
Abstract
Purpose
Fractures of the lateral condyle of the humerus in children are a common injury. If displaced or unstable they may require surgical reduction and fixation with Kirschner wires (K-wires). K-wires are placed using either an open or closed technique. The decision to bury or leave the ends extending through the skin is surgeon-dependent and based on factors including post-operative infection risk, bony union and ease of wire removal.
Methods
We performed a systematic review and meta-analysis of non-buried versus buried K-wires for lateral condyle elbow fractures in children in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses methodology. A comprehensive search strategy included Medline, Embase and CINAHL via NICE Evidence from database inception to June 2017. Two authors independently reviewed, included or excluded articles, extracted data and assessed for quality with the ROBINS-I tool. We performed direct comparison meta-analysis for all adverse events, post-operative infection and failure of bony union.
Results
Three studies were analysed comprising of 434 participants. There was a significantly reduced relative risk of adverse events in the non-buried group, equating to approximately 45% reduced risk (RR 0.55, 95% confidence interval 0.34 to 0.88). There were no significant differences in risk of post-operative infection or failure of bony union. All three cost-analyses in the included studies observed savings with non-buried K-wires.
Conclusion
Non-buried K-wires for lateral condyle elbow fractures convey a lower risk of adverse events and may be more cost-effective compared with buried K-wires. Non-buried K-wires do not appear to increase the risk of infection or failure of bony union. These findings are limited by a high risk of bias due to inherent methodological flaws in the design of included studies.
Introduction
Fractures of the lateral condyle of the humerus in children are a common injury, accounting for 12% to 20% of all elbow fractures, which in turn are the second most common fracture in children, usually occurring between the ages of five and ten.1–3 If non-displaced, they can be managed non-operatively with immobilisation and monitoring for nonunion. 4 If they are displaced or unstable, then these fractures require operative management with open, or limited open reduction and internal fixation with Kirschner wire (K-wire) or screw fixation. 5 K-wires are placed using either an open or closed technique and the ends of the wire are then either buried or left non-buried, extending through the skin. This decision is generally based on surgeon preference.
Buried wires may improve patient comfort and theoretically may reduce infection rate and improve bony union. Non-buried wires are easily removed in the outpatient setting and avoid the need for a second general anaesthetic, operating time and additional cost associated with removing buried K-wires. This is inconvenient for the parents of the patients and has financial implications for both them and the health service. There is clinical equipoise in terms of whether the wire is buried or not and this is a theme that is seen in other areas of upper limb trauma. 6 For lateral condyle elbow fractures, the risk of erosion of the buried wire through the skin has emerged as an important adverse event and may necessitate an early return to theatre for wire removal.7–9
Therefore, the main concerns that appear to determine whether wires are buried or not in the paediatric elbow are the difference in adverse outcomes between the two techniques, specifically risk of infection and risk of erosion. The aim of this systematic review and meta-analysis is to provide an overview of the current evidence for non-buried versus buried K-wires in paediatric lateral condyle elbow fractures and quantify the risk of key adverse outcomes, between the two techniques, to enable evidence-based decision-making for surgeons and patients.
Materials and methods
Search strategy
We performed an exhaustive search of the Medline, Embase and CINAHL via National Institute for Health and Care Excellence Evidence Search (searched 19 June 2017). The search strategy in Figure 1 was used to identify all studies and reviews relating to management of K-wires in paediatric lateral condyle elbow fractures. Searches were not limited by date, language or publication status. The search results were independently screened for relevance by two authors (JCW and CYP). Full-text articles were retrieved via NHS OpenAthens and the Royal College of Surgeons Library. Only studies directly comparing non-buried or buried K-wires in the context of paediatric lateral condyle elbow fractures were included. Each included study was assessed for methodological rigor using the Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) tool. 10 No indirect comparison meta-analysis was performed due to the quality of the original data and the high risk of bias, inherent in case series. 11 As post-operative infection and skin erosion is the key determinant of technique, these were considered to be our co-primary outcomes. The unit of analysis was taken to be the patient rather than the elbow. 12 Existing reviews were screened to ensure all relevant primary studies had been identified. Disagreements on study eligibility were resolved by consensus, with reference to the senior author (DME). The process of inclusion and exclusion of studies according to these criteria is displayed in a study attrition chart in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Fig. 1). The study protocol was prospectively registered with the PROSPERO database (http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42017071113).
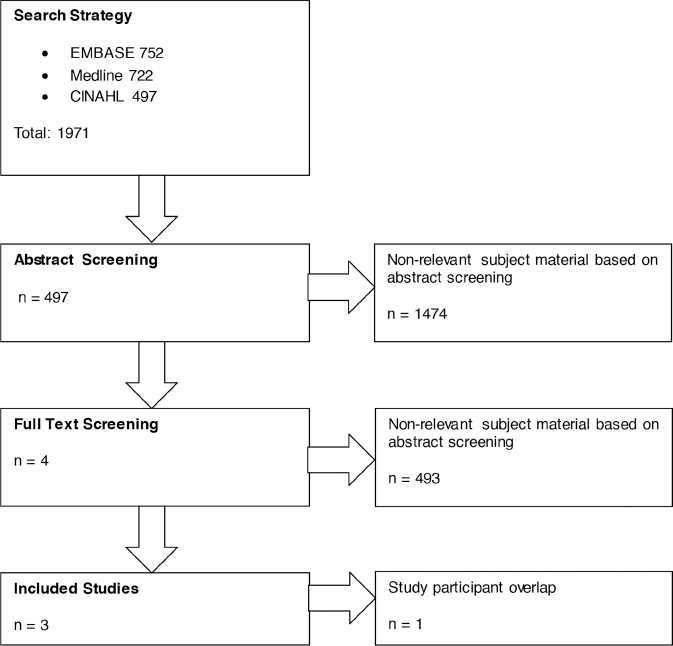
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
Data collection and analysis
Data was extracted onto a pre-defined electronic data extraction form by one author (JCW), which was independently checked by another author (CYP). All authors of the included studies were contacted by the senior author (DME) for further information about antibiotic protocols and specific technique.
Statistical analysis
We performed simple descriptive statistics for patient demographics. The rate of post-operative infection and wire erosion were calculated for each group (non-buried versus buried) so that results could be compared across included studies. The primary outcomes, post-operative infection and wire erosion were calculated and displayed as a rate (%). If three studies reported the same outcome, then the data from the single studies were pooled for comparative analysis. We performed direct comparison meta-analysis with RevMan5 (Review Manager (RevMan) Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) to calculate relative risk ratios with 95% confidence intervals (CI) using the Cochran-Mantel-Haenszel test. We used a fixed-effects model due to relative study homogeneity. No subgroup analysis was planned or undertaken. Statistical heterogeneity was quantified for all direct comparisons using the I2 statistic. 13 Significance was set at the 5% level. Meta-analysis results are displayed in a forest plot and a funnel plot was produced to assess publication bias in our primary outcome. 14
Results
Our search strategy yielded a total of 1971 research articles; of which four were primary clinical studies directly comparing non-buried versus buried K-wires in lateral condyle humeral fractures in children (Table 1).7–9,15 The studies were carried out between 2011 to 2016 and included a total of 501 patients, of which 351 underwent K-wire fixation of lateral condylar fractures with non-buried wires and 150 had the same procedure but with buried wires. Two studies were from the United Kingdom, one from the United States and one from Singapore. The two from the United Kingdom were reports from the same institution and so this group was contacted to assess the independence of the study populations.7,8 Both studies contained cross-over of study participants and so only the latest paper was included. 8 This resulted in a pooled population of 296 patients with non-buried wires and 138 with buried wires. All three of the included studies were retrospective case series. Sample sizes ranged from 75 to 234 with the study periods ranging from four to ten years. The follow-up periods ranged from 1.5 months to eight months. According to the ROBINS-I tool, all of the included studies were at high risk of bias due to their retrospective, non-randomised design and lack of outcome assessor blinding. 10
Characteristics of included studies
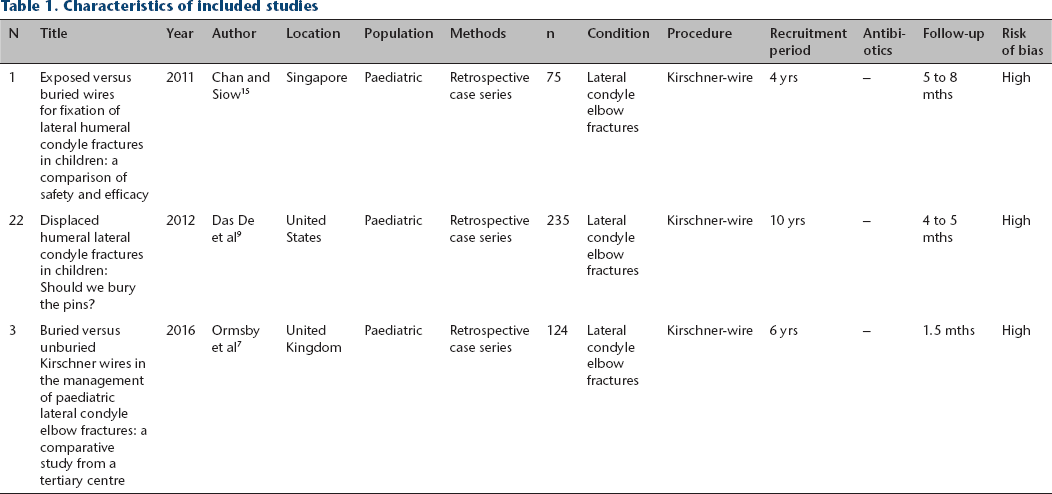
In two of the included studies9,15 all of the patients received open reduction of the lateral condylar fracture and K-wire fixation. In Ormsby et al, 7 122 of the 124 patients underwent open reduction and K-wire fixation, while two patients underwent closed reduction, arthrogram and percutaneous K-wire fixation. All 60 patients managed with buried K-wires underwent an open reduction. The buried K-wires were subsequently removed under general anaesthetic at either six weeks for two studies7,9 or at 11 weeks. 15 In one study 9 the buried wire was removed in clinic with the patient awake only if it had eroded through the skin. In all studies, patients were immobilised in an above elbow plaster backslab. All non-buried wires were removed in clinic at four weeks without general anaesthetic.7,9,14
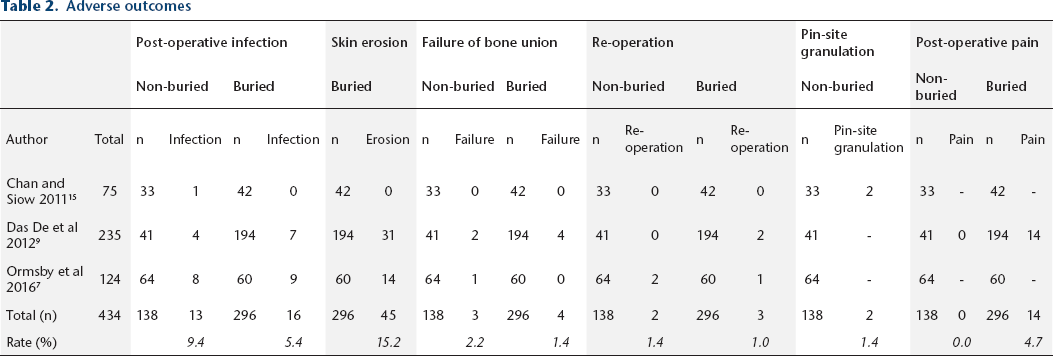
Outcome reporting was consistent across all studies for post-operative infection, skin erosion for buried wires, non- or malunion and need for re-operation (Table 2). Across all studies, there were a total of 18 adverse events in the non-buried group (13%) compared with 68 adverse events in the buried group (23%). These included post-operative infection, skin erosion, non- or malunion and need for re-operation (not including planned removal of buried wires). On direct comparison meta-analysis, there was a significantly reduced relative risk of adverse events in the non-buried group, equating to approximately 45% reduced risk (RR 0.55, 95% CI 0.34 to 0.88, Fig. 2). There was minor heterogeneity for our primary outcome (I2 = 9%) and a funnel plot indicated no publication bias.
Adverse outcomes

Forest plot showing adverse events (K-wire, Kirschner wire; M-H, Cochran-Mantel-Haenszel; CI, confidence interval; df, degrees of freedom).
In the majority of cases, the diagnosis of post-operative infection was made clinically, although one study also used adjunctive microbiological evidence. 8 Infection was described as either superficial or deep. In all, 10% (n = 3) of all infections across the three studies were described as deep, with two deep infections occurring in patients with buried K-wires and one occurring in a patient with a non-buried K-wire. The rate of post-operative infection was calculated for each study and ranged from 0.02% in the study by Chan and Siow 15 as the lowest rate across both groups to 15% in the study by Ormsby et al 7 – both in the buried K-wire group. The range of infection rates in the non-buried group was 3% to 12.5%. On direct comparison meta-analysis, there was no significant difference between the rate of post-operative infection between the two groups (RR 1.32, 95% CI 0.68-2.56, Fig. 3).

Forest plot showing post-operative infection (K-wire, Kirschner wire; M-H, Cochran-Mantel-Haenszel; CI, confidence interval; df, degrees of freedom).
All the included studies reported erosion of the wire through the skin in patients with buried K-wires. These rates were substantially higher than post-operative infection, apart from in one paper where no erosions occurred. 15 The range of skin erosion rates in the three papers where this adverse event was reported was 0% to 23%, with a pooled rate of 15%. This outcome is only applicable to buried K-wires as non-buried wires are not by definition beneath the skin. Skin erosion is a major contributor to the rate of adverse events in the buried group (Fig. 2).
Failure of bony union occurred rarely across the included studies. In the non-buried groups there were three cases across the 138 patients (2.2%), and in the buried group there were four cases out of the 296 patients (1.4%). There was no significant difference in risk of failure of bony union on meta-analysis (Fig. 4). The need for unplanned re-operation was also rare with two patients in the non-buried group (1.4%) returning to theatre and three patients in the buried group (1.0%). Two patients with non-buried wires required re-operation due to infection. Two patients in the buried cohort required re-operation for internal pin migration and one required re-fixation due to malunion. Again, this was not statistically significant between the two groups (Fig. 5). The length of time the K-wires remained in situ was reported all three studies. Non-buried wires were generally removed at four weeks in all three studies. For buried wires, two studies 7,9 removed wires at six weeks while the third study removed wires after 11 weeks 15 . Interestingly, the length of time that K-wires were left buried did not appear to influence complication rate, as Chan and Siow 15 reported no incidence of erosion or infection despite keeping pins in situ for a substantially longer duration. There is insufficient data to comment on this definitively. Only one study 9 reported post-operative pain, which was higher in the buried group (non-buried = 0.0%, buried = 7.0%) but this did not appear to be measured on a validated pain scale. Chan and Siow 15 reported two cases of non-buried pin site over granulation that responded to silver dressings and did not require further intervention.

Forest plot showing failure of bony union (K-wire, Kirschner wire; M-H, Cochran-Mantel-Haenszel; CI, confidence interval; df, degrees of freedom).

Forest plot showing re-operation (K-wire, Kirschner wire; M-H, Cochran-Mantel-Haenszel; CI, confidence interval; df, degrees of freedom).
Discussion
This systematic review and meta-analysis of non-buried versus buried K-wires for lateral condyle fractures provides a summary of the evidence that informs this technical decision and sheds new light on the potential sequelae. The importance of this clinical question is apparent from the number of studies that have attempted to challenge equipoise on this decision. The key driving factors in deciding to bury or not bury K-wires in these common paediatric fractures are broadly related to surgical and economic considerations.
The primary outcome of the included studies was post-operative infection. The risk of infection in non-buried wires is thought to be higher due to the concept of bacteria tracking from the outside environment, along the pin and into the bone. This is a concern that is shared in all upper limb fracture surgery. Interestingly, a recent review by the primary author indicated that on descriptive analysis the risk of infection in non-buried wires appeared to be restricted to hand fractures. 6
Similarly, the actual incidence of osteomyelitis across eight studies of non-buried versus buried K-wires in upper limb fracture was very low (0.2%). 6 Routine antibiotic usage was inconsistent in the reports of the included studies. Following request, the authors of each included study provided additional information on antibiotic protocol. The study population of Chan and Siow 15 routinely received three peri-operative doses of intravenous antibiotic, whilst the study populations in Das De et al 9 and Ormsby et al 7 received a single peri-operative dose of intravenous antibiotic. Our meta-analysis found no significant difference in post-operative infection between non-buried and buried K-wires for lateral condyle fractures, which should help to direct clinicians to other outcomes of interest and economic considerations. Indeed, the in-depth cost analysis by Das De et al 9 indicates that even when infection is included in analysis, the cost of buried K-wires outweighs that of non-buried K-wires.
Erosion of the wire through the skin for buried K-wires was the most common complication across both techniques. The erosion of the wire through the skin is of particular concern as a basis for burying the wire is the presumption of reduced infection rates with no exposed metalwork. 7 The erosion of the skin would negate any such presumed benefit. This complication was seen in two out of three of the included studies and was the major contributor to the statistically significant increased risk of adverse events in buried K-wires (Fig. 2.) The senior author (DME) and authors of the included studies believe that wire erosion occurs due to a combination of surgical factors, including the ends of the wires not being bent sufficiently, inadequate wound protection with padding and prolonged time to removal of wires. In this population, it is unlikely that patient factors, such as co-morbidity, would have a significant effect on the overall incidence of erosion. Both Das De et al 9 and Ormsby et al 7 theorise that the oedema associated with lateral condyle fractures leads to increased soft-tissue tension, potentially accounting for the higher rates of wire erosion in buried wires. Das De et al 9 further attributed the increased level of pain reported in their study to soft-tissue tension.
Rates of non- and malunion were low across all studies and there was no significant difference on meta-analysis. Anecdotally, there is a perceived benefit in a stronger fixation and lower risk of failure of bony union in buried K-wires which forms part of the rationale for this technique. This was not borne out by any of the individual studies, nor was it seen on pooled analysis (Fig. 4). Therefore, along with post-operative infection, our results indicate that failure of bony union is not a strong rationale for opting to bury K-wires in lateral condyle elbow fractures.
All three of the included studies provided cost-effectiveness analyses. Chan and Siow 15 described a saving of $800 to $1000 per patient for patients with non-buried compared with buried wires. Das De et al 9 performed an in-depth decision-based, cost-effectiveness analysis, which concluded that despite an estimated cost of treating deep infections ranging from $3710 to $32 130, and taking into account their estimated rate of infection in non-buried wires at 7%, leaving the K-wires non-buried was the most cost-effective technique, equalling a saving of $3442 per patient compared with buried K-wires. Most recently, Ormsby et al 7 performed a United Kingdom-based cost-effectiveness analysis based on local NHS tariffs of theatre time and ward costs, estimating that a ‘per patient’ saving of £1400 could be made by not burying K-wires.
This systematic review was limited by the quality of the included studies. According to the ROBINS-I Tool, all of the included studies had a high risk of bias, predominantly due to pre-intervention selection bias; inherent in their study design. 10 This limits the reliability of the observations we have made in our meta-analysis. The sample sizes are small and may be under-powered to determine differences in outcomes, although this will have been mitigated to some extent by pooled analysis. However, outcome reporting was generally consistent and appropriate to the research question.
This systematic review and meta-analysis provides an overview of the evidence for non-buried versus buried K-wires for paediatric lateral condyle elbow fractures. Despite limitations in the design of the included studies, our meta-analysis suggests a nearly two-fold increased risk of adverse events when the wires are buried beneath the skin compared with when they are left non-buried. There was no difference in rates of post-operative infection or failure of bony union between the two techniques and non-buried K-wires confer substantially less cost to the health system.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.