
Abstract
Purpose:
The purpose was to study radiographic and perceived leg length discrepancy after skeletal maturity in patients treated for femoral shaft fractures with elastic stable intramedullary nails in childhood.
Methods:
Thirty-five adults underwent standing radiographs and answered a questionnaire regarding perception of leg length discrepancy. Demographic data, fracture characteristics, angulation, stability of fixation, and callus formation, at time of fracture, were assessed.
Results:
Mean age at fracture was 10.2 (4.9–16.7) years, and mean follow-up time was 11.1 (3.8–16.8) years. In 8 of 35 participants, the fractured limb was 11–15 mm longer than the non-fractured, and in 16, 1–10 mm longer. In eight participants, the fractured limb was 1–10 mm shorter than the non-fractured, and in three participants, 12–23 mm shorter. The younger the child, the greater the lengthening (Rs = −0.49, p = 0.003). The greater the femoral angulation at time of fracture, the greater the shortening (Rs = 0.42, p = 0.013). There was no significant correlation between stability of fixation or callus formation 1 month postoperatively and radiographic leg length discrepancy after skeletal maturity. Fourteen (40%) had perception of leg length discrepancy at follow-up, of whom eight had a radiographic leg length discrepancy of 10–24 mm.
Conclusion:
Treatment with elastic stable intramedullary nail of femoral shaft fracture in childhood may result in radiographic leg length discrepancy. Younger children were more prone to lengthening and should possibly be assessed before skeletal maturity. The degree of fracture stability or callus formation at the time of fracture did not significantly affect leg length discrepancy. Perception of leg length discrepancy was not necessarily associated with a radiographic leg length discrepancy (≥10 mm).
Level of evidence:
level IV, case series.
Keywords
Introduction
The treatment of femoral shaft fractures in school-aged children has shifted from non-surgical to surgical with elastic stable intramedullary nails (ESINs).1–3 The principle of ESIN is to create a three-point support for each of two C-shaped nails, where the elasticity of the nails maintains load-sharing until the fracture is healed. 4 Although satisfactory results have been reported,5–8 the technique does not always provide sufficient stability, and may result in both shortening and lengthening, causing residual leg length discrepancy (LLD).9,10 Several studies have described LLD of ≥10 mm at follow-up after femoral shaft fractures treated with ESIN in children (Supplemental Appendix A).7,11–21 In the Flynn scoring criteria, LLD of <10 mm and angulation of ≤10° are considered an excellent result. 13 The degree of LLD that may cause pain, gait deviations, or other problems later in life is not clear. O’Brien et al. 22 described in normal subjects, a 10-mm difference as a threshold for perception of LLD. Previous studies, not related to pediatric femoral shaft fractures, state that LLD of more than 15–20 mm in adulthood can lead to low back pain and hip arthritis.23,24 The subjective experience and expected outcome of possible LLD may play a role in patient satisfaction. It was reported that the perception of LLD after total hip arthroplasty did not correlate with radiographic LLD ≥5 mm. 25 Perception of LLD in adults after a femoral shaft fracture in childhood is not known.
To estimate ESIN fixation stability, Lascombes et al. 26 introduced the nail to medullary canal ratio (NCD), comparing the nail diameter to the narrowest width of the medullary canal (isthmus); an NCD of at least 40% was recommended to provide sufficient stability. Park et al. 19 reported increased femoral growth in children treated with ESIN if the NCD was low. Instability during fracture healing may generate indirect bone healing with extensive callus formation. 27 Prolonged healing and the remodeling process may also lead to overgrowth, resulting in LLD. 28 Overgrowth after rigid intramedullary devices was first described by Blount in 1954 29 and the same phenomenon has been reported after external fixation, 30 plate fixation, 31 and by the Nancy group, when introducing the principle of ESIN. 7 Fracture malalignment with angulation may lead to LLD as well as a remaining fracture gap.
To the best of our knowledge, there are a few studies on LLD in skeletal maturity after pediatric femoral shaft fractures,32,33 and none after treatment with ESIN. Furthermore, there is a lack of literature evaluating the individuals’ perception of LLD and possible relation to radiographic LLD after pediatric femoral shaft fractures.
The aim was to study residual radiographic LLD in skeletal maturity after treatment of femoral shaft fractures with ESIN in childhood, and associations with femoral angulation, fracture stability and callus formation during fracture healing. Furthermore, we wanted to explore if any subjective symptoms were associated with radiographic LLD.
Material and methods
Participants
In this cohort study, individuals with pediatric femoral shaft fractures between 1998 and 2014 were identified through the diagnosis registers in two regions of Sweden (Västra Götaland and Stockholm) using the diagnosis code for femoral shaft fracture (S72.3, International Classification of Diseases, ICD-10-SE) and the procedure code for intramedullary nailing of femur (NFJ59, NOMESCO Classification of Surgical Procedures). 34 Medical records were reviewed by one of the authors (M.F.) to confirm the diagnosis and treatment in childhood and the eligibility to participate. Inclusion criteria were femoral shaft fracture with open femoral physes at the time of surgery, treatment with ESIN, and available pre-, peri-, or immediate postoperative radiographs and radiographs during the healing period. Exclusion criteria were other previous or concomitant fractures of the lower extremities, conditions that could affect growth and remodeling, re-fractures, or repeated surgery of the index fracture other than planned extraction of the elastic nails.
One hundred sixty-three individuals were identified and invited to participate. Eighty-five responded and accepted participation; 18 of the 85 were excluded due to other injuries or medical conditions affecting growth or fracture treatment with semi-rigid nails, which has the same surgical code as ESIN. Sixty-seven were eligible and scheduled to visit the radiology department at one of two tertiary hospitals. Thirty-two of the 67 did not attend; thus, 35 participants underwent a radiographic examination and, at the same visit, answered a questionnaire (Figure 1).
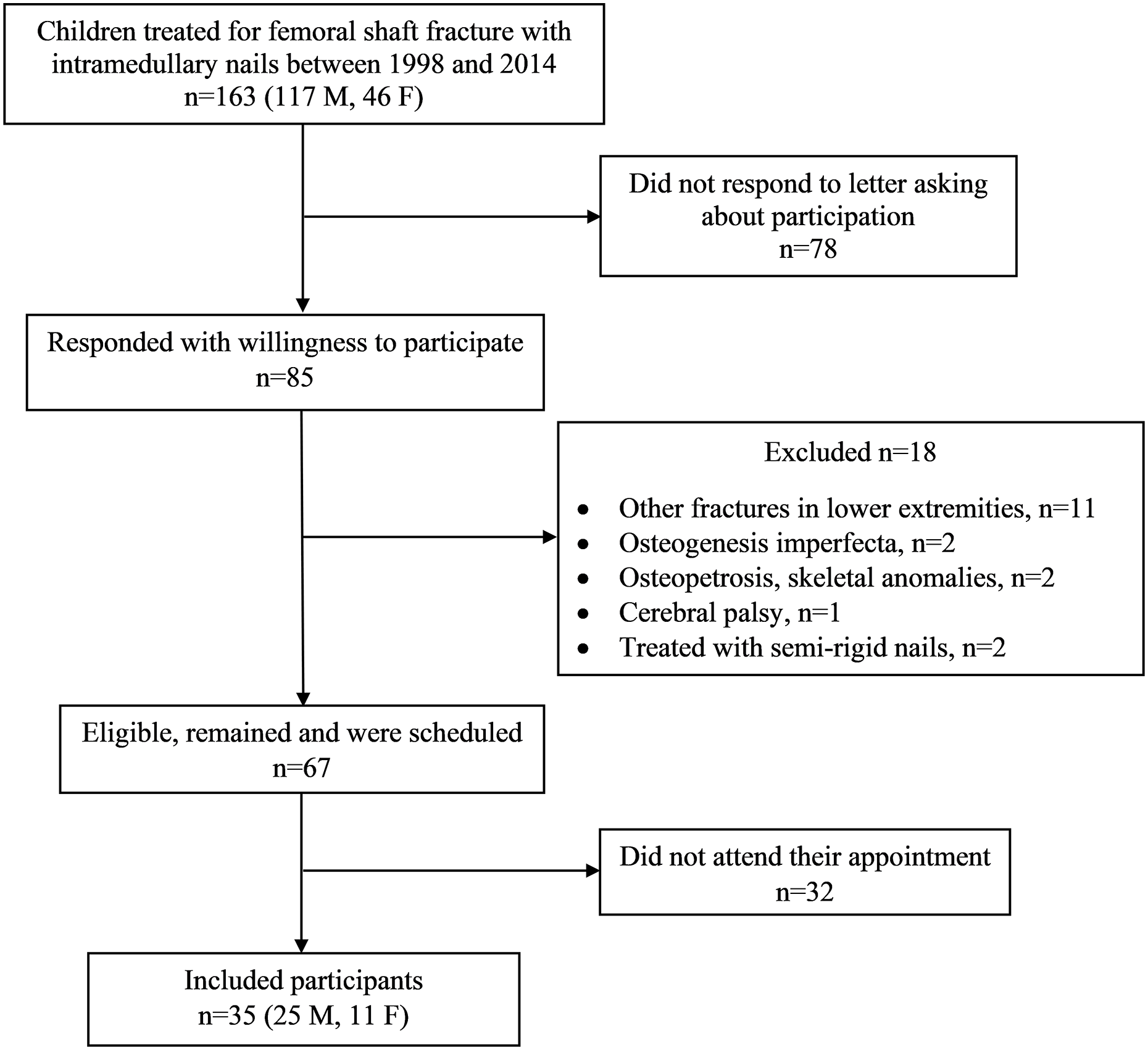
Flowchart of participant recruitment.
Demographic data
Age at time of fracture and at follow-up, sex and cause of fracture were obtained from medical records. The fractures were classified on initial radiographs, in accordance with the AO classification. 35 Fracture localization was determined as the proximal, middle, or distal third of the shaft. The number of ESINs and nail diameter were obtained from medical records and radiographs.
Assessment of radiographs at the time of fracture treatment
Femoral angulation was assessed in the frontal and the sagittal plane. Fracture stability after fixation was determined as NCD ratio, that is, the sum of the diameters of the nails divided by the diameter of the femoral canal at the narrowest site (isthmus) (Figure 2). 19 The NCD ratio at the fracture level was calculated on both the anteroposterior (AP) and the lateral view. 36 Callus formation was assessed on AP and lateral view and the callus index was calculated as the maximum width of callus formation divided by the bone width at the same level (Figure 3). 37 Fracture gap or overlap, and degree of horizontal fracture dislocation were assessed on the AP and the lateral view.
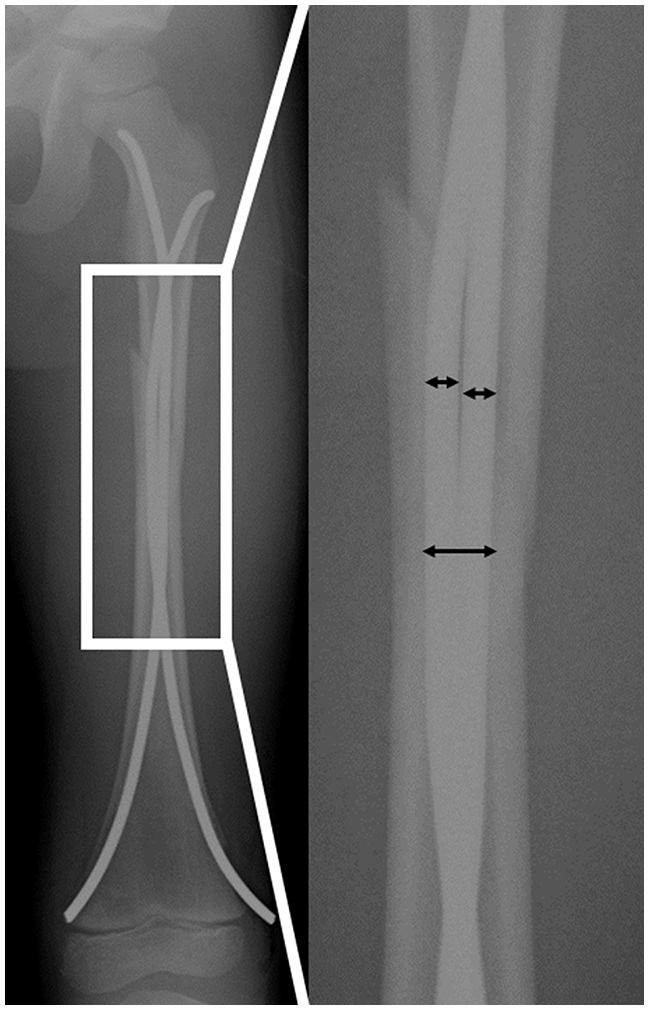
Stability assessment: nail canal diameter (NCD) ratio was calculated at isthmus on anteroposterior view.
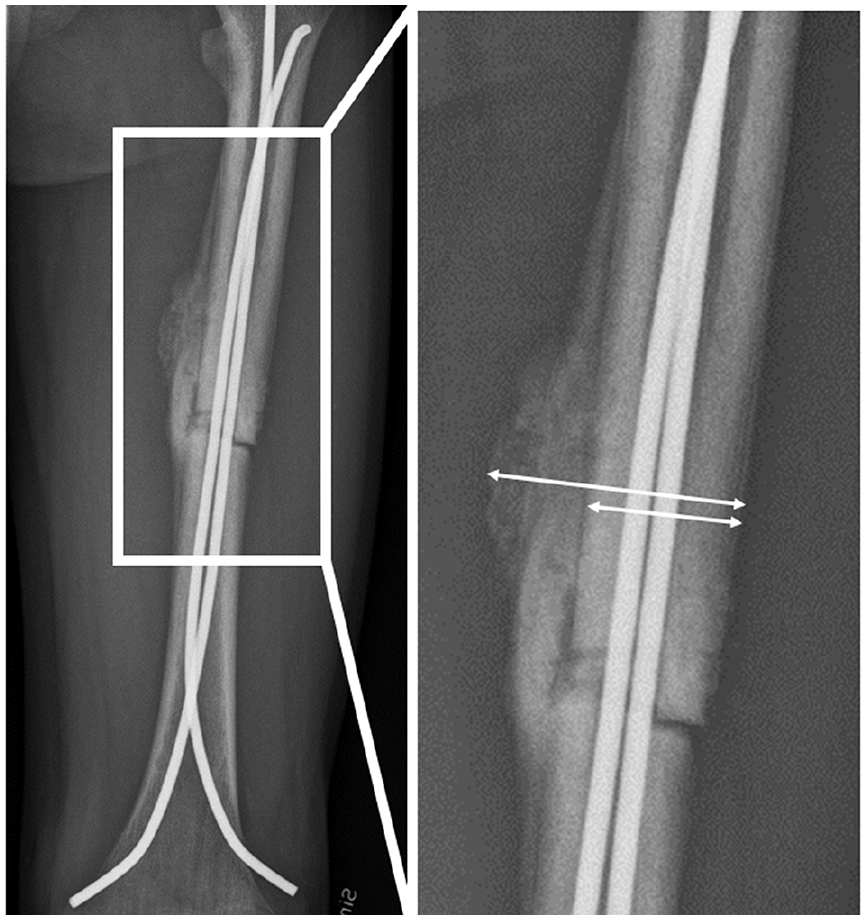
Callus formation: callus index was calculated as the maximum width of callus formation divided by the bone width at the same level.
Measurement of LLD at follow-up
Standing, full-length weight-bearing (FLWB) AP view radiographs with (GE Definium 8000, GE Healthcare, Chalfont St. Giles, UK) were performed (Figure 4). Each radiograph was composed of data from up to five exposures and was presented as a single view of the entire lower extremity with the knee fully extended. Magnification markers were placed adjacent to the lower extremity and used for calibration of the magnification factor. The leg length was defined and measured from the center of the femoral head to the distal tibia (Figure 4). The length of the femur was measured from the center of the femoral head in line with the femoral axis to a point between the periphery of each condyle. The length of the tibia was measured on the tibial axis, from a line between the tibial plateaus to the distal tibia. 38 LLD was calculated as the difference between the fractured limb and the non-fractured limb (fractured minus non-fractured). For the purpose to evaluate the individual’s perception of LLD, the difference between the longer limb and the shorter limb was used regardless of fractured or non-fractured limb. In addition, femoral angulation was assessed in the frontal plane.
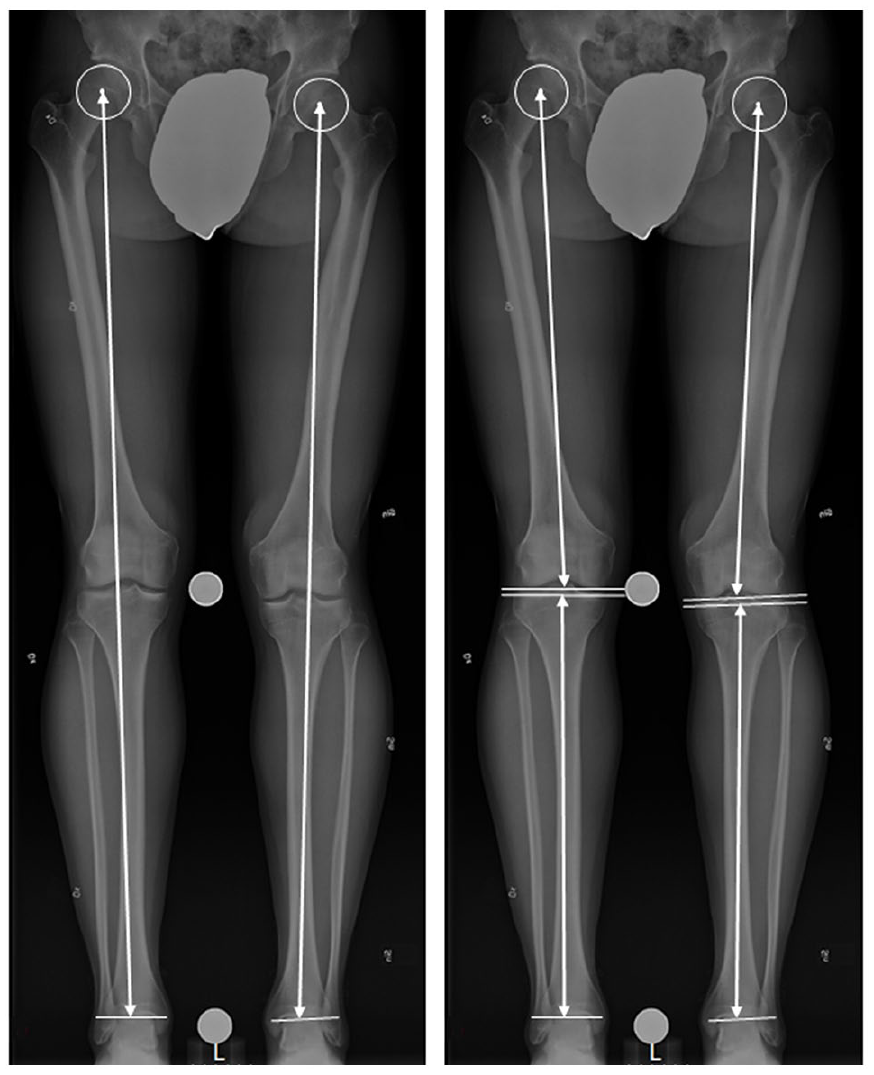
Illustration of measurement of limb length (left) and length of femur and tibia (right).
One author (M.F.) measured all radiographs. To investigate the inter- and intra-observer reliability of the measurements, two of the authors (M.F. and Y.A.) measured radiographs of 13 participants independently, twice with a 6-week interval. The inter- and intra-observer reliability for femur and tibia, and total leg length measurements were (0.936–0.964) and (0.995–1.000), respectively.
Questionnaire regarding perception of LLD and other symptoms at follow-up
Three questions were chosen to assess problems derived from LLD, and an additional question for other symptoms, to be answered in writing:
Have you noticed or experienced any LLD?
Do you experience any limping or a feeling of unevenness when walking?
Do you wear a shoe lift to compensate for LLD? How many centimeters is the shoe lift?
Do you experience any other symptoms?
If the participant answered any of the first two questions with yes, this was defined as perception of LLD.
Statistical analysis
Mean values with ranges were calculated for normally distributed continuous data, medians with interquartile ranges (IQRs) for non-normally distributed continuous data, and percentages for categorical data. The length of the longer limb compared with the shorter limb was analyzed with Wilcoxon’s signed-rank test. Spearman’s rank correlation was used to test for correlations between each of the variables (age and angulation at the time of fracture, NCD ratio, callus formation, fracture gap or overlap, and degree of horizontal fracture dislocation) and residual radiographic LLD, defined as the difference in length between the fractured and the non-fractured limb. The Mann–Whitney U test was used to analyze the differences in LLD between the groups with or without perception of LLD. The chi-square test was used to determine whether there was association between residual radiographic LLD (≥10 mm) defined as the longer limb compared with the shorter limb, and perception of LLD. The intra- and inter-observer reliability was calculated for the FLWB radiographic measurements. Statistical significance was set at p < 0.05. Statistical analysis was performed with SPSS (version 25, SPSS Inc., Chicago, IL, USA).
Results
Demographic data are presented in Table 1. Individual data demographics, number of ESINs, angulation, calculation of stability, callus formation, and length measurements are outlined in Supplemental Appendix B. In all but one participant, the ESINs had been removed at the time of follow-up.
Demographics, fracture, and treatment characteristics.
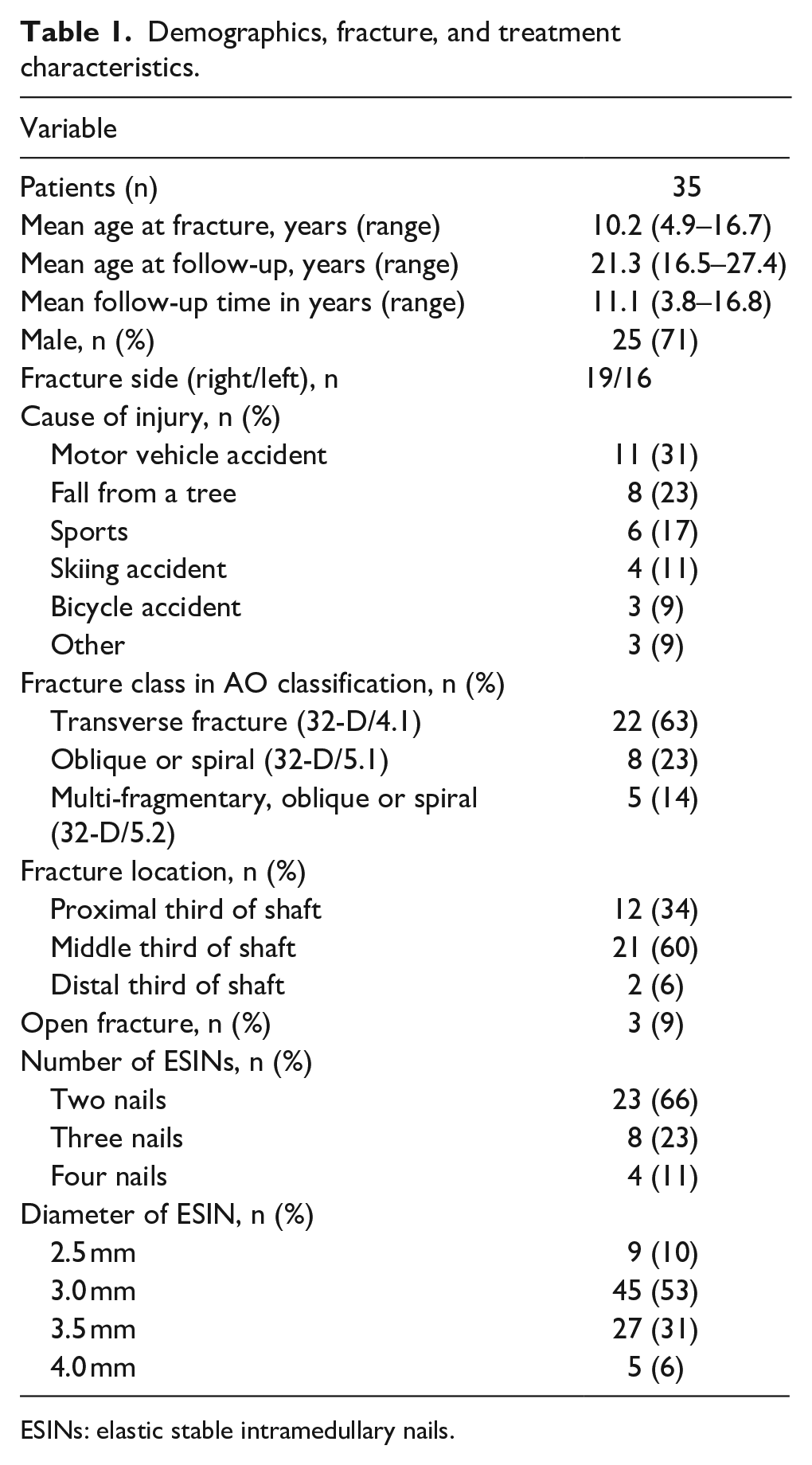
ESINs: elastic stable intramedullary nails.
Angulation, stability, and callus formation at the time of fracture treatment
The radiographic assessment for angulation, stability of fixation, and callus index was performed based on the radiographs from the first postoperative outpatient clinic follow-up after a median of 4.7 (IQR = 4.0–5.9) weeks postoperatively. Median angulation, all in varus, was 3° (IQR = 1–6). Median angulation in the sagittal plane was 4° (IQR = 1–7). The average NCD ratio was 0.9 (range = 0.6–1.5) at isthmus and 0.8 (0.4–1.4) at the fracture level on AP radiographs. In the lateral view, the average NCD ratio was 0.8 (0.5–1.3) at isthmus and 0.7 (0.4–1.1) at the fracture level. Average callus index was 1.6 (1.0–2.1) in the AP view and 1.5 (1.2–1.9) in the lateral view. Fracture gap >2 mm, in the frontal or the sagittal plane, was present in 2 of the 35 participants. None had a fracture gap >5 mm. Correspondingly, compression >2 mm was present in 7 of the 35 participants. Horizontal fracture dislocation >25% of the bone width was present in 10 of the 35 participants, none with horizontal fracture dislocation >50%.
Radiographic LLD and femoral angulation at follow-up
The fractured limb was median 7 mm (IQR = 5–11, range = 1–15) longer in 24 of the participants. In the remaining 11 participants, the fractured limb was median 9 mm (IQR = 5–11, range = 1–23) shorter. When comparing the longer limb with the shorter limb regardless of the fractured or the non-fractured, the longer limb was median 7 mm (IQR = 5–11, range = 1–23) longer, p < 0.001. The differences depended on a difference in femur length, median 7 mm (IQR = 4–12, range = 2–16), p < 0.001, and not at the tibial level, median 0 mm (IQR = −3 to 3, range = −5 to 8), p = 0.939. Lengthening of the fractured limb of ≥10 mm was seen in 11 (31%) participants, who were 4.9–11.9 years of age at time of fracture. Shortening of the fractured limb of ≥10 mm was seen in 5 (14%) participants, who were 9.6–16.7 years of age at time of fracture. Children with a fracture before age 9 years (n = 11) had a longer limb on the fractured side, while both shortening and lengthening were seen among older children and adolescents.
The median angulation, all in varus, was 3° (IQR = 2–4). Two participants had more than 10° of angulation, 14° and 16°, respectively.
Correlations
There was a negative correlation between radiographic LLD at follow-up, and age at time of fracture (Rs = −0.49, p = 0.003; Figure 5). There was a positive correlation between femoral angulation approximately 1 month postoperatively and residual radiographic LLD (Rs = 0.42, p = 0.013). No significant correlations were found between residual radiographic LLD and NCD ratio at isthmus or at fracture level in the AP or lateral view. Nor were there any significant correlations between radiographic LLD and callus index, fracture gap, or overlap or horizontal fracture dislocation in either view.
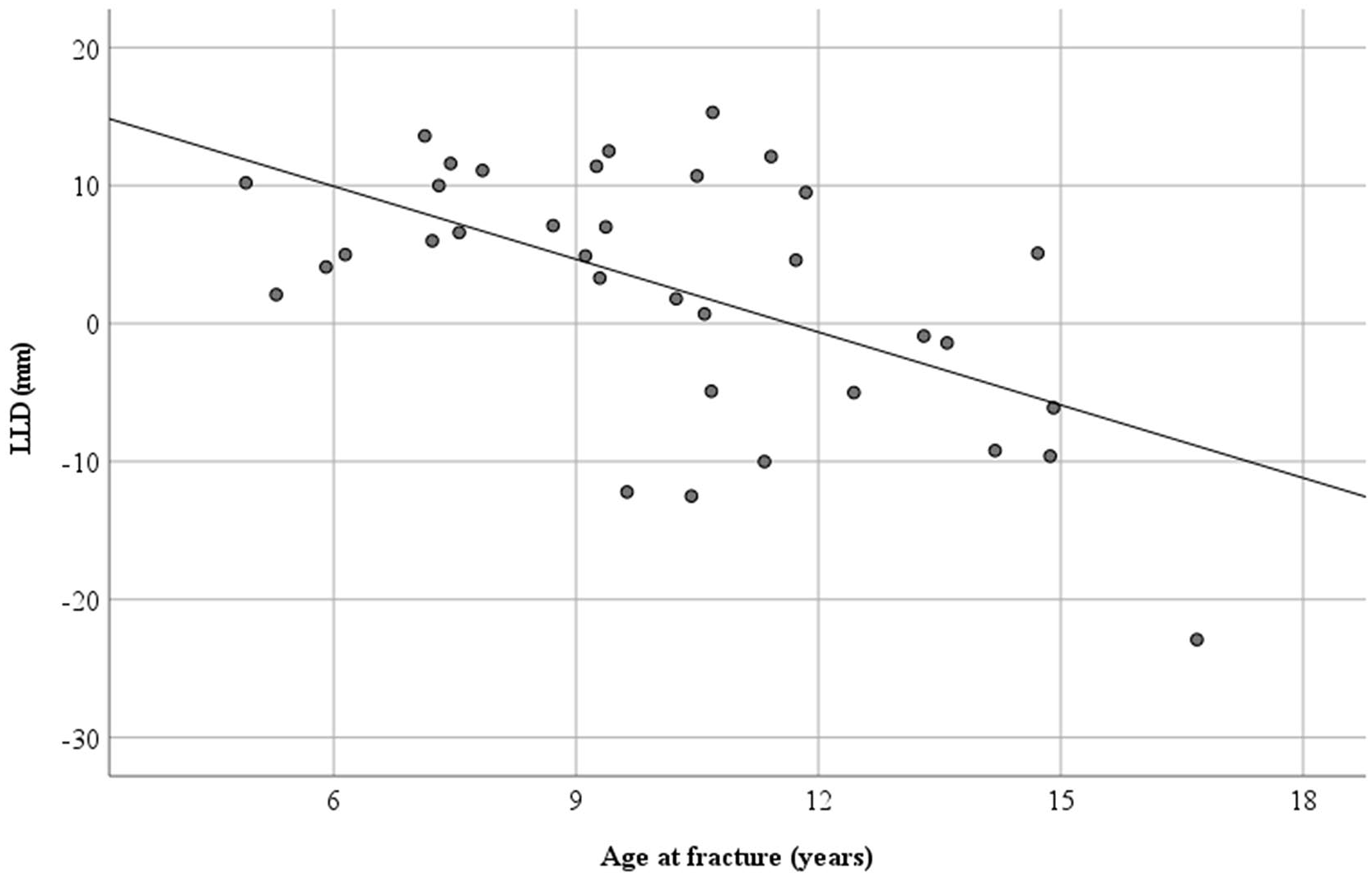
Residual radiographic leg length discrepancy (LLD), defined as the difference between the fractured and the non-fractured limb, in relation to age at time of fracture (n = 35). A positive LLD value means lengthening, and a negative value means shortening.
Questionnaire regarding perception of LLD and other symptoms at follow-up
Fourteen participants (40%) reported perceived LLD, by answering yes to the first two questions, with other words reported they noticed or experienced LLD, as well as limping or a feeling of unevenness when walking. There was neither a statistical difference in radiological LLD between the participants reporting perceived LLD and the 21 who did not (median = 10 mm IQR = 5–12 vs 7 mm IQR = 5–11, p = 0.377), nor a significant difference in the proportion of individuals with perceived LLD among individuals with radiographic LLD ≥10 mm (n = 8 out of 14) compared with individuals with radiographic LLD <10 mm (n = 6 out of 14), p = 0.268. There was no statistical difference in perception of LLD regardless of if the fractured limb was shorter or longer at follow-up, p = 0.673. Of those with lengthening of ≥10 mm, five participants (45%) experienced perception of LLD, as did three (60%) of those with shortening ≥10 mm. Of those with an LLD <10 mm, six (32%) reported perceived LLD.
Of the fourteen participants who perceived LLD, four reported a feeling of unevenness when walking, of whom one reported use of a shoe lift of approximately 2 cm (radiographic LLD was 10 mm, and femoral angulation was 14°). Ten participants reported musculoskeletal pain; eight (80%) of these ten reported perception of LLD (Table 2). None of the participants had been treated surgically for LLD.
Number of participants with radiographic leg length discrepancy a (LLD), perception of LLD, and other symptoms, at follow-up in adults with femoral shaft fracture in childhood (n = 35).
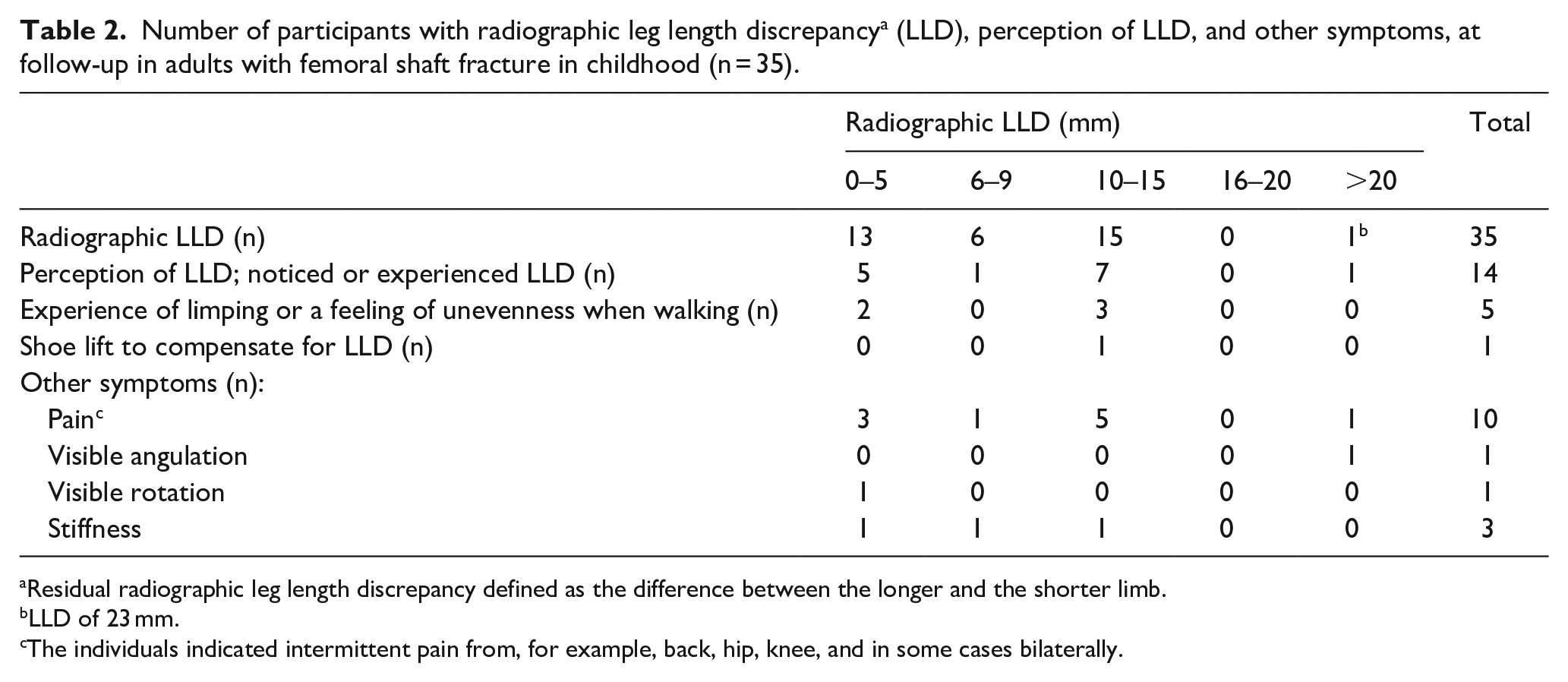
Residual radiographic leg length discrepancy defined as the difference between the longer and the shorter limb.
LLD of 23 mm.
The individuals indicated intermittent pain from, for example, back, hip, knee, and in some cases bilaterally.
Discussion
This study identified 16 of 35 (46%) individuals with residual LLD ≥10 mm. Children under 9 years of age at the time of fracture seemed to be more prone to lengthening, while both shortening and lengthening were seen in older children. Perception of LLD was reported in 14 (40%) of 35 participants.
Our results on LLD after skeletal maturity are in line with two previous studies evaluating LLD after femoral shaft fractures treated with ESIN, although their follow-up time was short and did not reach to after skeletal maturity.7,17 In a 3-year follow-up of 29 patients, Gogi et al. 17 reported that nine children had an average lengthening of 2.7 mm, and three had an average shortening of 11.7 mm. Residual varus angulation was median 3° in this study, which is similar to the results of Lohiya et al. 18 In this study, the residual LLD and angulation indicated mostly excellent or satisfactory results according to Flynn’s scoring criteria. 13
Hresko and Kasser reported injury to the femoral physis in association with non-physeal fractures in the lower extremity, and recommended adolescents who have femoral fractures to be evaluated and followed for possible physeal injury. 39 Two participants had more than 10° of angulation, 14° and 16°, respectively, at level of the fracture. None of the participants in this study had any signs of physeal injury.
Three participants had a shortening more than 10 mm (12, 13, and 23 mm, respectively). The individual with a shortening of 23 mm, clearly not a satisfactory result, had an angulation of 16°. He was 16.7 years at the time of fracture and follow-up time was 3.8 years. A solid intramedullary nail rather than ESIN would have provided more appropriate fixation.
In the older age group and in heavier children, there has been a major shift since the time period the participants of this study were treated, with the development of physeal sparing interlocking nails, toward intramedullary nails. At the same time, there has been a trend toward ESIN even in younger children before school-age. Hence, traction and cast treatment where an overlap of 1–2 cm depending on age is considered appropriate to prevent LLD caused by overgrowth. 32 This treatment is well known, reliable, and has low morbidity, and is furthermore, convenient in developing countries.
Regarding the influence of stability of fixation on LLD, Park et al. 19 reported, in a 41-month follow-up, lengthening of the fractured femur by mean 14.1 mm in relatively unstable fracture fixation, NCD ratio of mean 0.8 (range = 0.6–0.9), as opposed to mean 3.8 mm in relatively stable fracture fixation, NCD ratio of mean 0.9 (0.7–1.0). In our slightly older cohort, the average NCD ratio was 0.9 (0.6–1.5), indicating a relatively stable construct, and we found no significant correlation between NCD ratio and radiographic LLD in skeletal maturity.
Even though the principle of ESIN is a three-point support for two nails, it might be useful in length-unstable fractures to fill the canal with several nails to increase stability and prevent shortening.40,41 Kaiser et al. 42 describe the use of a third nail to increase stability, but emphasize that the correct technique should be used for the first two nails. Our cohort was too small for specifically analyzing those with three or four nails.
Excessive callus formation as a sign of indirect fracture healing and the remodeling process that follows may result in overgrowth. 28 In this study, callus index did not correlate with residual LLD in skeletal maturity. Residual LLD could be secondary to the surgical treatment. When assessing the fracture gap and overlap as well as the degree of horizontal fracture dislocation postoperatively, we found no significant correlation between these variables and radiographic LLD in skeletal maturity.
The literature on the perception of LLD is scarce, and the aim of the questionnaire was to provide an insight on long-term perceived LLD and other symptoms. Unexpectedly, out of 14 participants with perception of LLD, six had a radiographic LLD <10 mm. We can only speculate as to why these six participants experienced a difference in leg length. It might be related to biomechanical changes of the lower extremity or hip. In general, a shorter or a longer limb did not affect the perception of LLD among the participants. It was beyond the scope of this study to evaluate residual pain, but a surprisingly large proportion (29%) reported musculoskeletal symptoms, including pain, at follow-up. In the future, follow-up studies including validated patient-reported outcome measures (PROMs) could increase knowledge of the long-term results, including pain, after femoral shaft fractures in childhood.
Limitations
One of the limitations in this study was the few participants and the high number lost to follow-up, which may increase the risk of selection bias; individuals with persistent symptoms may have a greater willingness to participate. The relatively small study group made it problematical to stratify by age, fracture type, localization, and the number of nails. Another potential limitation is the lack of a control group regarding radiological and perceived LLD. We used a non-validated questionnaire since we did not find any PROMs addressing perception of LLD. Patients’ weight and information regarding postoperative weight-bearing regimen could rarely be identified in the medical charts. The standing radiographs were performed at two hospitals, but with the same technique and type of equipment. The standing radiographs did not include sagittal angulation. Clinical examination could have added information on LLD, range of motion, malrotation, and objective as well as subjective symptoms. One limitation including children with different ages as in our cohort is the difference in healing and remodeling potential, that most likely influence the development of LLD.
Conclusion
Treatment of femoral shaft fractures with ESIN in childhood may result in residual radiographic LLD (≥10 mm) after skeletal maturity. Children under the age of 9 years at the time of fracture seemed to be more prone to lengthening, while both shortening and lengthening was noted in older children. There was no indication that fracture stability or callus formation influenced residual radiographic LLD. Perception of LLD in skeletal maturity is not necessarily associated with a radiographic LLD (≥10 mm). Our results may be useful from a clinical perspective and underline the importance of follow-up to identify those with LLD that might require treatment before skeletal maturity.
Footnotes
Acknowledgements
The authors thank Associate Professor Aina Danielsson (A.D.), MD, PhD, senior pediatric orthopedic surgeon, Department of Orthopaedics, Sahlgrenska University Hospital, Gothenburg, Sweden, for developing the questionnaire, and Salmir Nasic, FoU Skaraborg Hospital, Skövde, Sweden, for statistical advice.
Author contributions
M.F. (MD) contributed to the study design, data acquisition, analysis and interpretation of data, and manuscript preparation. J.v.H. (MD, PhD) contributed to the study design, analysis and interpretation of data, and manuscript preparation. Y.A. (MD, PhD) contributed to the study design, performed measurements, and manuscript preparation. J.R. (Associate Professor, MD, PhD) contributed to the study design, analysis and interpretation of data, and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by regional research grants from Västra Götalandsregionen, and from Göteborgs Läkaresällskap. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Informed consent
The study was approved by the Regional Ethical Review Board of Gothenburg (Dnr 495-12), and written informed consent was obtained from all individual participants, or their guardians if they were aged <18 years, included in the study.
Research involving human participants
The STROBE guidelines were followed in the development and reporting of this study. 43 All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Supplemental material
Supplemental material for this article is available online.