
Abstract
Objective
To conduct a meta-analysis to show the associations of perioperative and postoperative outcomes of mini-plate internal fixation (MPIF) versus Kirschner wire internal fixation (KWIF) for treating metacarpal and phalangeal fractures.
Methods
A literature search was performed in PubMed, Web of Science, Cochrane Library, and Embase from the earliest date of data collection to April 2018. Studies that compared perioperative and postoperative outcomes of MPIF with those of KWIF in patients with metacarpal and phalangeal fractures were included.
Results
Twenty-six articles met the inclusion and exclusion criteria (n = 2029 patients; 1042 with MPIF and 987 with KWIF). MPIF was related to a greater increase in length of surgery, hospital days, excellent and good rate of outcome, short-form health survey-36 score, and flexion and extension range compared with KWIF. MPIF was related to a greater decrease in intraoperative blood loss, finger visual analog scale score, functional exercise time, fracture healing time, incidence of complications, and postoperative infection rate compared with KWIF.
Conclusions
Patients with MPIF have sufficient pressure and strength, and MPIF promotes successful joint fusion and reduces complications of the operation. MPIF is ideal for reduction and stability of patients with metacarpal and phalangeal fractures.
Keywords
Introduction
Metacarpal and phalangeal fractures are common in the emergency department of orthopedics. Among various type of metacarpal and phalangeal fractures, complicated fractures are more common.1–3 Many types of fixation materials can be used in treating metacarpal and phalangeal fractures, such as a mini-plate, Kirschner wire, and steel wire. 4 However, only a mini-plate and Kirschner wire are frequently used in surgery. Kirschner wire was the first fixation material to be used in the clinic, and intramedullary fixation with Kirschner wire has many advantages, such as being economical, minimal invasive, and easily available. 5 However, after years of practice, intramedullary fixation with Kirschner wire was found to have disadvantages, such as its unreliable fixation effect and high occurrence of surgical sequelae. 6 Therefore, the curative effect of Kirschner wire did not always satisfy doctors and patients. However, a mini-plate has many advantages, such as its stiffness, reliable fixation effect, and allowing exercise early postoperatively. 7 However, the mini-plate has many disadvantages, such as its high surgical cost, major damage to normal tissue, and requirement of secondary surgical intervention. 8
Recently, in China, mini-plate internal fixation (MPIF) and Kirschner wire internal fixation (KWIF) have been commonly used. Many researchers have already compared the curative effect of the mini-plate and Kirschner wire from different aspects.8–10 However, the sample sizes in these studies were too small. To date, researchers have not reached agreement on which type of fixation material should be used to treat metacarpal and phalangeal fractures. Therefore, this study aimed to evaluate the associations of perioperative and postoperative outcomes of MPIF versus KWIF.
Materials and methods
Literature and search strategy
Two reviewers independently searched PubMed, Embase, Web of Science, and the Cochrane Library for information from inception of the databases to April 2018. The following related terms were searched: metacarpal, phalangeal fracture, mini-plate internal fixation, Kirschner wire, Chinese, China. The search strategy was constructed by combining the above-mentioned terms with “AND” or “OR”. No restrictions were imposed on the language of studies. We also screened reference lists of retrieved articles so that relevant studies were not missed.
Study selection criteria
Two reviewers independently assessed the retrieved articles to determine whether they met the inclusion criteria. In case of disagreements, a third reviewer was involved in the discussion until a consensus was reached. The criteria for inclusion of papers selected for detailed review included the following: (1) the study was designed as a randomized, controlled trial or a retrospective study; (2) the study compared the effect of MPIF with KWIF for treatment of metacarpal and phalangeal fractures; (3) patients were adults (≥18 years old); and (4) the outcomes contained at least one evaluation of the length of surgery (minutes), intraoperative blood loss, hospital days, excellent and good rate of outcome, finger visual analog scale (VAS) score, short-form health survey (SF)-36 score, functional exercise time (weeks), fracture healing time (weeks), flexion and extension range, incidence of complications, and postoperative infection rate. Exclusion criteria included the following: case–control studies, animal studies, cadaver studies, single case reports, comments, letters, editorials, protocols, guidelines, publications based on surgical registries, and review papers; and inclusion of <10 patients for a clinical study.
The patients were divided into the MPIF group and KWIF group. We analyzed the study type (randomized, controlled trial, retrospective review, cohort study) and treatment methods described. The sample size in each study was extracted from the available information. Injury severity indicators as available were identified and analyzed. The study protocol was approved by the ethics committee of Tianjin First Center Hospital.
Data extraction and quality assessment
Two reviewers independently performed data extraction and methodological quality assessment. Data extracted from the included studies consisted of authors, publication date, study design, number of patients, and outcome data in the MPIF and KWIF groups. The outcome measures comprised the length of surgery (minutes), hospital days, excellent and good rate of outcome, finger VAS score, SF-36 score, functional exercise time (weeks), fracture healing time (weeks), flexion and extension range, incidence of complications, and postoperative infection rate. The methodological quality of the study was evaluated in seven domains, including sequence generation, allocation concealment, participants’ blinding, assessors’ blinding, incomplete data, selective reporting, and other bias. Each included study was considered as an unclear, low risk, or high risk of bias for each domain according to the Cochrane Handbook 5.1.0.
Statistical analysis
Statistical analyses were performed using Review Manager Software 5.3 (West China Hospital of Sichuan University, China, International Cochrane Collaboration). For dichotomous outcomes, the odds ratio (OR) with 95% confidence interval (CI) were calculated to estimate a pooled average difference between MPIF and KWIF. The weighted mean difference (WMD) and 95% CI were calculated for continuous outcomes. Statistical heterogeneity was quantitatively evaluated by the chi-square test with the significance set at P < 0.10 or I2 > 50%. The data are presented in the form of Forest plots.
Results
Literature search
The retrieval strategy is shown in Figure 1. Twenty-six articles met the inclusion and exclusion criteria. Among all of the participants in the 26 studies, the outcomes for 2029 patients were described, of which 1042 patients were treated with MPIF and 987 were treated with KWIF. The detailed characteristics of the studies are listed in Table 1. All articles were retrospective case reviews of hospital admissions. None of the studies used randomization. No other apparent bias was found among the included studies. Figures. 2 and 3 show the risk of bias summary.

Flow chart illustrating the literature search.
Characteristics of the included studies.

Note: when only one value is shown for MPIF and KWIF, it refers to MPIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation.

Risk of bias graph.

Risk of bias summary. + indicates a low risk of bias, − indicates a high risk of bias,? indicates unclear or unknown risk of bias.
Results of the meta-analysis
Fourteen studies reported the details of the length of surgery (minutes). Pooled results showed that MPIF was related to a greater increase in the length of surgery compared with KWIF (WMD = 1.07; 95% CI, 0.94 to 1.20; P < 0.001), without significant heterogeneity (I2 = 12%, P = 0.32) (Figure 4). Three studies reported the details of intraoperative blood loss. MPIF was related to a greater decrease in intraoperative blood loss compared with KWIF (WMD = −0.52; 95% CI, −0.81 to 0.24; P < 0.001), without significant heterogeneity (I2 = 0%, P = 0.54) (Figure 5). Thirteen studies reported the details of hospital days. MPIF was related to a greater increase in hospital days compared with KWIF (WMD=1.16; 95% CI, 0.94 to 1.37; P < 0.001), without significant heterogeneity (I2 = 33%, P = 0.12) (Figure 6).

Forest plot of comparison of the length of surgery (minutes) between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.

Forest plot of comparison of blood loss between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.

Forest plot of comparison of hospital days between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.
Twenty-five studies reported the details of an excellent and good rate of outcome. MPIF was related to a greater increase in the excellent and good rate of outcome compared with KWIF (OR=5.10; 95% CI, 3.97 to 6.55; P < 0.001), without significant heterogeneity (I2 = 0%, P = 0.67) (Figure 7).

Forest plot of comparison of an excellent and good rate of outcome between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.
Four studies reported the details of the finger VAS score. MPIF was related to a greater decrease in the finger VAS score compared with KWIF (WMD=−2.73; 95% CI, −2.64 to −1.90; P < 0.001), without significant heterogeneity (I2 = 49%, P = 0.12) (Figure 8). Three studies reported the details of the SF-36 score. MPIF was related to a greater increase in the SF-36 score compared with KWIF (WMD=2.88; 95% CI, 2.58 to 3.41; P < 0.0001), without significant heterogeneity (I2 = 18%, P = 0.29) (Figure 9).

Forest plot of comparison of the finger visual analog scale score between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.

Forest plot of comparison of the short-form health survey-36 score between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.
Three studies reported the functional exercise time (weeks). MPIF was related to a greater decrease in functional exercise time compared with KWIF (WMD=−1.87; 95% CI, −2.73 to −1.0; P < 0.001), without significant heterogeneity (I2 = 0%, P = 0.97) (Figure 10). Twenty-three studies reported the fracture healing time (weeks). MPIF was related to a greater decrease in fracture healing time compared with KWIF (WMD=−1.75; 95% CI, −1.90 to −1.60; P < 0.001), without significant heterogeneity (I2 = 36%, P = 0.04) (Figure 11).

Forest plot of comparison of functional exercise time (weeks) between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.

Forest plot of comparison of the fracture healing time (weeks) between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.
Four studies reported the flexion and extension range. MPIF was related to a greater increase in the flexion and extension range compared with KWIF (WMD=2.73; 95% CI, 2.43 to 3.03; P < 0.001), without significant heterogeneity (I2 = 49%, P = 0.12) (Figure 12).

Forest plot of comparison of the flexion and extension range between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.
Sixteen studies reported the incidence of complications. MPIF was related to a greater decrease in the incidence of complications compared with KWIF (WMD = 0.27; 95% CI, 0.19 to 0.38; P < 0.001), without significant heterogeneity (I2 = 0%, P = 0.92) (Figure 13). Twenty-four studies reported the postoperative infection rate. MPIF was related to a greater decrease in the postoperative infection rate compared with KWIF (WMD=0.24; 95% CI, 0.17 to 0.35; P < 0.001), without significant heterogeneity (I2 = 0%, P = 0.98) (Figure 14).
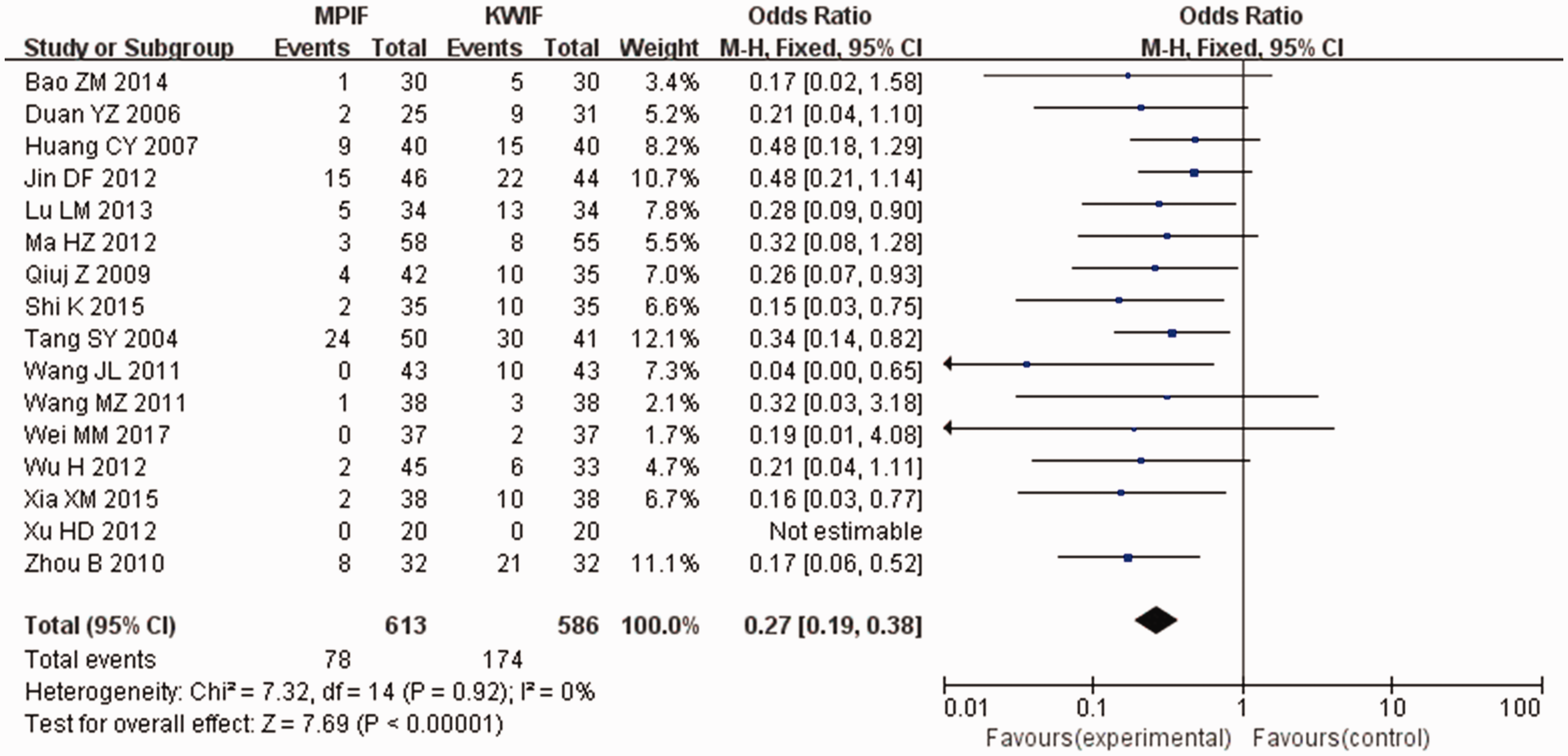
Forest plot of comparison of the incidence of complications between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.

Forest plot of comparison of the postoperative infection rate between MPIF and KWIF. MPIF=mini-plate internal fixation; KWIF=Kirschner wire internal fixation; CI=confidence interval; df=degrees of freedom.
Discussion
Previous studies have shown that the incidence of metacarpal fracture is 32%, proximal phalangeal fracture is 17.3%, middle phalangeal fracture is 5.7%, and distal phalanx fracture is 45%.11–15 If metacarpal and phalangeal fractures occur, proper treatment should be performed in time to avoid malformation and dysfunction.16–20 The traditional method of surgical treatment of metacarpal and phalangeal fractures is KWIF. The advantages of KWIF are a small incision, simple operation, small interference in the blood supply of the fracture, low cost, and simple internal fixation. However, KWIF easily becomes loose and slips, reliable fixation cannot be achieved, rotation is easy to control, there is easy separation between the fracture ends and the Kirschner wire often passes through joint fixation, and it is detrimental to early functional exercise.20–23 When the Kirschner needle is fixed, although stability is good, it can prevent rotation. However, there is no pressure effect at both ends of the fracture and this also affects healing of the fracture. Therefore, plaster fixation is required after the operation.24–27 The external fixation time of Kirschner wire is long, and it is easily complicated by joint stiffness, and malunion and nonunion, which seriously affect the rehabilitation of hand function. At present, most researchers in China believe that the mini-plate is superior to KWIF and other internal fixation methods.8–9 MPIF can firmly fix bone on the basis of anatomical reduction and it does not destroy the articular surface. Therefore, the function of the hand can be restored to the maximum.28–30
Application of MPIF has the following advantages. (1) MPIF has a wide range of indications, and it is applicable to the palmar finger and even part of the comminuted fracture in the joint. 31 (2) The mini-plate is firmly fixed without external fixation. In animal experiments, some researchers have found that MPIF is stronger than steel wire with resistance to bending, rotation, and pressure. 32 The mini-plate is strong enough to resist the pull of the muscles of the hand and is beneficial for opening of the wound. (3) Early functional exercise of the tendon can avoid adhesion. 33 (4) MPIF shortens the healing time of the fracture. 34 Minimizing pain and decreasing functional damage caused by trauma are helpful, which are beneficial to complete recovery of function of the hand.
In the clinic, internal fixation should achieve anatomical reduction, reliable internal fixation, and early functional training. At present, treatment of metacarpal and phalangeal fractures with MPIF in China and in other countries has shown good results. Healing of the fracture and the effect of recovering joint flexion by MPIF have been recognized.35–37 The mini-plate has high plasticity, can fully provide sufficient pressure and strength, promote the success rate of joint fusion, and reduce complications of the operation, and is the ideal material for reduction and stability of the tubular bone.38,39 MPIF has good biocompatibility, excellent corrosion resistance, no allergic conditions, and is beneficial to bone.
This systemic study showed the associations of perioperative and postoperative outcomes of MPIF versus KWIF for treatment of metacarpal and phalangeal fractures. The most important finding in our study was the clear difference in outcomes between MPIF and KWIF. Additionally, patients with MPIF benefit from thorough analysis and optimization of their medical condition. Further high-quality, multicenter, prospective studies with a good design and a large number of participants and long-term follow-up are required to confirm our results.
Footnotes
Acknowledgments
The authors would like to thank Tianjin First Center Hospital for providing the database.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.