
Abstract
Abstract
Purpose
The effect of surgical specialty on the outcomes of paediatric patients treated for displaced supracondylar humeral fractures remains unclear. The results of residents, paediatric surgeons and orthopaedic surgeons were compared.
Methods
A retrospective review of 108 children (0 to 16 years) treated for displaced humeral supracondylar fractures (Gartland II or III) requiring closed or open reduction under general anaesthesia were included. The patient charts and radiographs were evaluated to identify type, grade and neurovascular complications. Operative performance (operative time, quality of reduction, need for open reduction, complications) of residents, paediatric surgeons and orthopaedic surgeons were evaluated.
Results
Residents used a crossed pin configuration for patients in 25/25 (100%), paediatric surgeons in 25/32 (78%) and orthopaedic surgeons in 33/33 (100%) (p = 0.0011). Loss of reduction was present in one patient treated with crossed pins, in two with lateral pins and in two without Kirschner-wires (p = 0.0034). The risk ratio of an unacceptable reduction was 4.0 (95% confidence interval (CI) 0.90 to 18, p = 0.070) for residents and 6.6 (95% CI 1.6 to 27, p = 0.0082) for paediatric surgeons as compared with orthopaedic surgeons. Complications were present in 37% of patients (11/30) for residents, 55% (24/44) for paediatric surgeons and 15% (5/34) for orthopaedic surgeons (p = 0.0013).
Conclusion
We found statistically significant differences in the incidence of unacceptable reduction, complications and the usage of crossed pin configuration between the surgical specialties. Patients would benefit from the practice of assigning the operative treatment of displaced supracondylar fractures to orthopaedic surgeons.
Level of evidence
Level III
Introduction
Supracondylar fractures of the humerus are the most common elbow fractures in children, representing 70% to 75% of all paediatric elbow fractures, and are usually caused by falling on an outstretched hand.1–4 The fractures are divided into extension and flexion types, of which the extension type is more common, comprising 97% to 99% of the fractures.1,4 Complications associated with these fractures include preoperative nerve and vascular injuries, iatrogenic nerve injuries, reduced range of movement, decreased carrying angle and compartment syndrome.4,5
According to the modified Gartland classification, type I fractures show no displacement with a typical fat pad sign present, type II are angulated with the posterior cortex intact and type III are completely dislocated. 6 Dislocated fractures often require closed reduction with a percutaneous pin fixation (CRPP) to stabilize the site of the fracture either by crossed or lateral entry Kirschner (K)-wires.4,7,8 Acceptable reduction is indicated by the restoration of the Baumann angle (Flynn's criteria), the anterior humeral line passing the middle third of the capitellum and intact medial and lateral columns.9–11 A recent meta-analysis of Dekker et al 2 found no statistically significant difference between the outcome measured with Flynn's criteria in crossed pin and lateral entry configurations. Several studies have reported the crossed pin configuration as being more prone to iatrogenic ulnar nerve injury (4% to 6%), while the stability of the fracture and rate of loss of reduction were similar2,12,13 or better in a crossed pin configuration.14,15 Iatrogenic ulnar nerve complications can be avoided by exploring the nerve through a medial incision.16–18
Of the 118 compensation claims filed for complications in paediatric fractures in our country between 1990 and 2010, 74 (63%) were supracondylar humeral fractures. 19 The most common iatrogenic injury (0% to 4.9%) mechanism is the injury or irritation of the ulnar nerve by the medial pin.13,20 Malunion can cause a cubitus varus deformity, which is characterized as the loss of the Baumann angle and hyperextension of the humeral joint, and can be avoided by sufficient reduction and preserving the acceptable posture, which is most effectively done by using a K-wire fixation. 4 Deformity is the most common reason for compensation in supracondylar fractures in our country. 19 Cubitus varus was linked in several claims to more serious complications than cosmetic deformity; these included chronic pain, increased risk of lateral condylar fracture and ulnar nerve dysfunction.21–24
As a national characteristic in our country, the practice is for paediatric surgeons to operate on the majority of paediatric fractures, in contrast to orthopaedic surgeons in most other Western practices.19,25 We wanted to further evaluate the role of surgical specialty on the risk of complications by comparing the surgical performance and clinical outcomes between surgical residents, paediatric surgeons and orthopaedic surgeons and to also identify differences both in the techniques used and the quality of the treatment.
Patients and methods
This is a retrospective study of 134 supracondylar humerus fractures of patients under the age of 16 years who were treated under general anaesthesia at our facility between 2005 and 2015. Two intra-articular fractures and one polytrauma patient were excluded. Six adolescent patients undergoing plate fixation were also excluded. Eight patients that underwent primary olecranon osteotomy due to intra-articular fractures were also excluded. Two patients were lost in the follow-up after the surgery. We systematically evaluated the radiographs of the remaining 115 patients to specify the type of fracture, the Gartland classification and to measure the displacement. Non-dislocated Gartland I type fractures were then excluded (n = 7), leaving 108 displaced supracondylar fractures in the analyses (Gartland type II, n = 60 and type III, n = 48). Preoperational neurovascular status included palpation of radial pulse, warmth, swelling and the colour of the hand as well as detailed evaluation of the median, ulnar and radial nerves. 26 The fracture mechanism and time between the injury and surgery were recorded.
The operative performance was evaluated between residents, paediatric surgeons and orthopaedic surgeons by comparing the operation time, the pin configuration used, the type (closed versus open) and quality of reduction used and the incidence of complications. The residents were paediatric surgical residents, who all had a minimum three years of surgical experience before entering the university hospital.
Anteroposterior and lateral radiographs taken preoperatively, intraoperatively as well as postoperatively were evaluated by the first author (AJS) blinded to the specialty or surgical expertise level of the operating surgeon. The division between extension and flexion type injuries was made with the displacement of the distal fragment of the humerus in the lateral radiograph. 4 The anterior and lateral displacements, along with the distance from the anterior humeral line to the capitellum, were measured. Unsatisfactory reduction was defined by Flynn's criteria: Baumann angle of < 10°, dislocations > 4 mm or 25% and any anterior humeral line that did not bisect the capitellar ossification centre.4,11 Control radiographs taken one month after the surgery along with patient charts were used to evaluate the radiographic outcome. The mean duration of the clinical follow-up was 5.88 months (0 to 6 years).
The complications included: those that were wound related, neurovascular, unsatisfactory reductions, the need for re-operation other than K-wire removal and compartment syndrome.
Statistical analysis
This was performed using Pearson's chi-squared test, analysis of variation (ANOVA) and t-tests. A p-value of 0.05 was considered as statistically significant. Relative risk (RR) was calculated with the orthopaedic surgeons being used as the reference.
Results
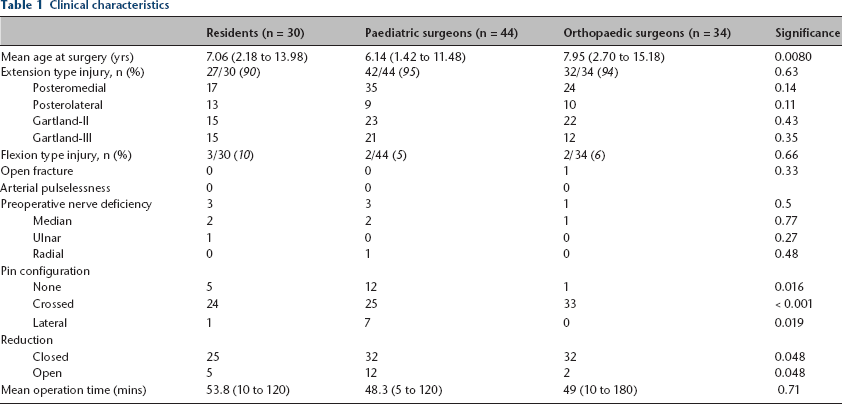
In all, 18 (17%) patients were treated by closed reduction without pinning under general anaesthesia. A total of 70 (65%) patients were treated with closed reduction and percutaneous pinning and 20 (19%) with open reduction and percutaneous pin fixation, 82 of which were crossed pin and eight lateral entry configurations. A long arm cast was used in all of the patients. The mean cast immobilization time was 29 days (9 to 51). A total of 67 (62%) patients received a prophylaxic intravenous cefuroxime. Of the fractures, 101 (94%) were the extension type (Tables 1 and 2). The mean age at surgery was 7.0 years (1.4 to 15). In all, 71 (66%) patients were male. The most common injury mechanism was falling on an outstretched hand. Seven patients with preoperative neural dysfunction were recorded. One child presented with an open fracture. One preoperative vascular injury was recorded (cold, pale hand). No preoperative compartment syndromes were recorded.
Clinical characteristics
Radiographic outcomes

AHL, anterior humeral line
Nine (8.3%) postoperative ulnar nerve deficiencies were recorded, all of which were treated with crossed pin fixation. Eight of them fully recovered. Six patients required the removal of the medial pin due to irritation of the ulnar nerve. One patient presented with a permanent ulnar nerve dysfunction at the one-year follow-up, in which an electroneuromyography (ENMG) study showed axonal damage to the ulnar nerve and distal radial nerve dysfunction. Four (6.2%, 4/65) patients with exposure of the ulnar nerve versus five (20%, 5/25) without exposure, developed an ulnar deficiency postoperatively (p = 0.050).
None of the patients had postoperational vascular complications. One compartment syndrome, due to improper casting, was recorded. None of the patients developed a deep wound infection.
Surgical expertise
Residents operated on 30 (28%) of the patients, paediatric surgeons on 44 (41%) and orthopaedic surgeons on 34 (31%). Residents used K-wires in 83% (25/30) of the patients, paediatric surgeons in 72% (32/44) and orthopaedic surgeons in 97% (33/34) (p = 0.017). Of these children, the residents used a crossed pin configuration in 25/25 (100%) of the patients, paediatric surgeons in 25/32 (78%) and orthopaedic surgeons in 33/33 (100%) (p = 0.0011). The mean operative time was 54 minutes (10 to 120) for the residents, 48 minutes (5 to 120) for the paediatric surgeons and 49 minutes (10 to 180) for the orthopaedic surgeons (ANOVA, p = 0.71).
Risk of complications and surgical expertise
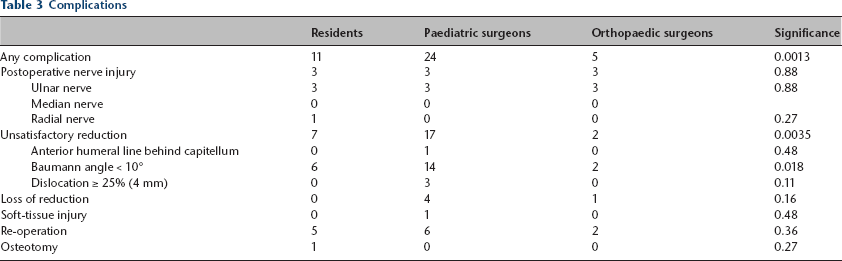
Open reduction was performed more often by residents (RR 2.8, 95% confidence interval (CI) 0.59 to 14) and paediatric surgeons (RR 4.6, 95% CI 1.1 to 19) as compared with orthopaedic surgeons (p = 0.048). Complications were present in 37% (11/30) of the patients treated by the residents, 55% (24/44) of those treated by the paediatric surgeons and 15% (5/34) of the patients treated by the orthopaedic surgeons (p = 0.011) (Table 3). An unsatisfactory reduction was present in seven (23%, RR 4.0, 95% CI 0.90 to 18, p = 0.070) of the residents’ patients, in 17 (39%, RR 6.6, 95% CI 1.6 to 27, p = 0.0082) patients of the paediatric surgeons, and in two (5.9%) patients of the orthopaedic surgeons. The anterior humeral line was behind the capitellum in none of the patients operated on by the residents, in one patient operated on by the paediatric surgeons and in none of the cases operated on by the orthopaedic surgeons (p = 0.48). No lateral dislocations of over 4 mm or 25% were present in the patients of the residents or orthopaedic surgeons (p = 0.11) but present in three (6.8%) patients of the paediatric surgeons. Varus malalignment (Baumann angle < 10°) was present in six (20%) patients treated by residents, 14 (32%) patients treated by paediatric surgeons and two (5.9%) patients treated by orthopaedic surgeons (p = 0.018). The mean Baumann angle was 14.8° with residents, 15.2° with paediatric surgeons and 17.4° with orthopaedic surgeons (ANOVA, p = 0.43) (Table 2). There were seven flexion type of fractures in the current series. Of them, three were operated on by residents and two each by paediatric surgeons and orthopaedic surgeons (not significant).
Complications
Risk of re-operation
In all, 13 (12%) patients required re-operation: three due to an unsatisfactory primary operation, five due to loss of reduction and five due to neural injury. Of these, five patients were operated on by a resident, six by a paediatric surgeon and two by an orthopaedic surgeon (p = 0.36). One patient with loss of reduction was treated with a crossed pins configuration, two with lateral entry and two without pinning (p = 0.0034). Loss of reduction was present in none of the patients treated by residents, in four (4/44, 9.1%) patients treated by paediatric surgeons (two lateral entry configuration and two without pins) and in one (1/34, 2.9%) patient by orthopaedic surgeons (crossed pin configuration, p = 0.16). One patient operated on by a resident required osteotomy to correct a clinically significant cubitus varus deformity.
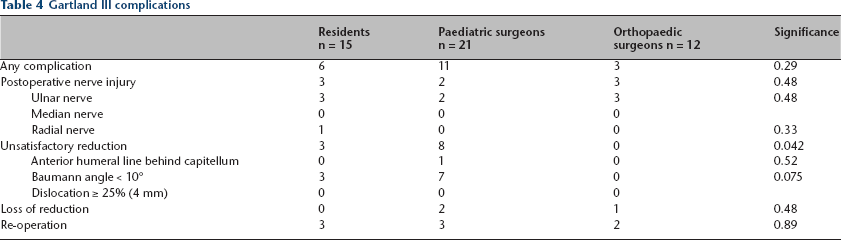
A subgroup analysis on Gartland type III fractures
A subgroup analysis on Gartland type III fractures (n = 47) was performed (Table 4). The risk of unsatisfactory reduction was significantly higher in the paediatric surgeons than in the orthopaedic surgeons (p = 0.042). There were no statistically significant differences in the occurrence of neural injuries, loss of reduction or re-operation.
Gartland III complications
Discussion
Supracondylar humerus fractures are common fractures in children. CRPP is the standard care for displaced supracondylar fractures, while the configuration of the pins remains under debate. 11 Risk of unacceptable reduction and complications were significantly less common in children operated on by an orthopaedic surgeon when compared with surgical residents or paediatric surgeons.
Limitations
The study design was a retrospective study on consecutively operated on children for displaced supracondylar humeral fractures. The analyses were conducted blinded by an independent observer (AJS). The number of patients (n = 108) was relatively limited. In general, there is a tendency for more difficult fractures to be assigned to more senior surgeons and also more severe injuries are typically treated at university hospitals, which may have induced selection bias. We evaluated the quality of the surgical treatment for the patients with supracondylar fractures treated at our institution with a special interest in the specialty of the physician. Due to a relatively short follow-up time it was not possible to determine the long-term outcome of the patients. An unsatisfactory carrying angle does not remodel after ossification, thus resulting in a permanent cubitus varus deformity which may require osteotomy. 27 We did not include the clinical carrying angle measurements as the Baumann angle is considered a reliable indicator of the outcome of a supracondylar fracture. 28 In our country, crossed-pin fixation is widely used as the standard configuration by paediatric orthopaedic surgeons. 10
Comparison with previous studies
Recently, Tuomilehto et al 29 reported a slightly higher rate of complications but no differences in the quality of reduction between residents and senior orthopaedic surgeons, although the findings were not statistically significant. Our study showed a significantly higher risk of complications in patients operated on by paediatric surgeons (55%) than by orthopaedic surgeons (15%), and the residents (37%) were between these two groups. Mangwani et al 30 reported an open reduction rate of 22% when 75% of patients were operated on by a resident which is similar to our findings but significantly lower when compared with orthopaedic surgeons.
According to Kasser 31 in 1999, 68% of the supracondylar humeral fractures were treated by orthopaedic specialists in New England. According to a recent study, 71% of the patients with Gartland III type fracture were operated on by a senior orthopaedic surgeon in Helsinki Children's Hospital between 2002 and 2006 and 2012 and 2014. 10 According to our study, only 31% of all fractures and 25% of Gartland III type fractures were treated by orthopaedic surgeons. A study by Holt et al 25 reported significantly higher rates of surgery and lower rates of complications in teaching hospitals, trauma centres and metropolitan hospitals as compared with community and local hospitals. Vallila et al 19 reported the lowest incident of complications in paediatric distal humerus fractures in university hospitals.
Older studies have reported considerably higher rates of unsatisfactory reduction (17% to 50%)16,32,33 as compared with our findings (25% total, 5.9% orthopaedic surgeons). A higher rate of CRPP was linked to better clinical outcomes and fewer complications, 34 most of which could be avoided by appropriate care. 19 Contrary to the overall decrease in the number of paediatric fractures, upper arm fractures have increased. 35 As surgical treatment has been shown to be increasing in recent years,36,37 allocating patients to orthopaedic specialists has indicated a decrease in the incidence of complications.19,25 Based on the findings of this study, all paediatric fractures are currently treated by orthopaedic surgeons in our institution.
Several studies have found a crossed pin configuration more stable than a lateral configuration.15,38,39 Exploration of the ulnar nerve through a small incision seems to prevent neural injury when adding the medial pin.17,18 Patients treated with a crossed pin configuration had less loss of reduction, according to our study. Loss of reduction was most unlikely in patients treated by orthopaedic surgeons, who treated all patients with crossed pins, however, the finding was not statistically significant.
Conclusions
The risk of unacceptable reduction and complications were significantly higher in children operated on by paediatric surgeons rather than orthopaedic surgeons. There was no significant difference in the incidence of the re-operation between the specialties but open reduction was performed significantly more often by paediatric than orthopaedic surgeons. Operative treatment of paediatric supracondylar fractures should be assigned to orthopaedic surgeons.
Footnotes
I. Helenius: Study concept, critical review of the manuscript.