
Abstract
Purpose
The aim of this retrospective study is to report the rate of displacement of Jakob Type 1 lateral condyle fractures that were initially treated in a cast.
Methods
We performed a retrospective review of all patients that were treated for a non-displaced (Jakob Type 1 < 2 mm) lateral condyle fracture of the humerus at our institution between 2002 and 2015.
Results
A total of 59 patients were initially treated with casting. Five fractures displaced and were converted to a closed pinning treatment plan with a conversion rate of 8.5%. There was a mean of 13.2 days (4 to 21) between treatment by initial casting and closed pinning.
Conclusion
This study demonstrates an 8.5% displacement and conversion rate from cast treatment to closed pinning for initially non-displaced Jakob Type 1 lateral condyle fractures of the humerus. The internal oblique radiograph is most accurate to determine displacement. We recommend obtaining an internal oblique view at initial evaluation and at follow-up in the cast for lateral condyle fractures. To minimize movement at the fracture site, we recommend treating Jakob Type 1 lateral condyle fractures with a long arm cast with the elbow at 90° and the forearm in the supine position with a sling-loop design.
Level of Evidence
IV – retrospective therapeutic study
Introduction
Lateral condyle fractures of the humerus are the second most common operative elbow injury for children following supracondylar fractures.1,2 Lateral condyle fractures of the humerus most commonly occur in paediatric patients around six years old. 3 There are two classification systems that exist to categorize lateral condyle fractures: the Milch Classification and the Jakob Classification.4,5 Milch Type 1 fractures travel medially into the capitellar-trochlear groove and Milch Type 2 fractures travel medially through the trochlea.3,5,6 The Milch Classification system is often used clinically but this classification system does not accurately indicate treatment. The Jakob Classification provides clinically useful information and treatment guidance. There are three types of lateral condyle fractures according to the Jakob Classification. Type 1 is a non-displaced fracture <2 mm. Type 2 is a minimally displaced fracture >2 mm with an intact cartilaginous hinge. Type 3 fractures are displaced and the capitellum is rotated from the joint 7 (Fig. 1). Jakob et al 4 observed in a cadaver model that non-displaced fractures demonstrated an intact cartilaginous hinge that anchored the lateral condyle fracture to the humerus. They proposed that a fracture becomes unstable once this cartilaginous hinge is disrupted. Weiss et al 8 further characterized the Jakob Classification as a predictive tool for complications by incorporating arthrogram findings. 8 Weiss demonstrated that fractures displaced > 4 mm always had a displaced articular hinge.
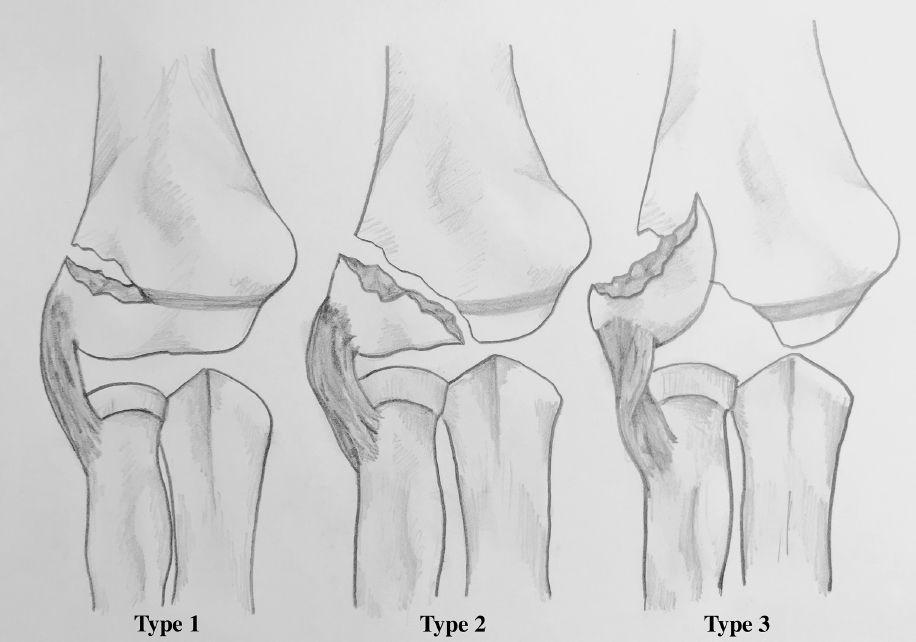
Type 1, 2 and 3 lateral condyle fractures according to the Jakob Classification (illustration drawn by Z. A. Winthrop).
Non-displaced fractures are commonly treated by cast immobilization and displaced fractures are treated with pinning or open reduction and internal fixation. 9 In the current study, we are focusing on non-displaced (< 2 mm) lateral condyle fractures treated with cast immobilization. The specific aim of this retrospective case series is to report the rate of treatment conversion from casting to pinning and the outcomes in a group of paediatric patients that initially underwent non-surgical management of non-displaced lateral condyle fractures of the humerus.
Materials and methods
This study was approved by the College of Medicine Institutional Review Board. We performed a retrospective review of all paediatric patients that were treated for a lateral condyle fracture of the humerus at our institution between 2002 and 2015. Records for patients that were treated for a non-displaced (Jakob Type 1: < 2 mm) lateral condyle fracture of the humerus were collected. Paediatric patients that were 14 years old and younger at time of injury or diagnosis were included. Patients that underwent initial surgical management were excluded. Patients with incomplete follow-up were excluded. Patient demographic information, cast duration and complications of treatment were recorded for each case. All radiographic images were obtained with standard elbow protocol by our Radiology Department. Displacement was measured in mm on digital images.
Results
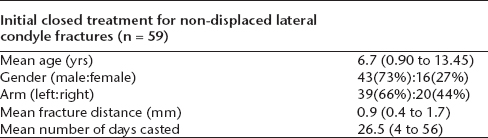
A total of 150 paediatric patients were treated for a lateral condyle fracture during the retrospective study period. There were 43 boys (73%) and 16 girls (27%) included in this study. In all, 39 patients (66%) fractured their left arm and 20 patients (44%) fractured their right arm. The mean age was 6.7 years (0.90 to 13.45) (Table 1).
Non-displaced lateral condyle fracture patient demographics
A total of 84 Jakob Type 2 and Jakob Type 3 patients were treated surgically and therefore all Jakob Type 2 and 3 cases were excluded from the study. Seven patient records were lost to follow-up. In all, 59 Jakob Type 1 patients were initially treated non-operatively. A total of 54 Jakob Type 1 patients healed uneventfully with casting. Five Jakob Type 1 patients experienced fracture displacement while in the cast and were converted to closed pinning with a conversion rate of 8.5% (Fig. 2). There was a mean of 13.2 days (4 to 21) between initial treatment with casting to closed pinning. Five cases were changed to closed pinning from casting after four, 13, 14, 14 and 21 days. The mean casting duration was 26.5 days (11 to 56) for all non-surgical cases. The mean follow-up was 79.4 days (17 to 901) for patients treated non-surgically. The mean follow-up was 190.6 days (65 to 405) for patients converted from casting to closed pinning. The time from injury to first radiograph was a mean of 0.53 days (0 to 5).
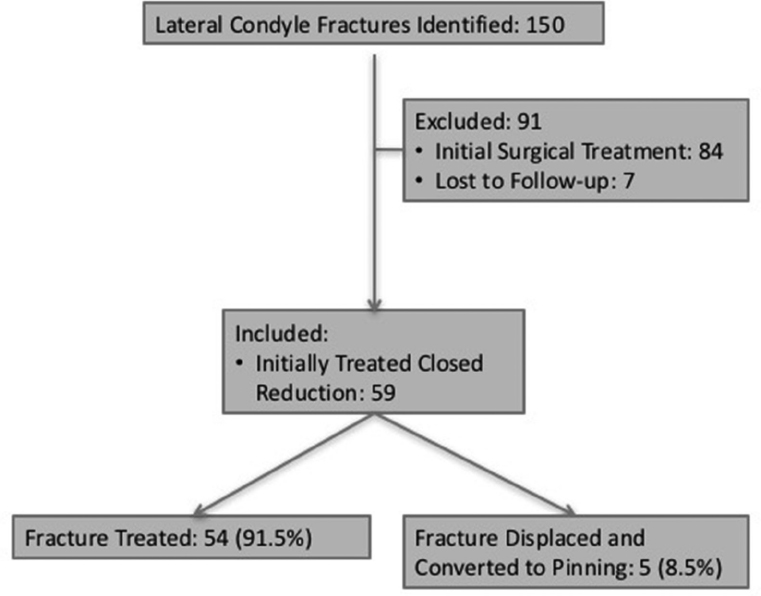
Breakdown of patients treated surgically and non-surgically for lateral condyle fractures.
Discussion
Fracture displacement is an issue for Jakob Type 1 fractures that extend all the way into the joint through the cartilage hinge. There are three potential causes of fracture displacement and conversion to closed pinning. First, movement in the cast when the swelling subsides can cause displacement. Secondly, if the child does not wear the sling as recommended, the fracture can displace as a result of movement. Thirdly, the fracture may displace when the surgeon removes the cast and moves the elbow for follow-up imaging. Due to the retrospective design of this study, we were not able to determine the reason for displacement in the five cases included in the current study. Fracture displacement can result in delayed healing and nonunion. Delayed fracture healing stems from synovial fluid exposure interposed into the intra-articular lateral condyle fracture. Continuous movement from the extensors of the wrist and fingers can impede healing and the extensors can rotate and displace the fracture. Late displacement of the lateral condyle can occur due to spasm or contraction of the extensors. Placing the arm in a long arm cast with the forearm supinated will theoretically relax the pull of the extensors at the wrist. Healing can also be delayed due to poor blood supply of the lateral condyle of the humerus.2,14,18
Badelon et al 10 observed a displacement rate of 18.8% for casted lateral condyle fractures < 2 mm (3/16). Devito et al 11 studied outcomes of paediatric patients treated non-operatively for lateral condyle fractures. The study included 51 fractures that were < 2 mm and six cases resulted in late displacement for a 12% displacement rate. Bast et al 12 reported that two patients out of 95 non-displaced lateral condyle cases treated with casting or splinting subsequently displaced in the cast and required surgery for a 2% treatment displacement rate. Pirker et al 13 obtained a displacement rate of 9.8% (5/51) for non-displaced lateral condyle fractures treated with casting. Knapik et al 17 conducted a systematic review and determined a risk of displacement of 14.9% from previous studies.14–17 This current retrospective study obtained an 8.5% displacement and conversion rate from cast treatment to closed pinning for initially non-displaced Jakob Type 1 lateral condyle fractures of the humerus.
Pirker et al 13 recommend radiographs out of the cast at a follow-up visit after four to six days for a non-displaced lateral condyle fracture. Skaggs and Flynn 19 also recommend removing the cast to obtain accurate radiographs of the fracture at follow-up appointments. Radiographs of the healing fracture out of the cast remove artifacts that obscure the fracture from the fiberglass cast. However, removing the patient from their cast each week may promote displacement of the fracture. A study has not been conducted to determine if the rate of displacement is significantly different for patients that are removed from their cast for imaging each week compared with patients that remain in their original cast for the entire time period.
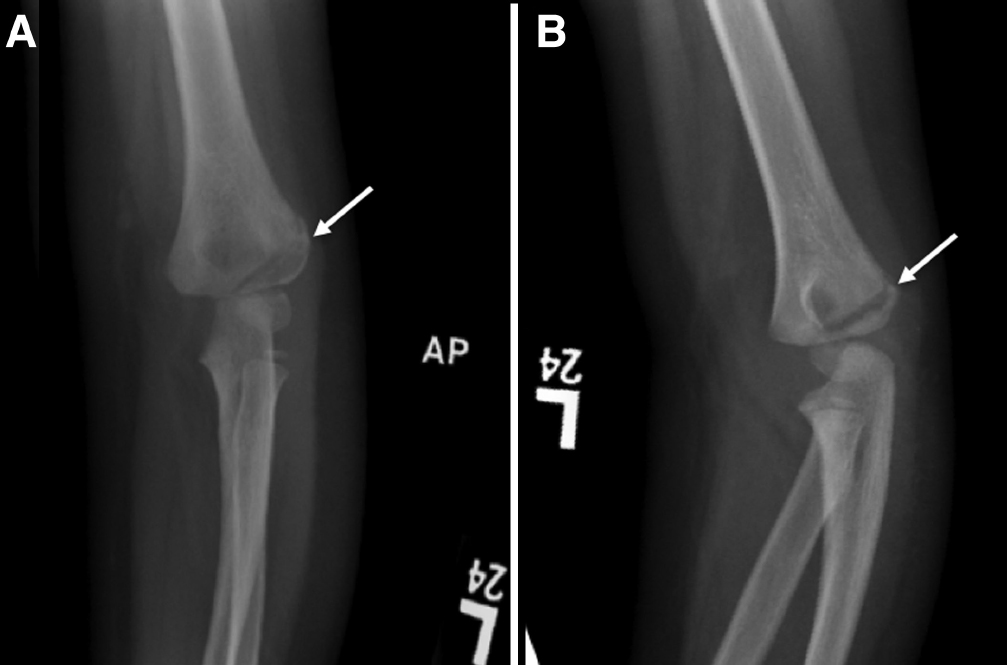
The internal oblique view is a key to diagnosis. Mahan 20 identifies the internal oblique radiograph as the required view for determining if a lateral condyle fracture is non-displaced or minimally displaced. Song et al 21 demonstrated that the internal oblique view was more accurate for determining fracture displacement and pattern when compared with the anteroposterior view in a prospective study of 54 lateral condyle fractures. Kurtulmus et al 22 also recommended that the internal oblique radiograph should be obtained at the first week of follow-up for conservatively treated patients to accurately visualize fracture displacement. In the current study, five lateral condyle fractures displaced on follow-up internal oblique radiographs within two weeks. One of the cases in the current study that displaced after initial casting did not include internal oblique views when the clinical decision was made. Anteroposterior and lateral radiographs were obtained at the initial evaluation for this patient. Anteroposterior and lateral radiographic views may falsely represent a minimally displaced lateral condyle fracture as a non-displaced lateral condyle fracture (Fig. 3). An internal oblique view should be obtained at the initial evaluation and at follow-up when there is suspicion of a lateral condyle fracture. We recommend obtaining an internal oblique view at two-week follow-up to determine if there is late displacement of the fracture.
(
Thompson and Zlotolow 23 recommend sling use with long arm casts and posterior splints for support to immobilize the joint above the fracture. Mercer Rang originally demonstrated a method for incorporating a sling loop into a long arm cast. 24 DeFroda et al 25 further described the method for incorporating a sling loop into a long arm cast. This method can improve patient sling compliance by improving sling fit and comfort, by increasing ease of sling reapplication and by promoting correct sling application. Sling recommendations can vary among doctors and patient compliance for sling use has not been investigated for closed treatment of lateral condyle fractures. Late displacement and treatment conversion rate may be reduced with sling use to support casting or posterior splint treatment for non-displaced lateral condyle fractures. Proper sling use will reduce movement at the elbow joint which contributes to late displacement of lateral condyle fractures.
Orientation of the forearm for long arm casting can affect lateral condyle fracture distance. Knutsen et al 26 demonstrated that lateral condyle fracture distance was shortest when the arm is placed in supination with a cadaveric model. We recommend applying a long arm cast with the elbow at 90º and the forearm in supination with a sling-loop design for the closed treatment of non-displaced lateral condyle fractures based on the cited literature (Fig. 4). While this recommendation is based on multiple individual studies and not the results of a large randomized control study, this recommendation provides effective treatment outcomes from our experience at this institution.

Application of a long arm cast in supination with a sling-loop design originally demonstrated by Mercer Rang (24).
Conclusion
Immobilization is a recommended initial treatment for patients with a lateral condyle fracture with < 2 mm displacement. Currently, a systematic review of published studies reports a displacement rate after closed reduction of 14.9% with a range of 2% to 51.9%. This current study demonstrates an 8.5% displacement and conversion rate from cast treatment to closed pinning for initially non-displaced Jakob Type 1 lateral condyle fractures of the humerus. We recommend obtaining an internal oblique view at initial evaluation and at follow-up in the cast for lateral condyle fractures. To minimize movement at the fracture site, we recommend treating Jakob Type 1 lateral condyle fractures in a long arm cast with the elbow at 90º and the forearm in supination with a sling-loop design.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.