
Abstract
Abstract
Purpose
The Blount staple has been widely used for treating angular deformities and leg length discrepancy (LLD) of the lower limbs. In recent years, the Eight plate has replaced the Blount staple for treating angular deformities in many centres. Although not described in the literature, it has been proposed that the Eight plate could also be used for treating LLD. We studied the effectiveness of the device for this indication.
Methods
Ten patients with LLD were included prospectively. Medial and lateral plates were inserted for symmetrical growth reduction and the patients were followed by radiostereometric analysis (RSA) 0, 3, 6, 9, 12, 24, 52 and 80 weeks postoperatively. The error of measurement with this technique is less than 0.05 mm.
Results
Case 1 continued to grow an average of 0.08 mm per week (6.7 mm longitudinal growth in 1.5 years) postoperatively, while Case 2 showed 0.07 mm longitudinal growth per week (5.6 mm longitudinal growth in 1.5 years). The longitudinal growth, in both children, showed only slight growth retardation throughout the follow-up period. The study was interrupted and no further subjects were included after the results indicated that only minor growth reduction had occurred in both patients.
Conclusion
The Eight plate does not significantly reduce growth when applied both medially and laterally in a symmetrical way at the proximal tibial physis.
Introduction
Several surgical procedures have been described for treating mild leg length discrepancy (LLD) [1–7], all of which have the disadvantage of being more or less irreversible, accomplishing total physeal arrest. The outcome of physiodesis with irreversible methods depends on correctly estimating the age of maturity and the final LLD or leg length. It has been shown that current methods of outcome estimation of physiodesis yield significant uncertainty [8, 9].
Several complications have been described with use of Blount staples for treating both angular deformities and LLD [2, 10–15]. A new device, introduced by Dr. Peter M. Stevens [16] and commonly referred to as the Eight plate, has, in many centres, replaced Blount staples for treating angular deformities in the lower limb, with good results. It has been claimed that one of the advantages of this device is that it does not cause physeal arrest and can, therefore, be removed, resulting in regained physeal growth in the area where it was originally inserted [16].
We hypothesized that placing the Eight plate both medially and laterally over the physis should, theoretically, reduce longitudinal physeal growth without damaging the physis. The need for accurate prediction would, consequently, not be critical, since the device could be removed once equality in leg length had been obtained. However, it was important that the primary operation should not be performed too late. It would be possible to treat LLD at an earlier age, not necessarily according to the age of maturity. Our hypothesis was that placing the Eight plate both medially and laterally over the physis would result in symmetrical growth retardation.
Materials and methods
Approval for the study and for ten patients to be included was granted by the local ethics committee. The subjects’ parents gave written consent for their child to be included. Scanograms were performed preoperatively for measuring LLD. Radiostereometric analysis (RSA) was used to determine the three-dimensional skeletal dynamics of the epiphysis relative to the metaphysis, which expressed the rate of growth retardation [17]. To facilitate radiostereometric follow-up with segment motion analysis, tantalum balls with a diameter of 0.8 mm were inserted percutaneously with a stainless-steel cannula with bevelled tip and a hand-operated piston. Three medial and three lateral markers were inserted in a triangular pattern in both the metaphysis and the epiphysis (e.g. on both sides of the growth plate) in a triangular pattern. RSA was used to determine the three-dimensional skeletal dynamics of the epiphysis relative to the metaphysis, which expressed the rate of growth retardation. Each RSA examination was performed with the patient in the supine position by using two 90° angulated roentgen tubes, facilitating simultaneous exposures of the knee with the implanted 0.8-mm tantalum markers, and a combined reference and calibration device with similar tantalum markers placed at known positions, on two separate unipolar films. The two-dimensional distances between the images of the tantalum markers on the two films provided the input data for computerised conversion to a three-dimensional coordinate system using the Kinema software (RSA BioMedical Innovations AB, Umeå, Sweden). Thereafter, the three-dimensional dynamics of growth retardation between consecutive RSA examinations could be calculated.
RSA was performed postoperatively and after 3, 6, 9, 12, 24, 52 and 80 weeks, at similar intervals as applied in an earlier study measuring the rate of growth retardation after percutaneous physiodesis [18]. Two children, one boy and one girl both aged 11 years, were fitted with a medial and lateral Eight plate at the proximal tibial physis. Figure 1a shows typical growth retardation of the proximal tibia after percutaneous physiodesis. The error of measurement with the RSA technique is less than 0.05 mm [18].
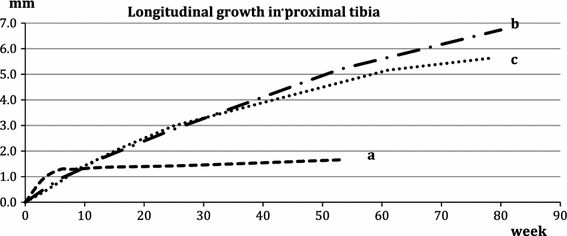
Longitudinal growth of the proximal tibia, measured using radiostereometric analysis (RSA). a Typical growth retardation of the proximal tibia after percutaneous physiodesis, b Case 1 and c Case 2
Case 1 was an 11-year-old boy who had been treated for a neuroblastoma with multiple metastases at the age of 1 year. He had been treated with chemotherapy and extirpation of the primary tumour from the adrenal gland. Relapse had been diagnosed at the age of 5 years, with metastasis in the left proximal tibia, and was treated with radiotherapy. In the following 3 years, the boy had sustained two fractures in the proximal tibia. The left proximal tibial physis had shown signs of growth retardation, probably as a consequence of the radiation treatment. At 11 years of age, the left tibia was 5.5 cm shorter than the right tibia. The patient was treated with a medial and lateral Eight plate on the right proximal tibia to reduce the amount of lengthening necessary of the left tibia (Figs. 1 and 2).
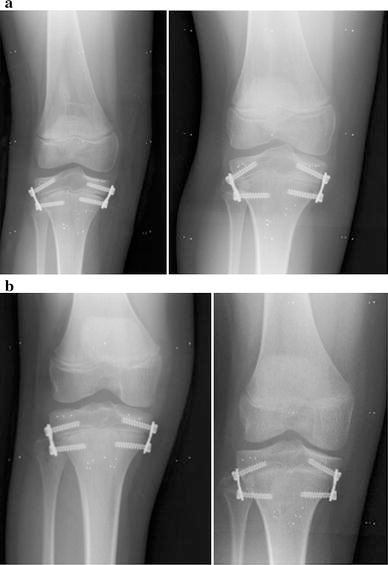
Case 2 was an 11-year-old girl with expected small stature (162 cm) and an LLD of 3.9 cm, with a 2.9-cm difference in the length of the tibiae (Figs. 1 and 2). Treatment with an Eight plate was chosen to diminish the difference without creating a permanent physiodesis.
Results
Case 1 had 0.08 mm longitudinal growth per week postoperatively (6.7 mm longitudinal growth in 1.5 years). The LLD after 1 year was 6.0 cm, measured by computed tomography (CT) scanogram. Case 2 had 0.07 mm longitudinal growth per week (5.6 mm longitudinal growth in 1.5 years). The LLD after 1 year was 4.0 cm, measured by CT scanogram.
The longitudinal growth rate in both children showed only slight growth retardation throughout the follow-up period (Fig. 1). As a consequence of the results obtained with the first two cases, the study was terminated.
Discussion
The theoretical idea of performing reversible physiodesis is attractive. In contrast to existing methods, the uncertainty for predicting final LLD at maturity would be of minor importance with this treatment. The correction could be performed at a younger age and more than once during the growth period. It would be possible to achieve better final results than that obtained with conventional techniques.
The results obtained for the two patients included in the study showed only slight growth retardation during the first 1.5 years postoperatively. The growth curves (Fig. 1b, c) were somewhat steeper during the first 12 weeks. This may imply a small effect of the Eight plate after 12 weeks, but it could also be a result of stimulation of growth, after drilling for the two screws, in the early phase after physiodesis. Extrapolating the curve in relation to the first 12 weeks as the real growth potential would not imply more than approximately 3 mm of growth retardation during 1 year. It would, as a consequence, take at least 3 years to correct an LLD of 1 cm if this was the case. The longitudinal growth was approximately 5 mm at 1 year, which is the amount of growth expected without intervention. After 1 year, the longitudinal growth in Case 2 (Fig. 1c) tended to slow down. This is, however, expected for girls aged nearly 13 years at the end of the study period reaching skeletal maturity. In an earlier study [18], we found that longitudinal growth after proximal percutaneous physiodesis of the tibia ended after less than 12 weeks. Theoretically, the longitudinal growth rate could diminish further after the 1.5-year study period and as a consequence of screws diverging maximally. If this was the case, the method must be described as unpredictable. Furthermore, it creates two problems. Firstly, the screws must reach maximum splay at the same time so as not to create an angulation by asymmetrical growth retardation. Secondly, there is a risk for permanent physiodesis when leaving the plate in place for more than 18–24 months. The Eight plate has proven effective for correcting angular deformities. The Eight plate in these cases serves as an extraperiosteal hinge. Placing the Eight plate both medially and laterally seems to allow for central physeal growth.
We terminated the study early, and decided to include no further subjects, because no significant effect was seen on longitudinal growth during 1.5 years. We cannot recommend the Eight plate for treating LLD. Both patients described are now planned to undergo lengthening of the short tibia with callus distraction in due course.
Footnotes
None.