
Abstract
Abstract
Purpose
Bone reconstruction after malignant tumour of the lower limbs is a challenge. Our aim was to investigate the results of bone lengthening and transport using the Fitbone motorized lengthening nail.
Methods
Eight patients were included. Two patients had had a tumour involving soft tissue only without bone resection. In six patients, the initial bone defect was 15.5 cm (8 to 24). The first step of reconstruction had consisted of temporary fixation and a cement spacer. The second step had consisted of bone grafting in five patients. One patient was managed with bone transport. Eventually, five patients had a limb-length discrepancy (LLD) managed with bone lengthening only. Two patients had a LLD and a nonunion managed with bone transport and lengthening. Mean age at bone lengthening was 15.2 years (11 to 19). Mean follow-up was 30.5 months (10 to 48).
Results
In all, 11 nails were implanted in eight patients (eight femurs, three tibias). Mean length gain per procedure was 54.5 mm (30 to 80). Mean healing index was 48.4 days per cm (22.6 to 85.7). The complication rate was 18%. In two cases we observed a loose locking screw, which was revised. In all cases the lengthening involved the short bone (femur or tibia). Mean Musculoskeletal Tumor Society (MSTS) score improved from 52.7 (16.6 to 73.3) to 79.9 (63.3 to 96.6).
Conclusions
Bone reconstruction using a motorized intramedullary nail stands as a safe and reliable alternative after malignant tumour. It allows biological reconstruction with satisfactory clinical and radiological outcome and low complication rate.
Level of evidence
III
Introduction
Most lower limbs malignant tumours in adolescents are located around the knee joint, close to the most active growth plates. 1 Advances in chemotherapy and medical imaging have dramatically improved long-term survival.2,3 Limb salvage can now be achieved in the vast majority of patients using reconstruction such as composite bone allograft, bone autograft, vascularized fibular autograft or tumour prostheses. The choice of reconstruction strategy is tailored to each individual patient, taking into account, the location of the tumour in relation to the adjacent joint and growth plate, the tumour volume, the bone growth potential and the overall survival rate. The functional impact of treatment has to be carefully considered and long-term outcome anticipated. Biological bone reconstruction is, therefore, advocated whenever possible but it remains a challenge with technically demanding procedures and relatively high reoperation rates.4,5 Treatment often generates bone shortening due to large initial bone resection, and damage to the very potent growth plates around the knee further increases the ultimate limb-length discrepancy (LLD). The subsequent functional deficit may compromise walking ability and generate low back pain and cosmetic disturbance. New concepts of fully implantable, motorized lengthening devices (powered by magnetic or electrical energy as opposed to devices requiring mechanical action) have now generated new perspectives for reconstruction. The Fitbone nail (Wittenstein, Igersheim, Germany), first introduced in 1998, was Food and Drug Administration approved in 2017. 6 It has provided satisfactory results for bone lengthening with low rates of complications. 7 The aim of this study was to evaluate the Fitbone nail for bone lengthening and bone transport after malignant tumour resection in adolescents. Our hypothesis was that it also provides satisfactory results in tumour patients with no higher complication rate despite the increased risks.
Patients and Methods
Patients
Between 2013 and 2015, we prospectively enrolled eight consecutive patients (six male and two female patients) who underwent wide excision of a malignant tumour of the lower limb followed by bone lengthening and/or transport using the Fitbone intramedullary nail. Mean age at tumour excision was 11 years (6.7 to 15.9). All patients had tumour free resection margins. Two patients had had a tumour involving the soft tissue only and had not required bone resection. Both were treated with adjuvant external radiation therapy at the knee level which generated the LLD. In six patients, initial reconstruction had been performed in two steps. The first step had combined a bone cement methyl methacrylate spacer filling the bone defect and stabilization using either a locking plate, locking nail or flexible nails. The second step had consisted of cancellous bone grafting according to the Masquelet-induced membrane technique in five patients. 8 One patient was managed with bone transport within the induced membrane. Eventually, five patients had a LLD after adjuvant chemotherapy and were managed with bone lengthening only. Two patients had a LLD and a nonunion managed with bone transport and lengthening in a single procedure. Projected LLD at skeletal maturity was calculated using Paley's multiplier method. 9 Demographics and oncological data of the patients are presented in Table 1.
Demographics and oncological data
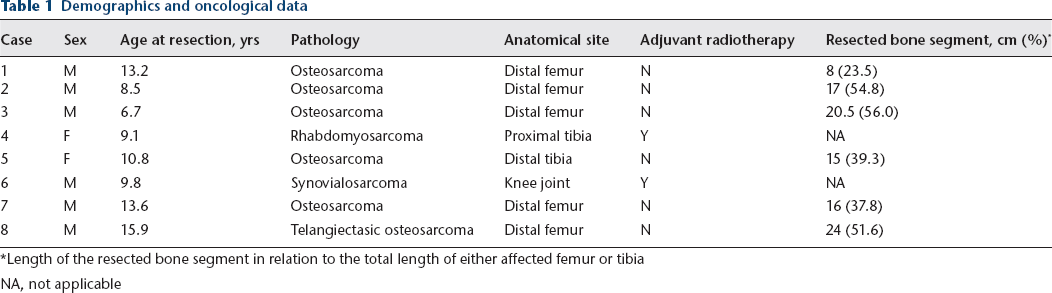
Length of the resected bone segment in relation to the total length of either affected femur or tibia
NA, not applicable
Surgical procedure
The preoperative planning was done according to the reverse planning method. 10 The amount of planned lengthening per procedure was equal either to the maximum length gain provided by the selected implant (30 mm to 80 mm), or to the projected LLD at skeletal maturity, whichever was the smaller. Osteotomies were performed through a stab incision, using a 4.5-mm power drill then an osteotome for optimal callus formation, carefully avoiding the radiated field in those two patients who had received radiotherapy. All nails were implanted through an antegrade approach both at the femur and tibia. Bone reaming was performed using rigid reamers through a tube system in 0.5-mm increments until 0.5 mm above the diameter of the selected implant. The product of bone reaming was used as an autograft at the osteotomy site. Blocking screws were placed when needed for acute deformity correction or to add further stability. In three cases a bone transport and subsequent bone lengthening were performed by use of a custom made Fitbone nail. The distraction osteogenesis was initiated between day 3 and 5 at a rate of 1.0 mm per day in three sessions, using an electronic external control unit. The patient felt the receiver located under the skin and placed the external transmitter against it. Pressing the button once triggered the energy transmission and generated nine impulses in a total of 90 seconds with visual and audible feedback. The patients were followed up on a weekly basis during the distraction phase, then monthly until bone healing was obtained. Physiotherapy was started at day 1 with knee and ankle passive and active unrestricted mobilization, walking with crutches and a weight bearing of 20 kg on the operated limb.
Data analysis and statistics
Standardized anteroposterior and lateral long-standing radiographs of both lower limbs were obtained preoperatively and at latest follow-up. Mechanical axis deviation (MAD), LLD, mechanical lateral distal femoral angle (LDFA) and medial proximal tibial angle (MPTA) were analyzed using TraumaCad software (Brainlab, Munich, Germany). Length gain and bone healing were analyzed. Bone healing was defined as corticalization of at least three sides of the callus on the radiographs, with subsequent transition to full weight bearing. Insufficient callus formation was defined as a bone healing time more than three times longer than the distraction period. Leg lengthening was considered successful when within 5 mm from the planned lengthening. Intra- and postoperative complications were recorded and classified as problems (grade 1), obstacles (grade 2) and minor or major complications (grade 3), according to Paley's classification. 11 Function was assessed using Musculoskeletal Tumor Society (MSTS) score before the bone lengthening procedure and at latest follow-up. 12
Results
General
In all, 11 bone lengthening and/or transport procedures were analyzed (three patients (cases 1, 3 and 5) had a planned second lengthening procedure with another Fitbone nail). Mean LLD was 11.8 cm (3.6 to 14.5). Mean time from tumour resection to lengthening procedure was 53 months (10 to 114). Bone lengthening was performed when skeletal maturity was reached or growth of the short bone segment was terminated (growth plate resection or radiation) and the patient and their family were willing to undertake the procedure. The average age at lengthening nail implantation was 15.2 years (11.3 to 19.3). The mean follow-up time was 30.5 months (10 to 48) (Table 2).
Results
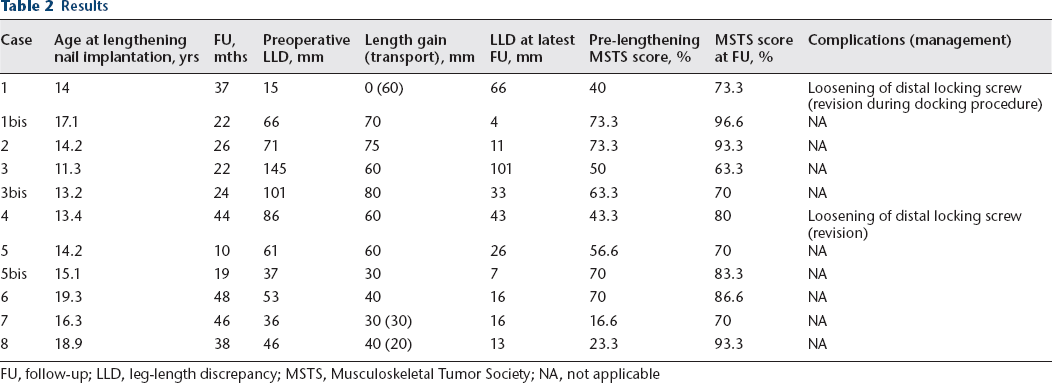
FU, follow-up; LLD, leg-length discrepancy; MSTS, Musculoskeletal Tumor Society; NA, not applicable
Length gain
The mean lengthening distance per procedure was 54.5 mm (30 to 80). The affected, short bone (femur or tibia), was lengthened in all cases according to the planning.
Distraction
The mean distraction period was 77 days (40 to 100) with a distraction index of 1.2 mm per day (0.9 to 1.3).
Bone healing
The mean bone healing time was 269 days (94 to 527), with a healing index of 48.4 days per cm (22.6 to 85.7). The lengthening nail was removed in all patients after an average of 16 months (10 to 22), replaced by a trauma nail in four cases.
Deformity correction
In cases 3, 4 and 8, a correction of the mechanical axis was performed in the coronal plane according to the preoperative planning (Fig. 1). Case 3 had a femoral varus with a MAD of 47 mm and a LDFA of 104°, corrected to 11 mm and 88°, respectively. Case 4 had a femoral varus with a MAD of 18 mm and a LDFA of 90°, corrected to 0 mm and 85°, respectively. Case 8 presented a tibial varus with an MAD of 38 mm and a MPTA of 80°, corrected to 11 mm and 88°. No bone deformity was generated by the lengthening in the remaining patients.

Case 2:
Functional outcome
All patients achieved satisfactory functional outcome. At latest follow-up, no knee extension or flexion deficit were observed in any of the patients and all patients were involved in recreational sports activities. Mean MSTS score was improved from 52.7 (16.6 to 73.3) to 79.9 (63.3 to 96.6).
Complications
No intraoperative complications occurred. No bone or soft-tissue infection was recorded. There was no case of recurrence of the malignancy. The overall complication rate was 18% (two problems).
Bone transport
In cases 1, 7 and 8 bone transport was performed with 6 cm, 3 cm and 2 cm, respectively. Transport was followed by 3 cm and 4 cm bone lengthening in cases 7 and 8, respectively. Bone union was obtained in all three cases after a mean 10 months (6 to 17). Mean healing index was 50 days per cm (30 to 87). Patient 1 had a planned docking procedure during which a loose locking screw was revised.
Discussion
Treatment of malignant tumours of the lower limbs in children and adolescents often generates bone shortening due to the large volume initial excision and damage to very potent growth plates around the knee. Infection rate is increased by the immunosuppressive effect of neoadjuvant and adjuvant chemotherapy and long operating times.13–15 Bone healing is impaired by osteopenia, large surgical approaches and, when present, by radiotherapy. Several procedures are needed to obtain bone union and may generate numerous scars, bone deformities and, sometimes, broken metal.4,16 Joint stiffness is not uncommon with juxta articular bone cuts and prolonged immobilization times. Distraction osteogenesis by use of an intramedullary motorized nail seemed appropriate in this patient population. Indeed, the device implantation can be achieved through stab incisions with minimal damage to the soft tissues and no transfixing pins, which facilitates early unrestricted joint movement and prevents joint stiffening. It offers the possibility of acute correction of axis deformity and also provides stable bone fixation, thus allowing early weight bearing. Overall results of the Fitbone nail for traumatic and congenital LLD are satisfactory, according to the literature.7,17 The complication rate was 18% in our series and no major complications occurred. This rate is not higher than in series of bone lengthening for LLD of miscellaneous origins using the same implant.7,17 Cashin et al 18 recently reported three cases of staged femoral reconstruction after malignant tumour resection. Immediate A frame free vascularized fibular graft was followed by a bone lengthening by use of a custom magnetically driven intramedullary nail. It allowed satisfactory functional outcome, with minimal complications. To our knowledge, the magnetic nail used (Phenix Medical, Paris, France) is not available anymore.
Reconstruction of large bone defects using the Masquelet technique bears a high risk of nonunion. 4 In these patients whose bone stock has often been spoiled for grafting at the second stage of the procedure, bone transport stands as an adequate option for biological secondary reconstruction. Kold and Christensen 19 used a Fitbone for the first reported case of bone transport using a motorized intramedullary nail in 2014. They obtained bone healing of a traumatic nonunion at the distal tibia with 3 cm transport and 2 cm lengthening. Cases 7 and 8 of the current series presented with a nonunion of the distal femur and were both managed using a custom-made Fitbone implant allowing a transport of 3 cm and 2 cm, followed by 3 cm and 4 cm lengthening, respectively. Union was achieved in both cases. Whereas bone transport was used as a secondary procedure in cases 7 and 8, case 1 was primarily reconstructed using a distal femoral metaphyseal allograft and 6 cm bone transport. Union was achieved after a planned ‘docking procedure’. We called this technique ‘induced transport’ in reference of the ‘induced membrane technique’, 8 as the bone segment is transported within the membrane, potentially taking advantage of the presence of bone forming proteins. Its main advantage is the preservation of the bone stock and avoidance of donor site morbidity.
Distraction osteogenesis using the Ilizarov method for primary and secondary reconstruction of bone tumours has provided satisfactory results.20,21 Tsuchiya et al 21 reported on 17 cases of primary reconstruction with a mean distraction of 9.3 cm (3 to 17) and a mean time of external fixation of 352 days (109 to 731). Wire/pin infection rate was 64%, although a single case of deep infection required surgical treatment. Bone grafting was performed at the docking site in all patients after completion of the distraction and needed to be repeated in two patients. Two patients required bone grafting of the regenerate because of poor bone formation. McCoy et al 20 reported their experience of bone lengthening and transport using external fixators in a retrospective series of 18 tumour patients (including upper limb and benign lesion cases). Mean lengthening achieved was 7.1 cm (3.5 to 18) and mean external fixator time was 223.9 days (76 to 467). Overall results were judged good to excellent with two complications, 18 obstacles and six problems. Pin site infection was the most commonly encountered complication. This complication is unique to external fixation, with increased risk of pin loosening and deep infection with prolonged fixator time frequently seen in tumour cases. Hygiene and daily activities are also affected, not to mention the psychological burden. 22 However, external fixation can stabilize very small juxta articular bone segments when intramedullary nailing would require additional allograft for locking. 23 A lengthening nail only allows for single level transport and has a distraction capacity limited to 8 cm. However, this can be tackled by a nail exchange or as recently reported, nail retraction followed by further lengthening. 24 An intramedullary nail can be left in place until full maturation of the bone regenerate, thus protecting the lengthened segment from a fracture after removal of the external fixator. 22
There are some limitations to this study. It is not comparative and involves only a limited number of cases. However, the numbers of skeletally immature patients with malignant tumours amenable to extra articular resection and sparing of the knee are quite low, and the used lengthening implant has only recently been available.
Conclusions
Fitbone is safe and reliable for bone lengthening and transport after malignant tumour resection in adolescents. It allows a biological reconstruction with satisfactory clinical and radiological results, low complication rate, and nearly normal function.
Footnotes
CTL: Manuscript preparation.
EP: Data analysis and manuscript preparation.
TBT: Study design and performed measurements
FD: Performed measurements and manuscript preparation.
JSDG: Study design and manuscript revision.