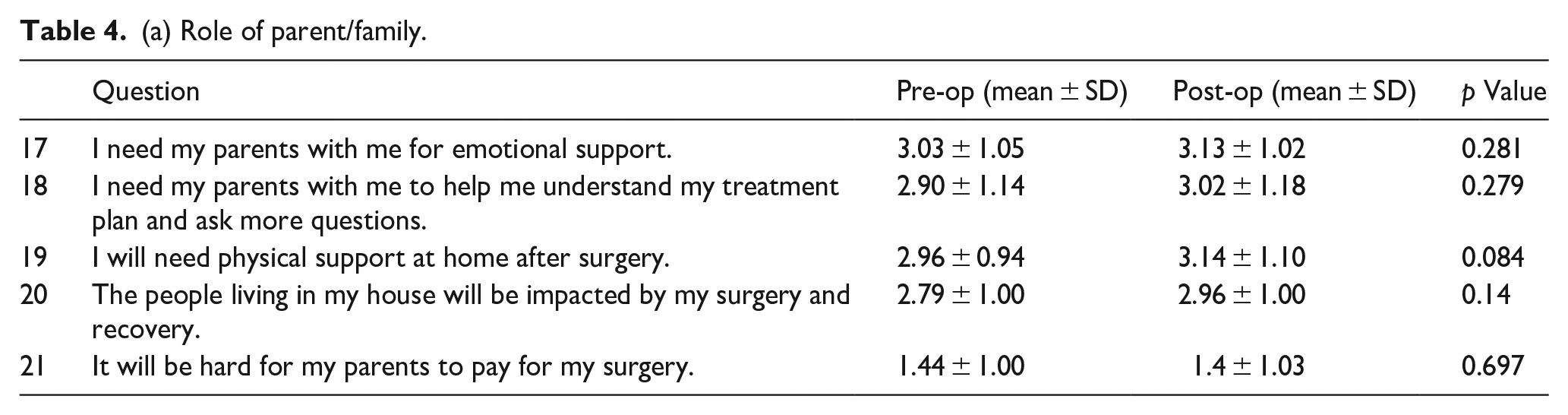
There was no statistically significant difference in the need for emotional support from parents, for parents to help understand the treatment plan/ask additional questions, physical support at home, or in how patients felt about the financial impact of surgery and the effect of surgery on others in the home (Table 4a and Figure 3). There was no statistically significant difference between the female and male genders or between age groups (Table 4b).
(a) Role of parent/family.
(b). Role of parent family (subgroup analysis).
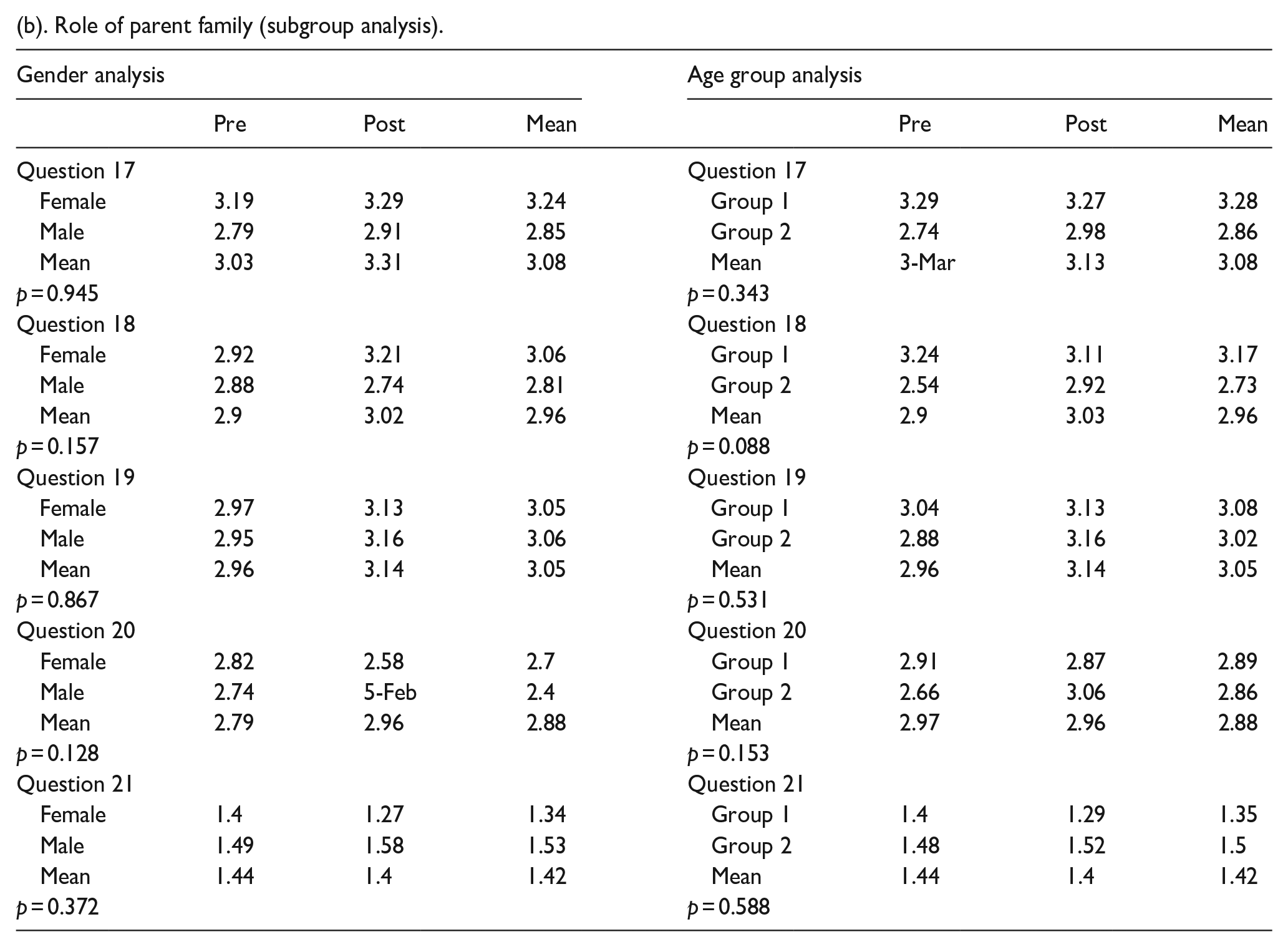
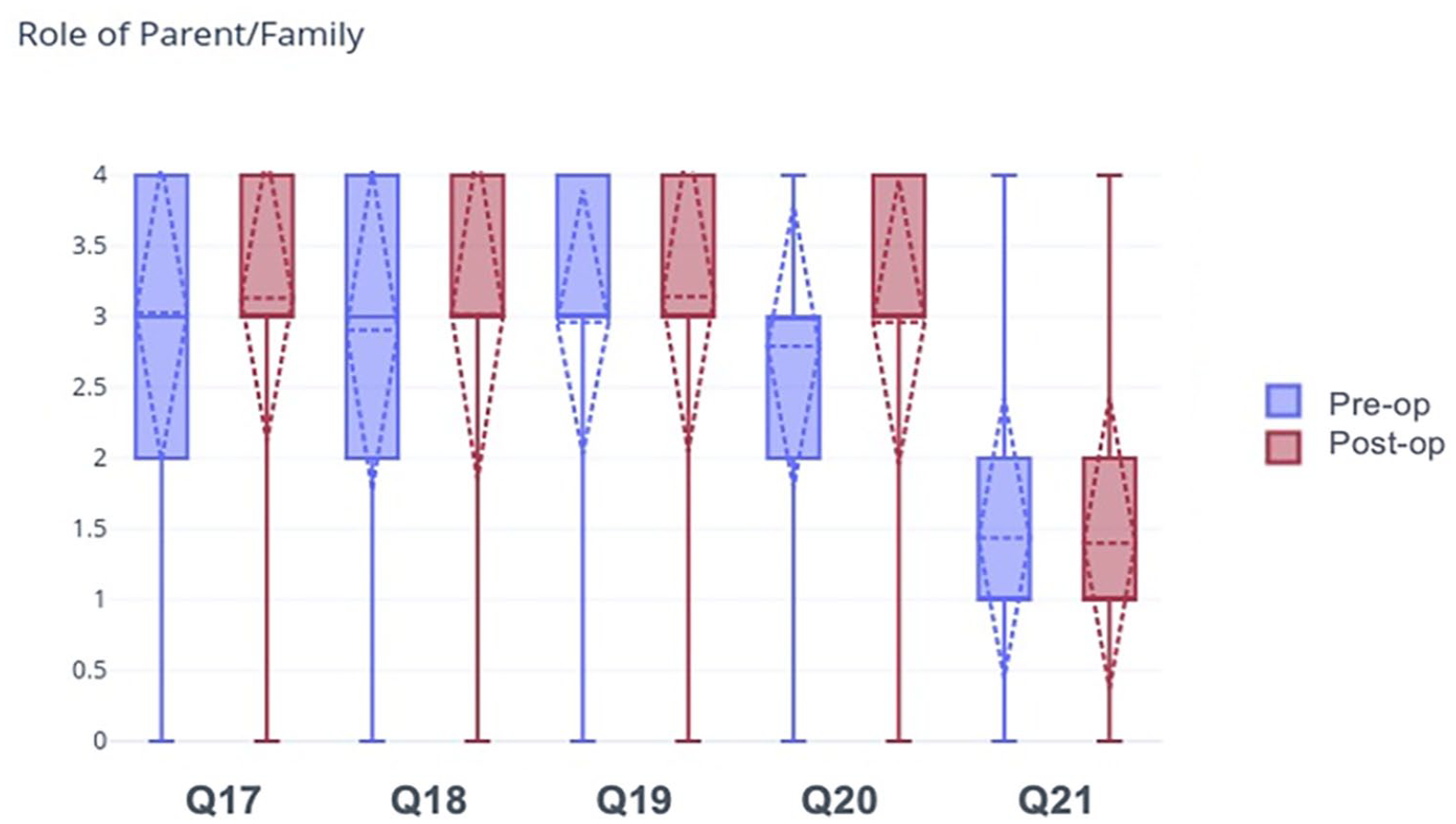
Patients were asked questions pertaining to the role of parent/family. The answer choices were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.” The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. N = 105. The star indicates a statistically significant change in preoperative compared to postoperative responses.
Friends/community
There was no statistically significant difference in how surgery impacted relationships with peers, the desire to keep up with friends during surgery, or the involvement of a religious community in the healing process. There was a statistically significant change in how patients felt about being connected with other patients with similar treatment plans (p=0.003) and in how patients felt about interacting with kids their age during their hospital stay (p = 0.008) (Table 5a and Figure 4). There was no statistically significant difference between the female and male genders or between age groups (Table 5b).
(a) Friends/community.
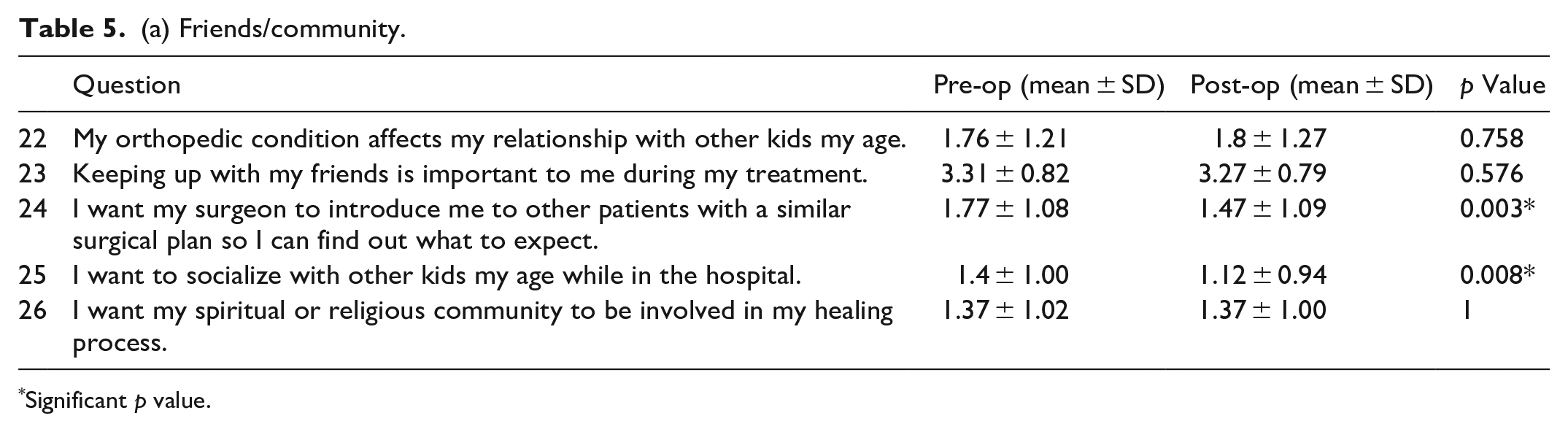
Significant p value.
(b) Friends/community (subgroup analysis).
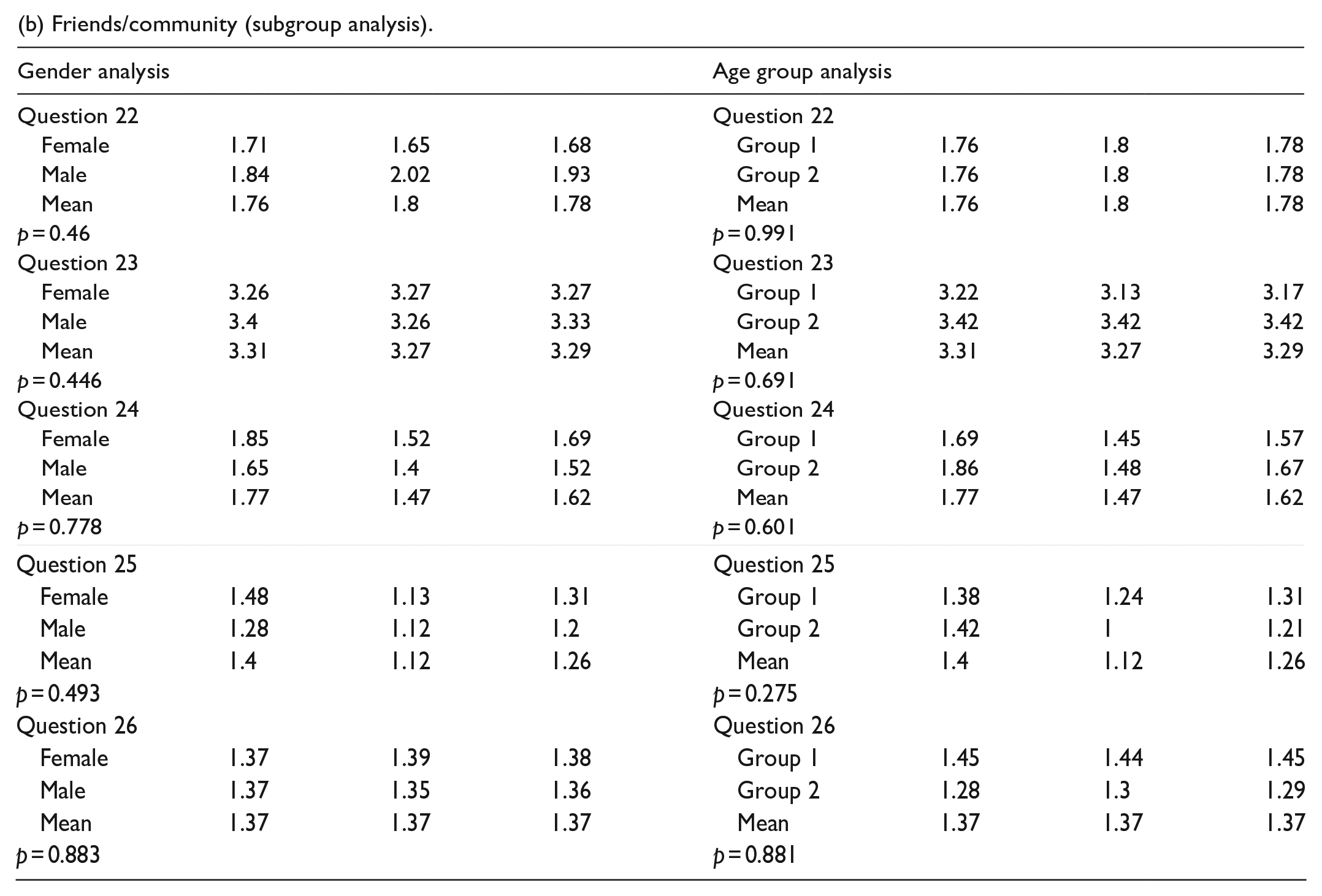
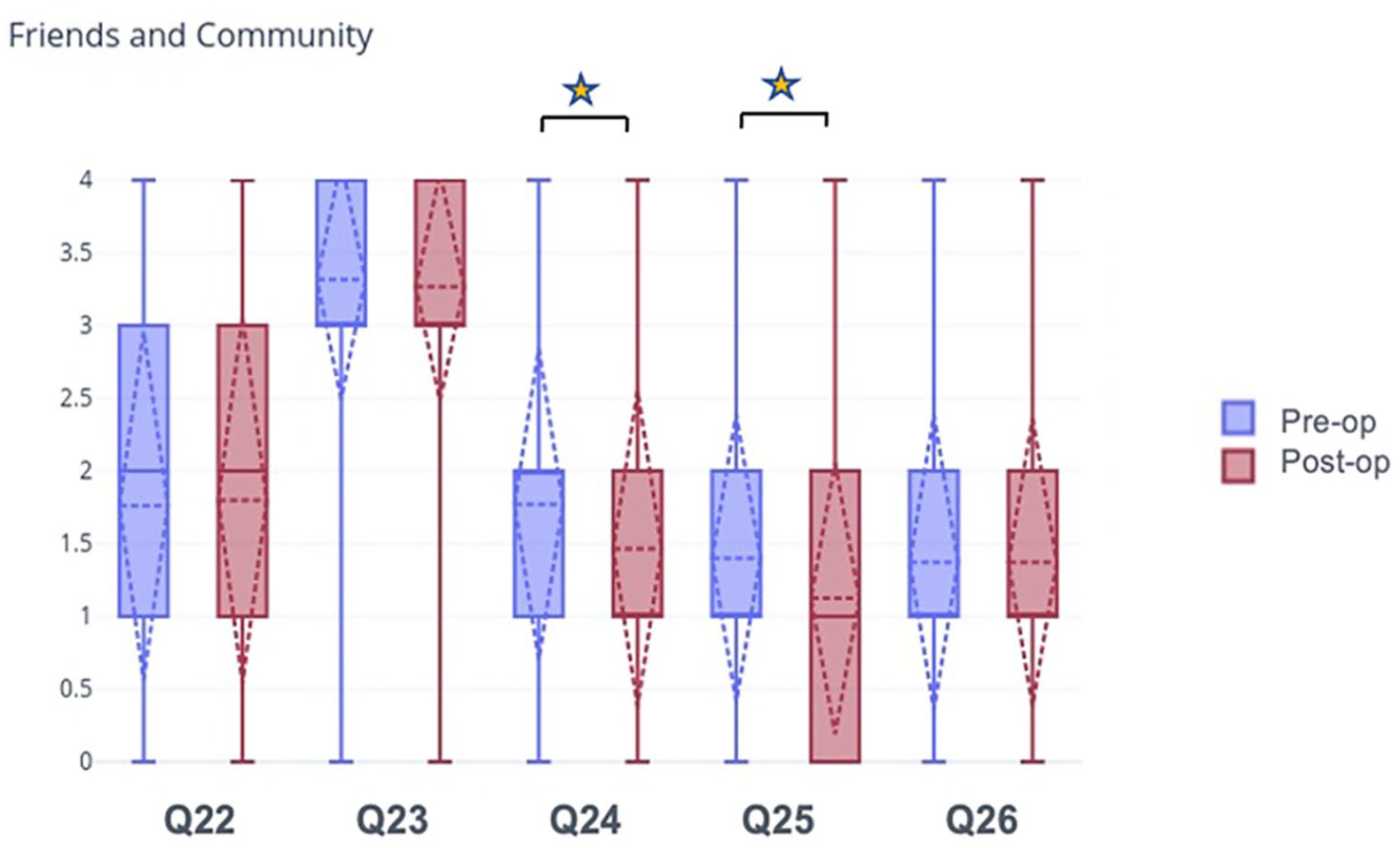
Patients were asked questions pertaining to friends/community. The answer choices were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.” The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. N = 105. The star indicates a statistically significant change in preoperative compared to postoperative responses.
Sports
88.57% of the patients were involved in sports before surgery. 87.62% were involved after surgery. The majority of patients wanted to return to sports and other athletic activities as soon as possible and wanted to return to the same level of activity after surgery (Table 6 and Figure 5).
Sports.
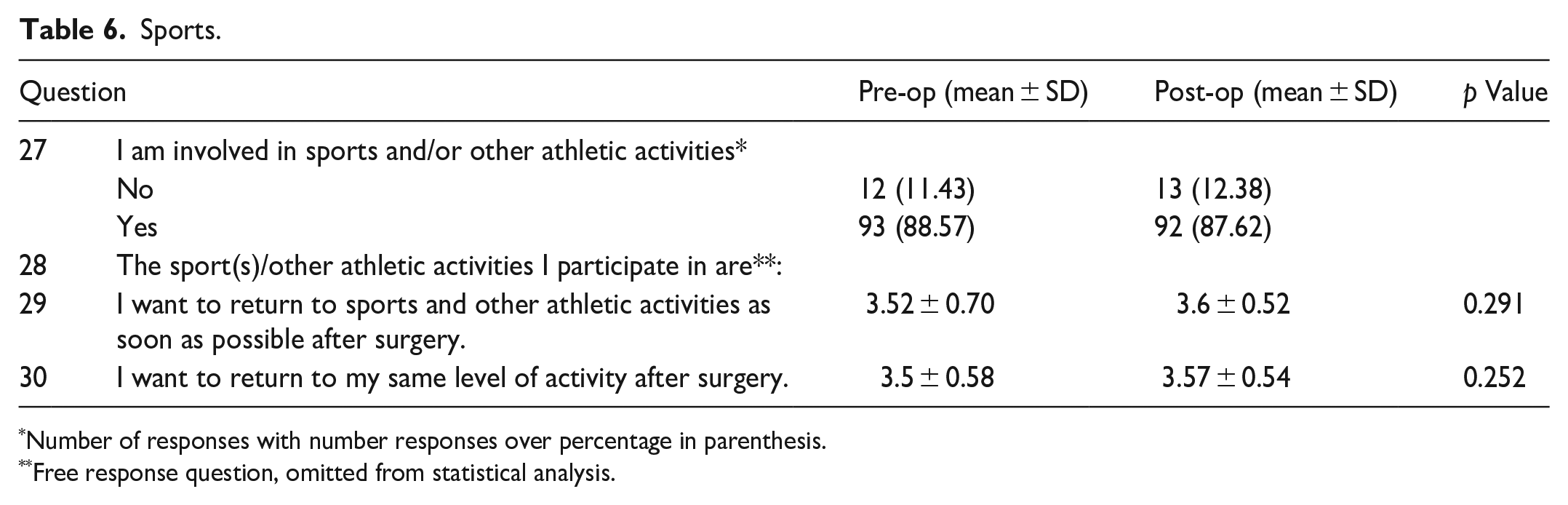
Number of responses with number responses over percentage in parenthesis.
Free response question, omitted from statistical analysis.
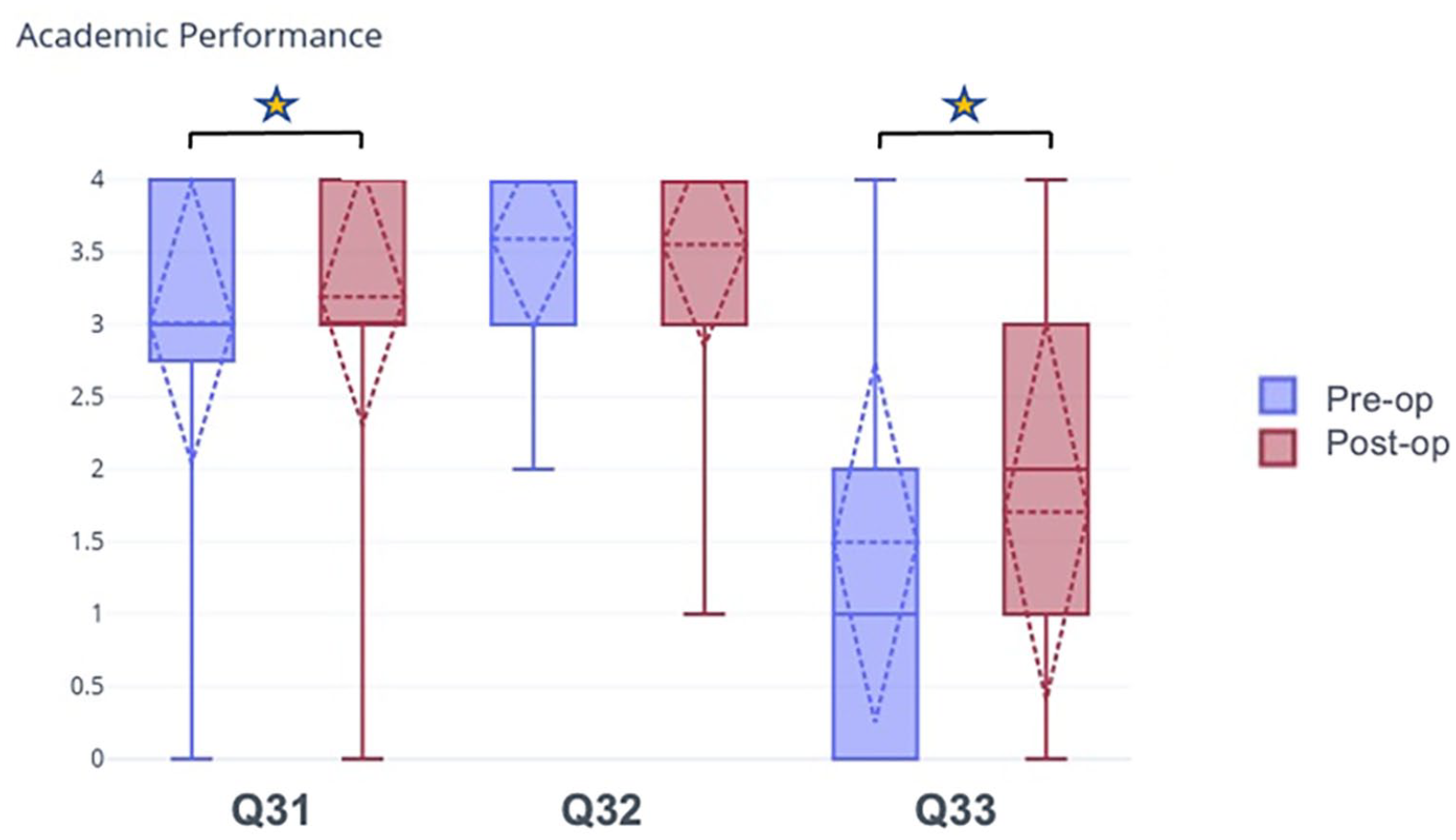
Patients were asked questions pertaining to academic performance. The answer choices were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.” The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. N = 105. The star indicates a statistically significant change in preoperative compared to postoperative responses.
Academic performance
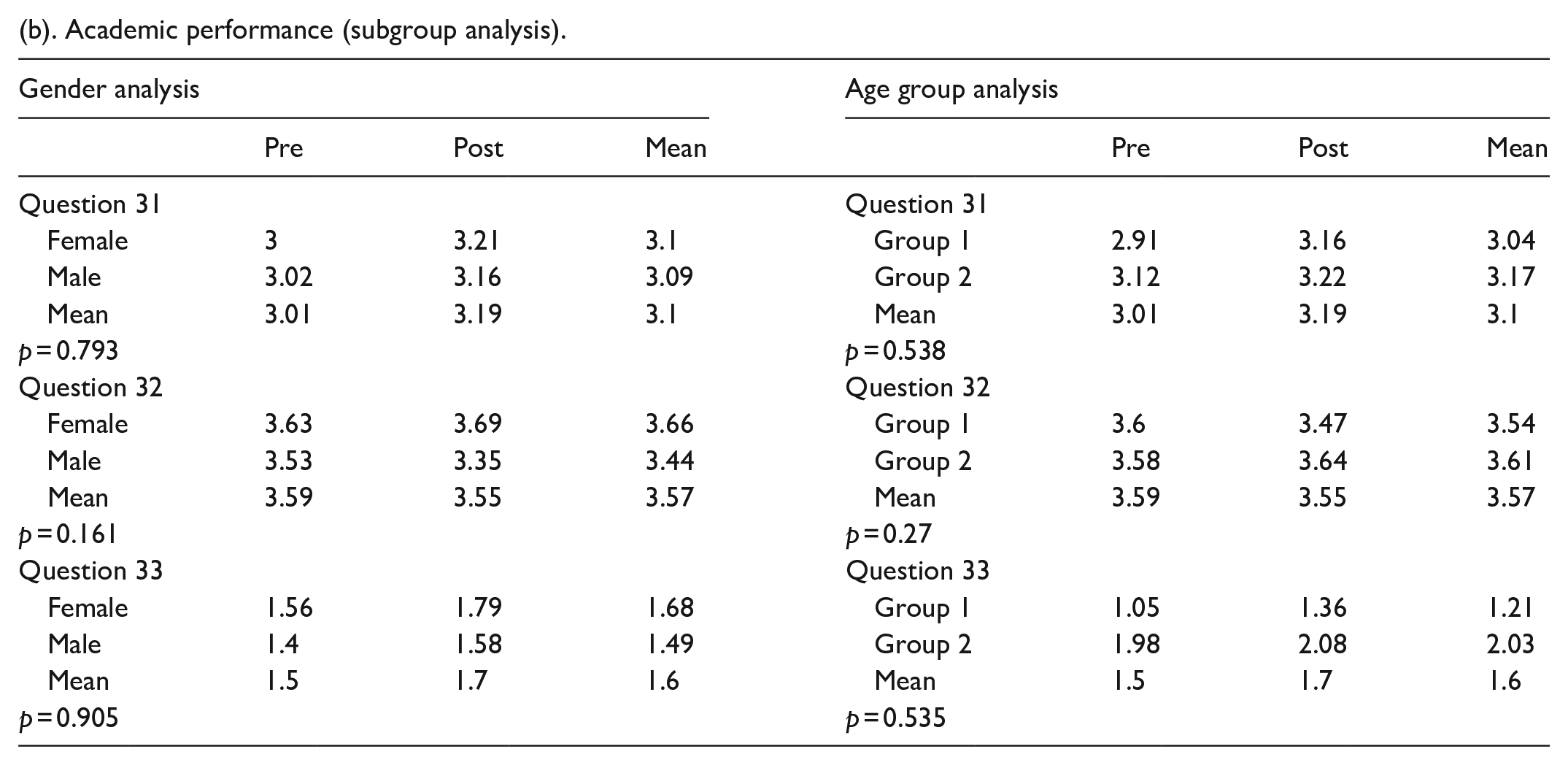
There was a statistically significant increase in patients’ desire to have their school know about their surgery in the postoperative period (p = 0.039). There was a statistically significant increase in the influence of patients’ medical conditions on where they would attend college (p = 0.045) (Table 7a and Figure 6). There was no statistically significant difference between the female and male genders or between age groups (Table 7b).
(a) Academic performance.
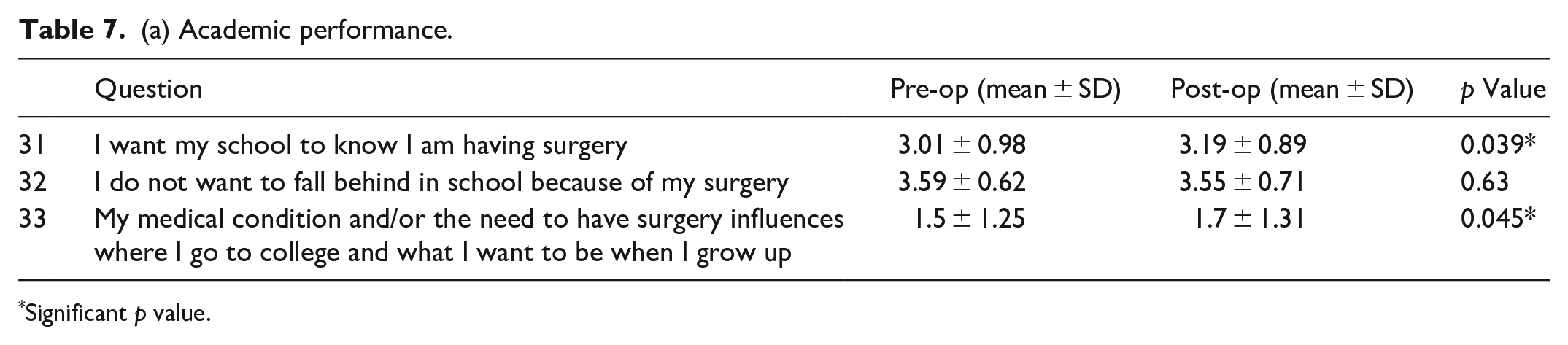
Significant p value.
(b). Academic performance (subgroup analysis).
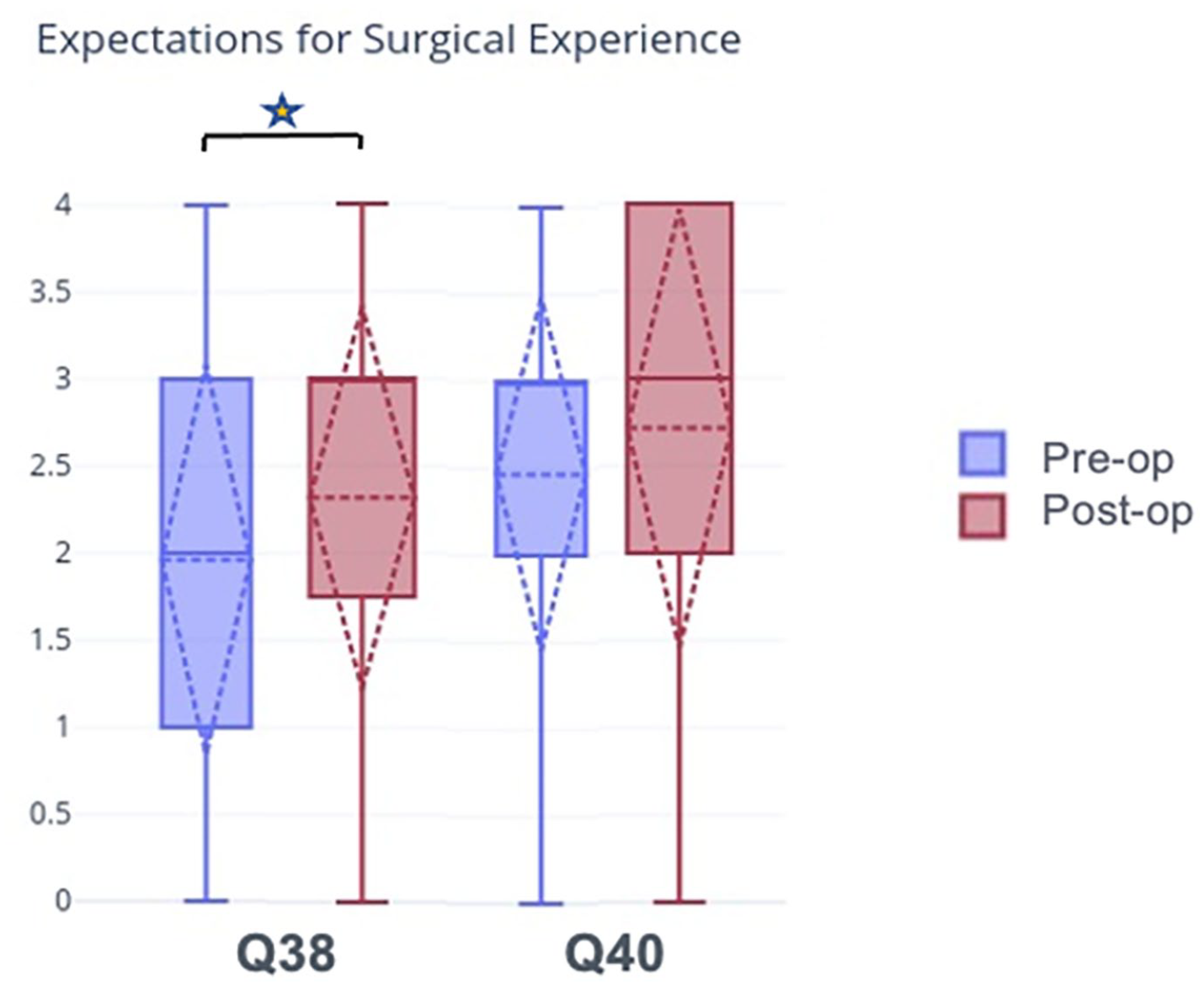
Patients were asked questions pertaining to expectations for surgical experience. The answer choices were “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.” The responses to each question were assigned numerical values as follows: “strongly disagree” = 0, “disagree” = 1, “neutral” = 2, “agree” = 3, and “strongly agree” = 4. N = 105. The star indicates a statistically significant change in preoperative compared to postoperative responses.
Experience of surgery
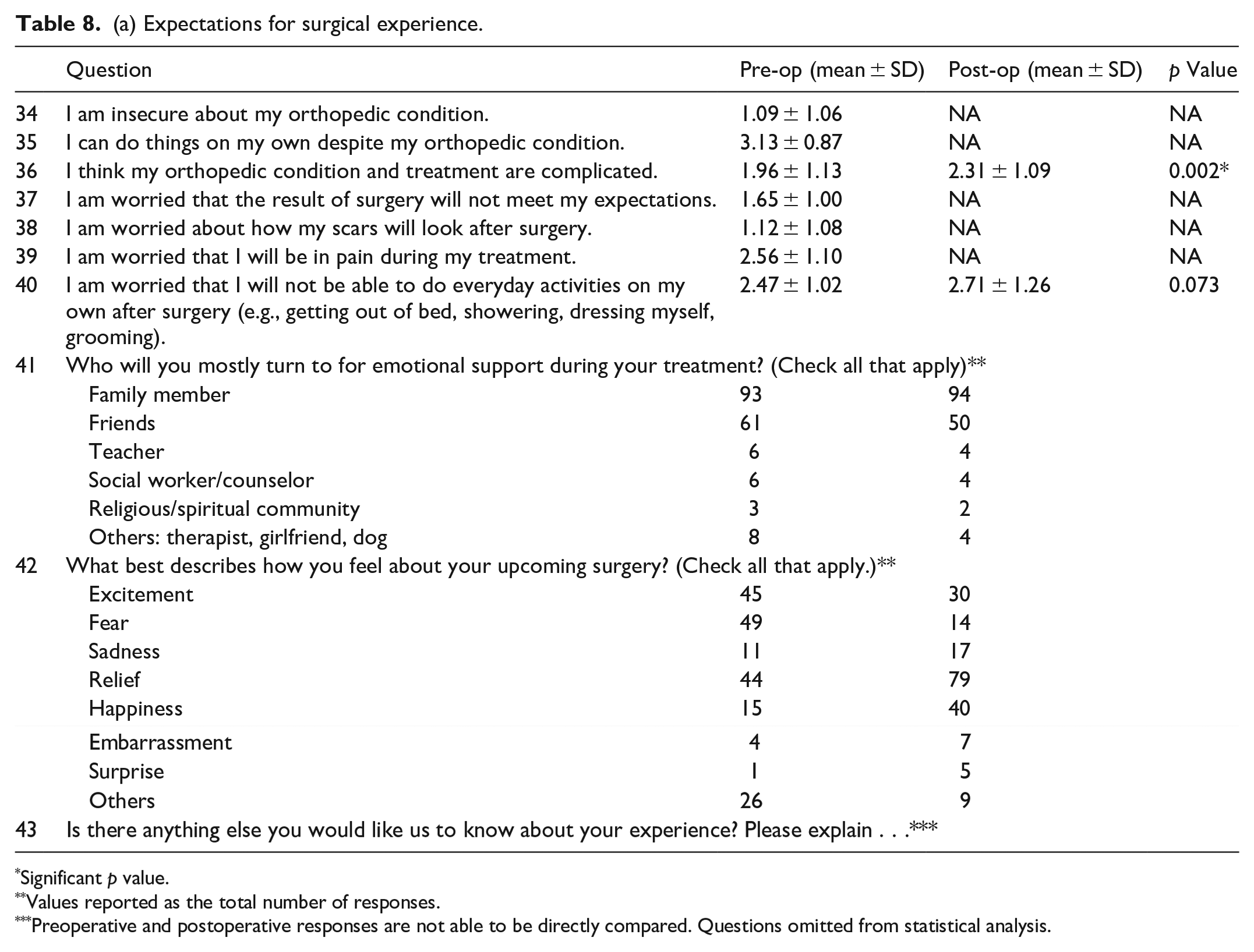
In the preoperative period, patients were not insecure about their medical condition overall and did feel they could do things despite it. There was a statistically significant increase in the perceived complexity of patients’ orthopedic problems in the postoperative period. There was no statistical significance in how worried patients were about the result of surgery meeting their expectations, the appearance of surgical scars, concern about the level of pain felt during surgery, or in concern about being able to do everyday activities independently after surgery (e.g., getting out of bed, showering, dressing, grooming).
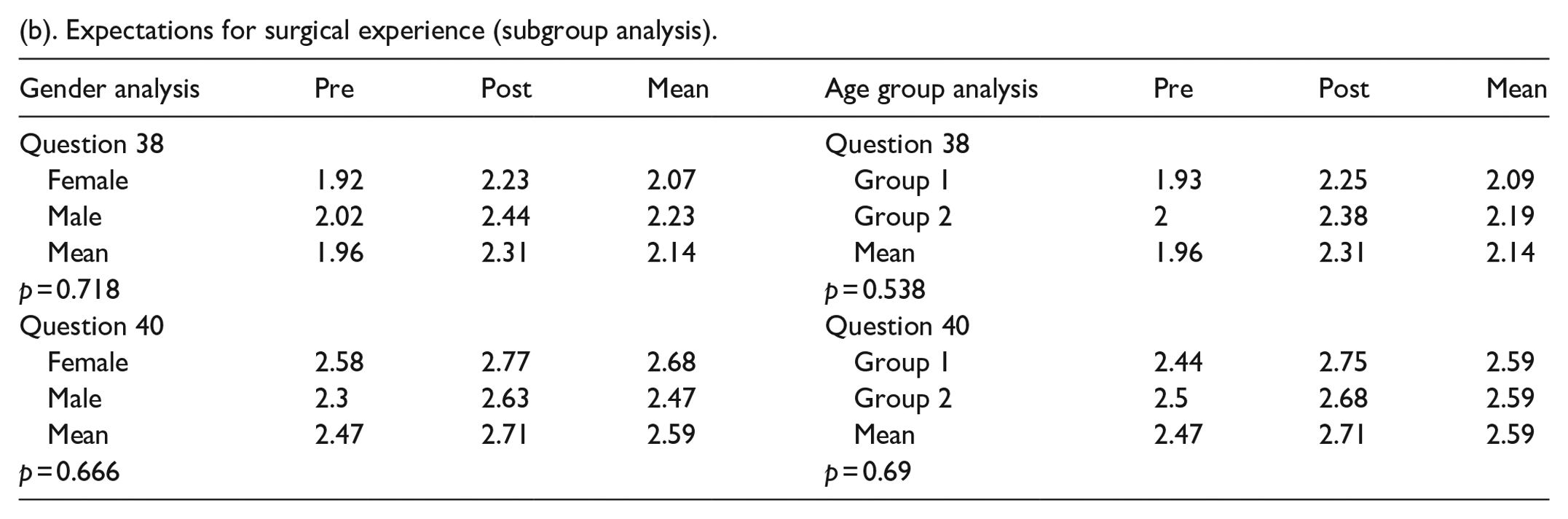
Most patients reported they would go to family and friends for emotional support. Before surgery, most patients reported feeling fear, excitement, and relief about their upcoming surgery. In the postoperative period, patients reported feeling relief, happiness, and excitement (Table 8a). There was no statistically significant difference between the female and male genders or between age groups (Table 8b).
(a) Expectations for surgical experience.
Significant p value.
Values reported as the total number of responses.
Preoperative and postoperative responses are not able to be directly compared. Questions omitted from statistical analysis.
(b). Expectations for surgical experience (subgroup analysis).
Discussion
Studies investigating the psychological, emotional, social, and physical impact of orthopedic surgery on adolescent patients are scarce in the orthopedic literature.3,7 These factors are known to be important in adolescent healthcare, especially with regard to symptoms, outcomes, and patient experience.5,7 Considering psychosocial factors in the holistic care of orthopedic patients has been shown to improve outcomes related to pain, perioperative anxiety, recovery, and quality of life. 13 This study aimed to assess what patients anticipate relative to their true experience in specific psychosocial domains.
The patients surveyed for this study did not express concern about surgery meeting their expectations and were generally not worried about the amount of pain they would experience. However, most patients were concerned with their ability to return to activities and the impact of surgery on their academic performance, which are concerns for this age group that have been previously reported by other authors4,14 (Tables 6–8 and Figures 5 and 6). Explaining surgery and allowing patients to ask questions gives them a sense of control over the process and minimizes anxiety4,6,13 (Tables 3 and 4 and Figures 5 and 6). Orthopedic surgeons can further empower patients by helping them set realistic expectations. This is especially important for patients with chronic conditions who may undergo further orthopedic surgery. Mancuso et al. found that patients aged 18–23 had higher expectations for surgical outcomes in the setting of hip replacement surgery. These expectations were specifically with regard to pain relief, ability to exercise, and ability to return to prior activity level. 14
Orthopedic surgeons should strive for optimal communication with adolescents. The patients in this study felt comfortable asking their surgeon questions and wanted their surgeon to speak directly to them as opposed to their parents. The majority of patients agreed they would interact with their surgeon on social media (Table 3a and Figure 2). Orthopedic surgeons have increased their social media presence by sharing clinical and research information on their personal accounts. This is an effective way to communicate with younger patients and build rapport, as their use of social media for health-related information has risen significantly in recent years.15,16
Though parents are key players in healthcare delivery to adolescent patients, the patients themselves should remain the main source of information relating to their surgical experience. Snyder et al. investigated the reliability of the proxy-reported health-related quality of life using the PedsQL (https://www.pedsql.org/about_pedsql.html). They compared responses to the survey in a group of adolescent patients with sports-related musculoskeletal injuries to those of a parent–proxy of the adolescent. They found that the patients’ self-reported measures were lower than those of their parents. This suggests that parents underestimate the potentially harmful impact of orthopedic consultation on physical, emotional, social, and school functioning.7,11,12 The patients in this study valued direct interaction with their surgeon and felt increasingly comfortable asking questions throughout the perioperative period.
Teenage patients in this study had a significant decrease in the desire to be in a pediatric unit, but they maintained the value of a private room throughout the study (Table 2a and Figure 1). This may reflect the inadequacies of a pediatric unit in serving the needs of adolescents and teenagers, who necessitate greater considerations with respect to privacy and autonomy. In a 2008 study of adolescents admitted to a general pediatric hospital, a lack of privacy was the most prevalent and substantial complaint. They felt a lack of personal space when carrying out activities such as using the toilet, grooming, and even carrying out therapy sessions. 17 However, this may have been less of a concern in the patient population surveyed in this study, as they had significantly greater concerns regarding their comfort and privacy before surgery than when reflecting upon the experience during follow-up.
A variety of outcome assessments have been used for adolescent patients in the orthopedic setting. Nonetheless, a validated tool specifically for the orthopedic setting does not exist. A concerted effort was made to improve on the limitations of phase 1 of this study and advance toward validating a new quality-of-life assessment tool. In that pilot study, a novel 62-question survey was used to assess the psychosocial needs of a homogeneous group of adolescent patients who underwent LLRS. 3 That cohort was the first to respond to the survey. Hence, a limitation inherent in both assessments is the use of a quality-of-life assessment tool that has not yet been validated.
To improve the pilot study, enrollment was expanded to include patients from additional orthopedic services including pediatric orthopedic surgery, spine, hand/upper extremity, and sports medicine. Capturing patients undergoing a wider variety of orthopedic surgeries makes these results more generalizable to all adolescent orthopedic patients. The survey was shortened to 43 questions to mitigate survey fatigue and encourage completion of both surveys once enrolled. 18 Only one enrolled patient in this study did not complete both surveys entirely. Finally, a section was added to the survey to assess the impact of orthopedic surgery on patients who play sports.
One limitation of the study is the challenge of determining the clinical significance of the findings despite being able to calculate statistically significant changes. Through a series of questions, we were able to infer specific key factors that influence children and adolescent’s orthopedic surgical experience. However, we are unable to measure the degree to which some interventions discussed in the study will improve the mental status, physical function, or ability to socialize in this patient population, which would demonstrate clinical significance. 19 In addition, some findings that were not found to have statistical significance do not necessarily lack clinical significance. For example, there was no statistically significant change in the desire to stay in a hospital room without a roommate, but the mean score for the responses was greater than 3 suggesting the majority of participants “agree” or “strongly agree” with this sentiment (Table 2a). This reflects an intervention that possibly has clinical relevance for this patient population. Despite the amount of statistically significant findings presented in this study, it is important to also highlight which of these findings will have clinical relevance.
Our ultimate goal is to implement changes in patient care, throughout office spaces, and at the level of the hospital to improve best practices. Knowledge gained is expected to improve healthcare providers’ understanding of the psychosocial needs of their patients to enhance best practices.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241278159 – Supplemental material for Core psychosocial insights, challenges, and opportunities in the orthopedic surgery care of children and adolescents
Supplemental material, sj-pdf-1-cho-10.1177_18632521241278159 for Core psychosocial insights, challenges, and opportunities in the orthopedic surgery care of children and adolescents by Amber A Hamilton, Jidapa Wongcharoenwatana, Jason S Hoellwarth, Adam Geffner, Rena Mehta, B Sue Epstein, Peter D Fabricant, Austin T Fragomen and S Robert Rozbruch in Journal of Children’s Orthopaedics
Footnotes
Author contributions
A.A.H., R.M., B.S.E., P.D.F., A.T.F., and S.R.R. created the project and main conceptual ideas. A.A.H., A.G., and R.M. contributed to the data collection. All authors interpreted the results. A.A.H. wrote the article with input from all other authors. S.R.R. directed the project.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Fabricant reports personal fees from BICMD, Inc., HS2, LLC, HSS ASC Development Network, LLC, Joint Effort Administrative Services Organization, LLC, and Osso VR, and is a board member of Clinical Orthopaedics and Related Research outside the submitted work. Dr. Fragomen reports personal fees from Smith and Nephew, Synthes, and NuVasive outside the submitted work. Dr. Hoellwarth reports personal fees from Stryker. Dr. Rozbruch reports personal fees from Informa, Johnson and Johnson, Nuvasive, Osteosys, and Springer and Menges family donation to Limb Lengthening and Complex Reconstruction Service research and education fund 2126 at Hospital for Special Surgery outside the submitted work. All other authors have no conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Menges family donation to the Limb Lengthening and Complex Reconstruction Service Research and Education Fund 2126 at Hospital for Special Surgery.
Ethics approval
This study was approved by the Institutional Review Board of the Hospital for Special Surgery, and the protocols used in the study were approved by the Hospital for Special Surgery Educational and Social Services Clinical Review Panel. Informed consent forms were approved by the Hospital for Special Surgery. Educational and Social Services Clinical Review Panel.
Informed consent
All participants were over the age of 18. Informed consent was obtained from all individual participants included in the study.
Research involving human participants
This research involved human participants. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.