
Abstract
Abstract
Purpose
Little data is available on the efficiency of different implants for epiphysiodesis. The purpose of this study is to compare the efficacy between plates and staples in decreasing leg-length discrepancy.
Methods
A retrospective review of 19 children who underwent temporary epiphysiodesis of the legs was conducted, with a minimum of two years of follow-up. The bone length and length ratio to the short side were measured at six months, one year and two years postoperatively. The change in discrepancy was compared between staples and plates by an independent t-test, and the shortest time to a significant decrease in discrepancy was determined using a paired t-test.
Results
Ten patients underwent 13 staple procedures in nine femurs and four tibias for a 2.8-cm discrepancy at age 11.8 years, and nine patients underwent 14 plate procedures in seven femurs and seven tibias for a 3.1-cm discrepancy at age 12.4 years. Patients were followed up to skeletal maturity, except two. The use of staples decreased the discrepancy in the bone ratio from +4.8% to +1.2% in two years, and the use of plates decreased this ratio from +5.1% to +3.3% in two years. The change in the length ratio was significantly greater after stapling. Six months were required after stapling before the first significant decrease in discrepancy; it took two years after plating.
Conclusions
This study showed a significantly lower efficacy for decreasing leg-length discrepancy by tension band plating. Orthopaedic surgeons should be aware of the limitations of using plates for suppressing bone growth.
Level of Evidence
III
Background
Leg-length discrepancy (LLD) is a common orthopaedic problem that can lead to standing imbalance, running injuries, low back pain, stress fractures and osteoarthritis of the hip. 1 In general, treatments to equalize leg length are limb shortening for smaller LLDs and limb lengthening for larger LLDs. 2 Limb shortening is often accomplished by epiphysiodesis, either permanent or temporary. Permanent epiphysiodesis is ablation of the epiphyseal plate to stop bone growth. 3 It is an irreversible procedure, and over-shortening is possible.4–9 A satisfying result depends on the exact time of stopping bone growth. Temporary epiphysiodesis suppresses bone growth through implants rather than through permanent ablation of the physis. The growth suppression can be adjusted by removing the implants once the treatment goal has been achieved.
Several implants have been used in temporary epiphysiodesis, and the therapeutic results have been variable.3,10–17 The use of percutaneous transphyseal screws is a quick and minimally invasive procedure. 11 However, bone bar formation after removing the transphyseal screw is a concern, and risks of valgus change of the tibia have been reported. 12 Staples have been reliably and effectively used in the treatment of epiphysiodesis since a report by Blount and Clarke in 1949. 13 Staple backout and subsequent mechanical deviation are not uncommon. 14 The applicability of tension band plating for growth tethering has been proven in an animal model. 10 Although with few implant-associated complications, the effects from tension band plating were unpredictable. 17
There are few studies that compare the efficiency of decreasing LLD using different implants. Lykissas et al 18 compared plates, staples and transphyseal screws in terms of decreasing LLD. No significant difference was reported among the three implants, but children who underwent stapling were significantly older than those who underwent plating. As age is an important factor in growth potential and efficiency of growth tethering, we conducted a study to test a null hypothesis that epiphysiodesis with plates had a comparable efficacy to that with staples in patients of similar ages.
Materials and methods
Staples were the standard implants for epiphysiodesis in the Chang Gung Memorial Hospital, Taiwan until 2010, as the manufacturer no longer supplies staples. After 2010, with tension band plates gaining popularity for modifying skeletal growth, we used stainless steel plate-screw constructs for temporary epiphysiodesis. This retrospective study reviewed children with LLD who were treated by temporary epiphysiodesis using plates or staples. To control the age at operation, we only included children who underwent epiphysiodesis between the ages of ten and 14 years and had more than two years of follow-up. Children who had LLD from skeletal dysplasia or metabolic diseases were excluded. The study was approved by the institutional review board in the authors’ hospital.
Surgeries
The epiphysiodesis surgeries were performed at the distal femur or proximal tibia between 2008 and 2012. In patients who underwent stapling, one to two staples were used at the medial and lateral sides of a physis. We used one to two staples in each condyle to fit the body sizes of the Asian children. The staples were manufactured by Smith-Nephew (Memphis, Tennessee) (Fig. 1). In patients who underwent tension band plating, one stainless steel plate and two screws were fixed at the medial and lateral sides of a physis. 19 The stainless steel plates were manufactured by Synthes (West Chester, Pennsylvania) (Fig. 2). No physis ablation, curettage or excision was done with the implantation operation.
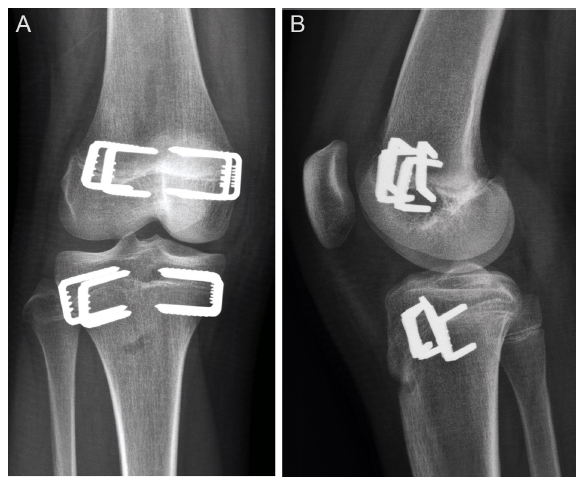
Temporary epiphysiodesis using staples.
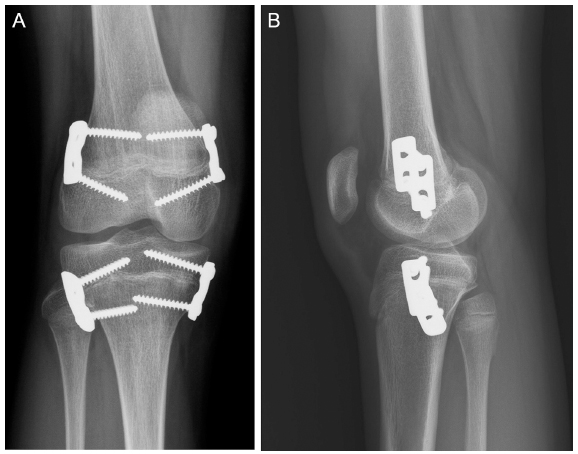
Temporary epiphysiodesis using plates.
Outcome assessment
After surgery, patients were followed up at six months and one year and then yearly. Leg length was assessed by a scanogram, and images were measured using the electronic picture archiving and communications system. Films were calibrated for measurement of distances, and measurements were performed with the built-in software. The LLD was recorded as exact length and length ratio. Length ratio was the bone length of the epiphysiodesis side divided by the length of the other side. Length ratio was 1.0 when the bone length was equal to the other. The efficiency of epiphysiodesis was assessed by the decrease of bone length and length ratio after the operation. The use of length ratio was to prevent the confounding of different body heights and growth rates among patients.
Statistical analysis
For comparison between patients who underwent stapling and those who underwent plating, background data of age at operation, sex, side, location of epiphysiodesis, initial LLD, follow-up duration and latest LLD were compared using the independent t-test for continuous variables and chi-squared test for nominal variables. Efficacy of epiphysiodesis was assessed by the decrease in discrepancy in the operated femur or tibia, and the efficacy was compared between the stapling and plating groups at six months, one year and two years postoperatively using the independent t-test. In assessing the time when the first significant reduction in discrepancy occurred, the paired t-test was used to compare between preoperative and postoperative conditions. A p-value of less than 0.05 was defined as statistically significant.
Results
In all, 19 patients, six boys and 13 girls, underwent 27 temporary epiphysiodesis surgeries in the study period. Eight patients received simultaneous operations at the ipsilateral femur and tibia. The causes of LLD included congenital short femur, fibular hemimelia, osteonecrosis after surgery for developmental dysplasia of the hip, traumatic physis injury, neonatal osteomyelitis, hemihypertrophy, idiopathy, radiation therapy for rhabdomyosarcoma and Legg-Calvé-Perthes disease (Table 1). They had operations at a mean age of 12.1 years (10.0 to 13.8 years) for an LLD of 2.9 cm and were followed up for 4.1 years on average. Physis closure occurred in all except two patients at the latest follow-up.
Demographic data of patients
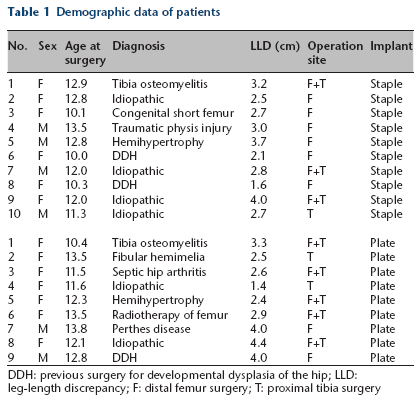
DDH: previous surgery for developmental dysplasia of the hip; LLD: leg-length discrepancy; F: distal femur surgery; T: proximal tibia surgery
Ten patients underwent stapling in nine femurs and four tibias at the age of 11.8 years for LLD 2.8 cm. Three patients had simultaneous stapling in the femur and tibia. The other nine patients underwent plating in seven femurs and seven tibias at the age of 12.4 years for LLD 3.1 cm. Five patients had simultaneous plating in the femur and tibia. The age at operation, location of epiphysiodesis and initial LLD were comparable between the two groups of children (Table 2).
Comparison of the patients treated with staples and those treated with plates. Data are presented as mean (sd)
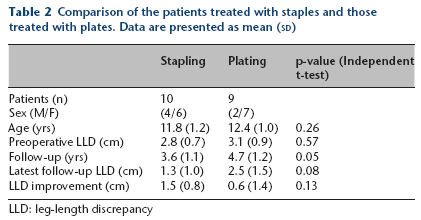
LLD: leg-length discrepancy
In the assessment of therapeutic efficacy between stapling and plating, the following analysis was conducted by length ratio of the operated femur or tibia rather than the whole leg length. The 13 staplings in nine femurs and four tibias decreased the bone length discrepancy from +1.72 cm (+4.8%) to +0.49 cm (+1.2%) in two years. The 14 platings in seven femurs and seven tibias decreased the bone length discrepancy from +1.90 cm (+5.1%) to +1.26 cm (+3.3%) in two years. The change of length ratio was significantly greater in the stapling group at two years (-3.6% by stapling versus -1.8% by plating, p < 0.05) (Fig. 3). The paired t-test between preoperative and postoperative length discrepancy showed that stapling produced the first significant decrease of discrepancy at postoperative six months (p = 0.036) and plating required two years to produce a significant decrease of discrepancy (p = 0.008) (Table 3).
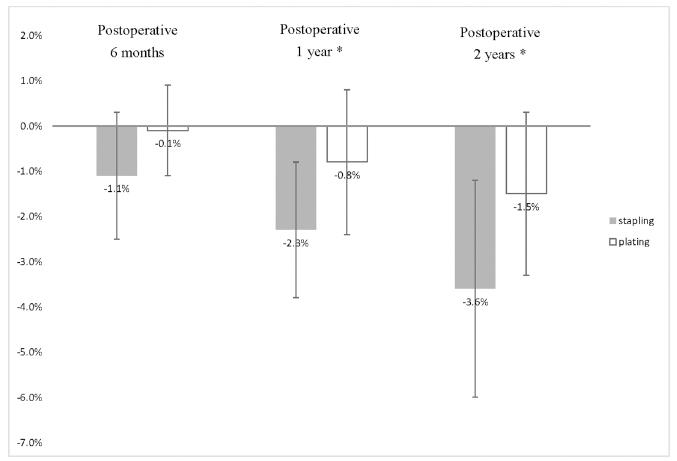
Change in the length ratio in the stapling group and plating group.
Length discrepancy in operated femurs or tibias. Data are presented as mean (sd).
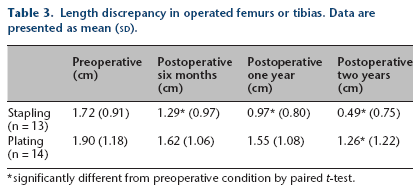
significantly different from preoperative condition by paired t-test.
With regard to the complications associated with the implants, no wound infection, implant loosening, limited knee movement or knee pain was noted in either group. Varus knee deformity occurred in two patients after femoral stapling and one patient after femoral plating. The problem was relieved by removing the implants from the medial femoral condyle. One patient with the sequel of septic hip underwent femoral plating for a 3.0-cm discrepancy at the age of 11.5 years. The discrepancy increased to 3.3 cm two years after plating, and the patient underwent lesion side femoral lengthening at the age of 14 years.
Discussion
The study results disproved the hypothesis that plating had the same efficacy in decreasing LLD as stapling. Stapling offered greater reduction of bone length and a quicker response to achieve a significant change. The implant-related complications were similar between staples and plates. With regard to the therapeutic efficacy and safety in temporary epiphysiodesis, staples were superior to plates.
Staples and plates shared a similar structure, which fixed the distance between the two anchors in the metaphysis and epiphysis. Cellular activity of the physis was suppressed by the two fixed-distance anchors, and skeletal growth was changed. 20 The guided growth plates were designed to act as a ‘tension band’ that placed the centre of rotation outside the bone.21,22 Therefore, plates provided a faster angular deformation with less inhibition of bone growth at the central part of a physis.23,24 The advantage of greater angular correction became a less favoured feature in reducing longitudinal bone growth. An inferior efficacy of plating in epiphysiodesis was reported when compared to physis ablation. 25
A previous study reported comparable effectiveness in correcting LLD with plates, staples and transphyseal screws. 18 This study showed different results between plates and staples. The two papers are retrospective reviews of patients with LLD from a variety of aetiologies. Lykissas et al 18 measured whole leg length after epiphysiodesis at the femur and the tibia simultaneously, and therapeutic efficacy was evaluated by the change in leg length per year. This study measured isolated bone length of the femur or tibia because epiphysiodesis was performed as per the individual patient requirements. Age might be the underlying factor for the differences in results between the two studies. Epiphysiodesis at an age before the adolescent growth spur can achieve a greater correction. For the patients of the age of 13.4 years who underwent stapling in Lykissas's study, the efficacy of stapling could be reduced by a lower growth potential at an older age. Recently, the authors of one case series reported poor results from the use of eight plates to stop skeletal growth. 26 We completely agree with the report and want to offer further evidence from a comparative study that reported against using plates in treating LLDs.
Some complications associated with the implants used in growth tethering surgery have been reported, including stress fractures, infection, changes in alignment, implant fracture, iatrogenic permanent physeal arrest, rebound overgrowth and intraarticular migration.12,14,27,28 In our series, the most common complication was varus deformity after epiphysiodesis at the distal femur. In the stapling group, two cases of varus knee deformity were observed after nine femoral staplings, whereas in the plating group, one varus deformity was noted after seven femoral platings. The knee alignment could be restored to neutral after removing the medial implants without further osteotomy. Proximal migration of the implants was more common in the plating group and may have led to cutting through the growth plate and asymmetric growth inhibition. This is one of the weaknesses of temporary epiphysiodesis via plating and can lead to asymmetric growth tethering and premature closure of the physis. A rebound phenomenon was observed in a few patients after staple removal, and premature physis closure did not occur in this case series. Subsequent growth after removing implants is unpredictable in the temporary epiphysiodesis. Besides, relative central overgrowth of the physis after using tension band plates, the so-called ‘volcano-effect’, was observed in this case series, especially in the young children. Although no knee pain or ambulation problems were reported by the patients or their parents, the long-term effects of this phenomenon will require further follow-up.
There were several limitations in evaluating the efficacy of epiphysiodesis in this study. The variety in the aetiologies of LLDs produced different rates of increase in discrepancy. This factor confounded the efficacy of epiphysiodesis that was evaluated by the decrease in discrepancy. This study combined epiphysiodesis at the distal femur and the proximal tibia, which have different growth rates. The case number was not sufficient for further splitting to the femur and tibia. Although the chronological age was comparable between the two groups, the skeletal age was not available for all patients. However, during the two-year postoperative follow-up period, the physis was still open in all cases. Besides the above factors, growth rate could be different among patients with different body lengths, parental factor and sex. For a clinical study, it is not easy to control for the velocity of skeletal growth since it is multi-factorial.
Since Blount and Clarke 13 presented their early results with epiphyseal stapling in 1949, this method of epiphysiodesis has remained popular in treating LLD. We used staples and plates for temporary epiphysiodesis before and after 2010. This retrospective review showed longer latency and lower efficacy in decreasing LLD on using tension band plating. Orthopaedic surgeons should be aware of the limitations of a tension band plate in deceasing bone growth. A new generation of staples or plates with fixed angle screws are expected to help children with minor LLD.