
Abstract
Abstract
Purpose
This study was performed to investigate leg-length discrepancy (LLD) and associated risk factors after paediatric femur shaft fractures.
Methods
A total of 72 consecutive patients under 13 years old (mean age 6.7 years; 48 boys, 24 girls) with unilateral femur shaft fracture, and a minimum follow-up of 18 months, were included. The amount of LLD was calculated by subtracting the length of the uninjured from that of the injured limb. Risk factors for an LLD ≥ 1 cm and ≥ 2 cm were analyzed using multivariable logistic regression analysis.
Results
Hip spica casting, titanium elastic nailing and plating were performed on 22, 40 and ten patients, respectively. The mean LLD was 7.8 mm (sd 8.8) and 29 (40.3%) had a LLD of ≥ 1 cm, while nine (12.5%) had a LLD of ≥ 2 cm. There were significant differences in fracture stability (p = 0.005) and treatment methods (p = 0.011) between patients with LLD < 1 cm and ≥ 1 cm. There were significant differences in fracture site shortening (p < 0.001) and LLD (p < 0.001) between patients with length-stable and length-unstable fractures. Fracture stability was the only factor associated with LLD ≥ 1 cm (odds ratio of 4.0; p = 0.020) in the multivariable analysis.
Conclusion
This study demonstrated that fracture stability was significantly associated with LLD after paediatric femur shaft fractures. Therefore, the surgeon should consider the possibility of LLD after length-stable femur shaft fracture in children.
Level of Evidence
Prognostic level III
Introduction
Femoral shaft fractures represent about 1.6% of all paediatric fractures, and occur in a bimodal distribution with peaks during the toddler and early adolescence stages. 1 Treatment methods for paediatric femoral shaft fractures include Pavlik harness, immediate or delayed hip spica casting, external fixation, flexible or rigid intramedullary nailing and plate fixation. The method depends on the patient's age, weight, fracture pattern and the surgeon's preference.2–11
The most common sequela after a paediatric femoral shaft fracture is leg-length discrepancy (LLD) owing to overgrowth of the injured femur. Many studies have investigated the biomechanical effects of LLD, and reported low back pain, hip pain and stress fractures to be musculoskeletal disorders associated with LLD.12–14 Most of the overgrowth has been shown to occur within the first 18 months following the fracture.15–17 It is believed that this is due to a physiological process associated with post-traumatic activation of the growth plate. 18 The mean overgrowth is approximately 1 cm and thus a proper amount of bayonet apposition is required for hip spica casting in young children.
Several studies have investigated the factors affecting overgrowth after paediatric femoral shaft fracture.16,17,19–23 Age, fracture site, fracture stability, degree of overlap and nail-canal diameter (NCD) ratio have been suggested as risk factors for femoral overgrowth. However, there are a lack of studies analyzing the risk factors for LLD after a paediatric femoral shaft fracture. Therefore, we performed this study to investigate the LLD after a paediatric femur shaft fracture and its associated risk factors.
Materials and methods
This retrospective study was approved by the institutional review board of our hospital. Informed consent was waived due to the retrospective design of this study.
Study population and data collection
Consecutive patients with a unilateral femur shaft fracture who were < 13 years old and had a minimum follow-up of 18 months at three institutions were included in this study. The exclusion criteria were as follows: 1) bilateral femur shaft fracture; 2) ipsilateral or contralateral lower limb fractures; or 3) pathological fracture due to cerebral palsy, bone tumour or osteogenesis imperfecta.
From the medical record review, the following information was obtained: sex, age, height, weight, body mass index (BMI), follow-up duration, side of limb, range of movement of the hip and knee joints, injury mechanism and treatment method. Injury mechanisms were divided into high-energy and low-energy injuries. We defined traffic accidents, sports injury and a fall from a height as high energy injuries, and slipping and falling from ground-level as low energy injuries. All fractures were treated by four paediatric orthopedic surgeons (MSP, SHL, KHS and TGK). Treatment methods included hip spica casting, titanium elastic nailing (TEN) and plating.
Radiographic measurements
From the preoperative anteroposterior (AP) and lateral radiographs of the injured femur, fracture location and fracture stability were determined. Fracture locations were classified as proximal third, middle third and distal third. Fractures were divided into length-stable and length-unstable fractures according to fracture stability. Transverse and short oblique fractures were classified as length-stable fractures; and long oblique, spiral, and comminuted fractures were classified as length-unstable fractures. Long oblique fractures were defined when the angle between the fracture line and a line perpendicular to the long axis of the femur was > 30°. Fracture-site shortening was measured from the postoperative AP and lateral radiographs of the femur.
To assess the limb length, the AP standing long-cassette radiographs of the lower extremity (teleroradiogram) were taken using a UT 2000 x-ray machine (Philips Research, Eindhoven, The Netherlands) at a source-to-image distance of 200 cm, and set at 50 kVp and 5 mAs with the patella facing forward. It consisted of a single radiographic exposure of both lower limbs, with the x-ray beam centred at the knee. Until two years after the trauma, a teleradiogram was taken regularly once per year. Thereafter, if the LLD was ≥ 1 cm, a teleradiogram was recommended to be regularly performed once every one to two years. Otherwise, a regular examination was decided according to the parents’ need. The radiographic images were retrieved using a picture archiving and communication system (PACS) (IMPAX; Agfa Healthcare, Mortsel, Belgium), and radiographic measurements were performed using PACS software. The whole limb length (WLL) was measured from the teleroentgenograms of the final follow-up. The WLL was defined as the length from the top of the femoral head to the center of the tibial plafond (Fig. 1).
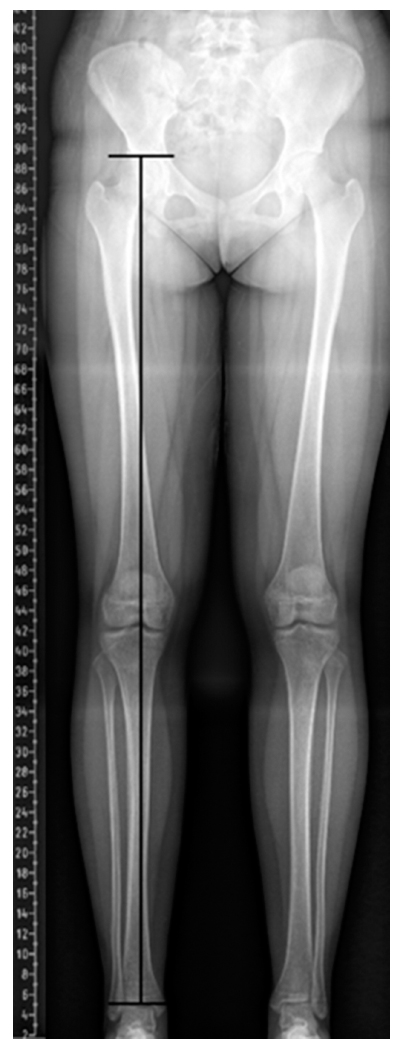
Whole limb length was defined as the length from the top of the femoral head to the center of the tibial plafond.
Before the main measurement, inter-observer reliability testing was performed for the WLL measurements. Two orthopaedic surgeons (KJC and BI) with six and four years of experience, respectively, independently measured the WLLs for 15 radiographs. After reliability testing, one of the authors (BI) measured all radiographic measurements.
The amount of LLD was calculated by subtracting the uninjured limb length from the injured limb length. Overgrowth was calculated by adding the fracture site shortening to the LLD. In order to investigate the risk factors for LLD, patients were divided into those with a LLD of < 1 cm or ≥ 1 cm according to Flynn's criteria 24 and those with an LLD of < 2 cm or ≥ 2 cm.
Statistical analysis
Reliability was assessed by the intraclass correlation coefficient (ICC) and 95% confidence interval (CI) in the setting of a two-way random-effect model, assuming a single measurement and absolute agreement. 25 With a target ICC value of 0.9 and 95% CI width of 0.2 for two observers, the minimal sample size was determined to be 15 radiographs using Bonett's methods. 26
To summarize patient demographics, descriptive statistics such as mean and sd were used. The chi-squared test or Fisher's exact test, and independent t-test or Mann-Whitney U test were used for comparisons of variables between groups. Multivariable logistic regression analysis was used to identify the risk factors for LLD after a paediatric femur shaft fracture after univariable analysis. Variables with a p-value < 0.1 in the univariable analysis were included in the multivariable analysis. All statistical analyses were conducted with SPSS software for Windows (Version 25.0; SPSS Inc, Chicago, Illinois). All statistics were two-tailed and p-values of < 0.05 were considered statistically significant.
Results
In total, 98 patients with a femur shaft fracture who were < 13 years old were screened. After implementation of the exclusion criteria, a total of 72 patients remained in this study of which 48 were boys and 24 were girls (Fig. 2). The mean age of the patients at the time of injury was 6.7 years (sd 2.9). There were 43 length-stable and 29 length-unstable fractures. The mean follow-up duration was 3.8 years (sd 2.7). Hip spica casting was performed on 22 patients, TEN on 40 patients and plating on ten patients. Mean LLD and mean overgrowth were 7.8 mm (sd 8.8; 95% CI 5.7 to 9.8) and 12.0 mm (sd 8.2; 95% CI 10.2 to 14.0), respectively. Of the 72 patients, 29 (40.3%) had a LLD of ≥ 1 cm and nine (12.5%) had a LLD of ≥ 2 cm (Table 1). Of these nine patients, four underwent additional surgeries for the correction of LLD at a mean interval of 3.5 years after initial surgery. Three boys underwent epiphysiodesis of the distal femur at the ages of 12.8, 13.0 and 10.3 years, respectively, and one girl underwent femoral lengthening of contralateral side using an Ilizarov external fixator at the age of 12.2 years. None of the patients had flexion contracture of the hip or knee joints.
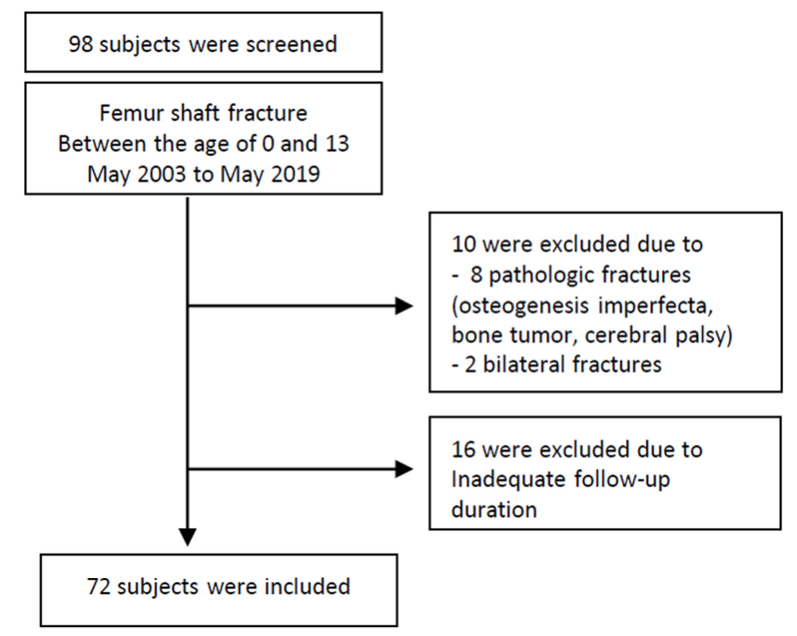
Inclusion and exclusion criteria.
Summary of patient demographics
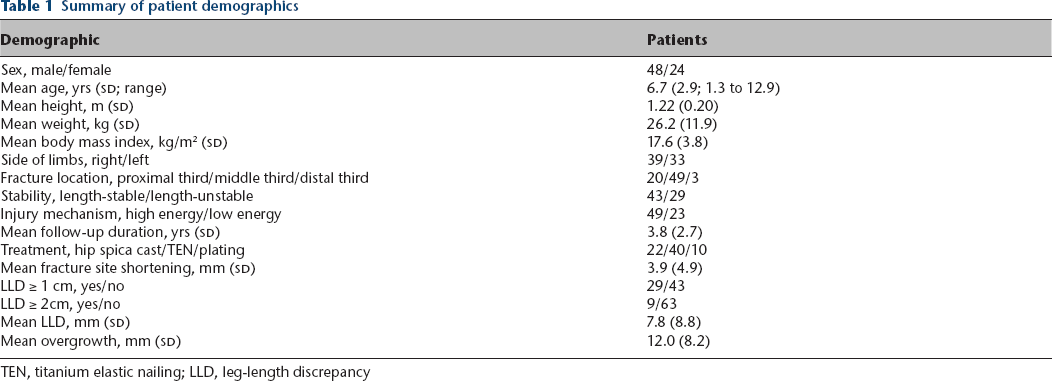
TEN, titanium elastic nailing; LLD, leg-length discrepancy
Radiographic measurements for WLL showed excellent interobserver reliability (ICC 0.958; 95% CI 0.886 to 0.983).
There were significant differences in fracture stability (p = 0.005) and treatment methods (p = 0.011) between patients with LLDs < 1 cm and ≥ 1 cm. However, there were no significant differences in sex, age, BMI, fracture location, follow-up duration and injury mechanism between the two groups. There were no significant differences in any variable between patient with LLDs < 2 cm and ≥ 2 cm (Table 2).
Comparison of variables between patients with LLD < 1 cm and ≥ 1 cm, and patients with LLD < 2 cm and ≥ 2 cm
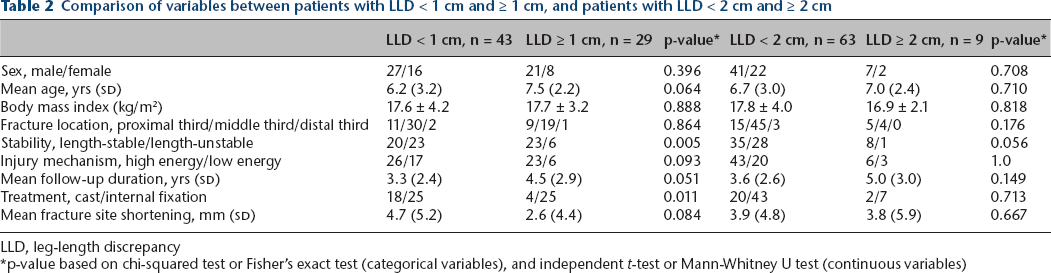
LLD, leg-length discrepancy
p-value based on chi-squared test or Fisher's exact test (categorical variables), and independent t-test or Mann-Whitney U test (continuous variables)
There were significant differences in fracture site shortening (p < 0.001), and LLD (p < 0.001) between patients with length-stable and those with length-unstable fractures. However, there were no significant differences in sex, age, BMI, fracture location, injury mechanism, follow-up duration, treatment methods and overgrowth between the two groups (Table 3).
Comparison of variables between length-stable and length-unstable fractures
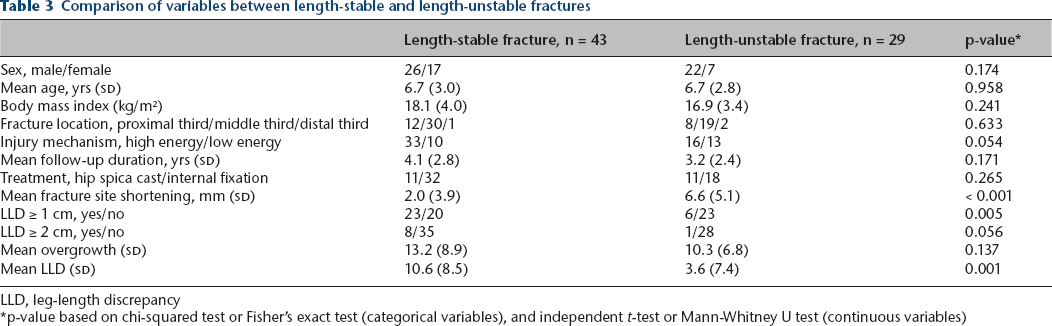
LLD, leg-length discrepancy
p-value based on chi-squared test or Fisher's exact test (categorical variables), and independent t-test or Mann-Whitney U test (continuous variables)
Patients treated with hip spica cast showed a younger age and a greater degree of fracture site shortening than those treated with TEN and plating (all p < 0.001). LLD in patients treated with hip spica cast (4.2 mm) was smaller than that in those treated with TEN (9.2 mm) and plating (10.5 mm), but the difference was not statistically significant (p = 0.055). The degree of overgrowth did not differ according to treatment modality (Table 4).
Comparison of variables between patients who underwent hip spica cast, titanium elastic nailing (TEN) and plating
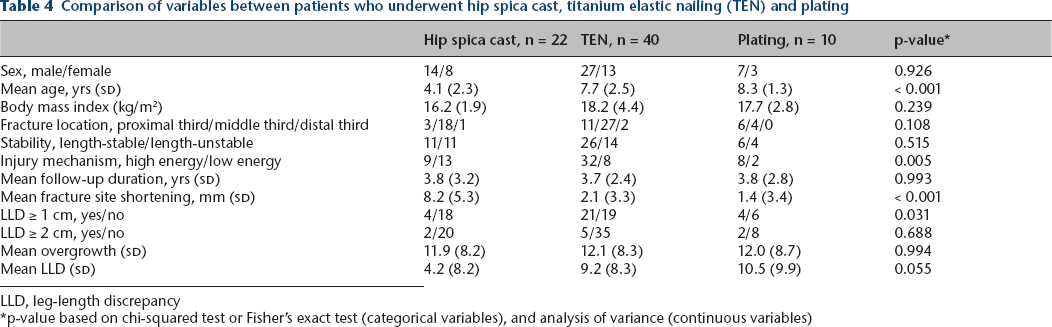
LLD, leg-length discrepancy
p-value based on chi-squared test or Fisher's exact test (categorical variables), and analysis of variance (continuous variables)
After univariable analysis, age, fracture stability, follow-up duration and treatment methods were included in a multivariable logistic regression analysis. Fracture stability was the only factor that was found to be associated with an LLD of ≥ 1 cm after paediatric femur shaft fracture (p = 0.020). Patients with length-stable fractures had 4.0 times higher risk of LLD ≥ 1 cm (Table 5). However, no significant risk factors were found to be associated with LLD ≥ 2 cm in the multivariable logistic regression analysis (Table 6).
Risk factors for leg-length discrepancy (≥ 1 cm) after paediatric femur shaft fracture
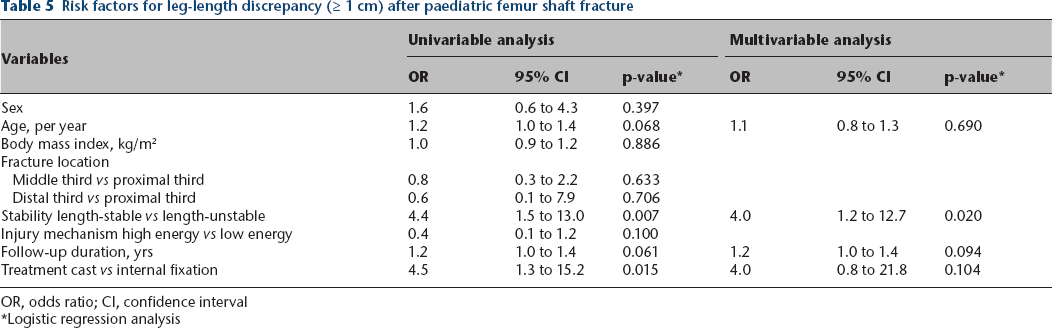
OR, odds ratio; CI, confidence interval
Logistic regression analysis
Risk factors for leg-length discrepancy (≥ 2 cm) after paediatric femur shaft fracture
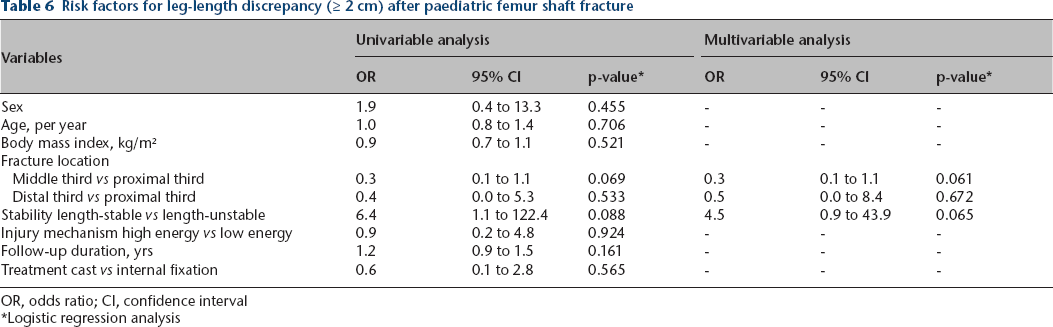
OR, odds ratio; CI, confidence interval
Logistic regression analysis
Discussion
LLD due to femoral overgrowth following a femur shaft fracture in children is a well-known phenomenon. If the LLD exceeds or is expected to exceed 2 cm to 2.5 cm at skeletal maturity, length equalization procedures, such as epiphysiodesis or limb lengthening should be considered. 27 Therefore, it is clinically important to identify risk factors for LLD after a paediatric femur shaft fracture. This study demonstrated that LLD after paediatric femur shaft fractures was significantly associated with fracture stability.
A number of studies have reported overgrowth after paediatric femur shaft fracture and described the associated risk factors. Park et al 20 reported that a length-unstable fracture was a risk factor for overgrowth in patients who underwent TEN or submuscular plating. Dai et al 22 found that length-unstable fractures and low NCD ratios (< 0.8) were significantly associated with limb overgrowth after the application of TEN. Park et al 21 also showed that a low NCD ratio (< 0.8) was a risk factor for femoral overgrowth after TEN. Sulaiman et al 23 showed a strong negative correlation between age and femoral overgrowth following plate fixation. Stilli et al 17 also showed a greater amount of overgrowth in children younger than five years after conservative treatment. However, in this study there were no significant differences in any variables including sex, age, fracture location, fracture stability and treatment methods between patients with an overgrowth < 1 cm, and those with an overgrowth ≥ 1 cm. Nascimento et al 28 showed no significant difference in the amount of overgrowth between a TEN group and traction followed by cast group.
There have been few studies investigating LLD and its risk factors after paediatric femur shaft fracture. Hariga et al 29 assessed the LLD in 37 children treated by flexible intramedullary nailing or hip spica cast. They found that LLD was significantly associated with the degree of initial overlap, but not associated with sex, age, fracture type, fracture level or treatment methods. Mutimer et al 30 evaluated the LLD following flexible intramedullary nailing in 17 children. They showed statistically significant LLD (4.3 mm) after TEN in eight children of four to eight years, but no significant LLD (0.1 mm) in children over eight years.
In this study, fracture stability was a significant factor for LLD of ≥ 1 cm. Patients with length-stable fractures had a four-times higher risk of having an LLD ≥ 1 cm than those with length-unstable fractures. Moreover, among nine patients with LLD ≥ 2 cm, eight patients showed length-stable fractures. Length-stable fractures showed less fracture site shortening (2.0 mm) than length-unstable fractures (6.6 mm). However, there was no difference in overgrowth between length-stable and length-unstable fractures. Therefore, length-stable fractures appear to be associated with longer LLD than length-unstable fractures.
Patients who were treated by internal fixation using TEN or plating had a 6.2 mm longer LLD than those who were treated by hip spica cast. Hip spica cast is usually performed with overlapping the proximal and distal fragment of the fracture site. However, for surgical fixation, the goal of reduction is not a ‘bayonet apposition’, unlike a hip spica cast. Therefore, patients treated by casts had more fracture-site shortening than those who underwent an operation, which might result in this study's results. Among nine patients with a LLD ≥ 2 cm, five were initially treated by TEN, two by plating and two by hip spica casting. We think that some degree of shortening may be desirable to prevent LLD when performing internal fixation for paediatric femur shaft fractures.
There were some limitations to this study. Firstly, the minimum follow-up duration of our cohort was 1.5 years, which may affect the study outcomes. However, there was no significant difference in follow-up duration between patients with a LLD of < 1 cm and those with a LLD of ≥ 1 cm, or between patients with length-stable and those with length-unstable fractures. In addition, follow-up duration was not associated with LLD after paediatric femur shaft fractures. Further long-term follow-up studies are required. Secondly, we did not have radiographs before the injury; thus, we assumed that limb lengths were equal prior to fracture. Our cohort did not include patients with conditions that cause LLD, such as congenital limb deficiency, neuromuscular disease, tumour and idiopathic hemihypertrophy. Thirdly, our sample size was small, and a sample size estimation was not performed because of the retrospective design of this study. We could not identify the risk factors for LLD ≥ 2 cm because only nine patients had LLD ≥ 2 cm. Further studies with large cohorts are required to provide clinically meaningful information based on sample size calculations.
In conclusion, this study demonstrated fracture stability was significantly associated with LLD after paediatric femur shaft fractures. Therefore, the surgeon should consider the possibility of LLD after length-stable femur shaft fracture in children.
Footnotes
MSP: Study design, Study supervision.
SHL: Study design, Interpretation of data.
KJC: Performed measurements, Interpretation of data.
B-eI: Performed measurements, Interpretation of data.
DYK: Interpretation of data.
KHS: Study design, Interpretation of data, Manuscript preparation.