
Abstract
Purpose
Intramedullary rodding is indicated for patients with osteogenesis imperfecta (OI) to manage deformity and help treat recurrent fractures. Historically, the focus of intramedullary stabilisation has been the lower extremity. Here we report our experience of intramedullary rodding of the humerus and forearm in children with OI and its impact on the fracture rate of those bone segments.
Patients and Methods
This is a retrospective chart review of all OI patients who have undergone re-alignment and intramedullary rodding of the humerus or forearm between October 1994 and February 2016. Patient demographics, surgical information, complications and pre-operative and post-operative fracture rates were gathered.
Results
A total of 45 upper extremity segments (26 humeri, 19 forearms) were rodded at an average age of 8.7 years (3.1 to 19.2). Of these, 15 (33.3%) of the bone segments required a return to the operating room at a mean 30.8 months (1 to 90) post-operatively. Fracture data was available for 24 of the bone segments. The average number of pre-operative and post-operative fractures was 3.58 (SD 2.84) and 0.46 (SD 0.72) respectively. The average pre-operative and post-operative fracture rates were 0.87 fractures/year (SD 0.47) and 0.10 fractures/year (SD 0.16) respectively.
Conclusion
In this OI population, re-alignment and rodding appeared to reduce the fracture rate of the humerus and forearm. Among our population, one third returned to the operating room and one fifth required revision to a new intramedullary implant. This data may help families better understand the potential outcomes of upper extremity realignment and rodding and its effect on the rate of upper extremity fractures.
Keywords
Introduction
Osteogenesis imperfecta (OI) is a heritable disorder characterised by bone fragility, short stature, frequent fractures, long bone deformity, and other connective tissue manifestations. 1 The concept of long bone deformity correction by means of multiple re-alignment osteotomies and intramedullary rodding was described initially by Sofield and Millar. 2 Re-alignment and intramedullary rodding remains the mainstay of surgical treatment for long bones in children with OI, albeit with less invasive techniques, increased reliance on fluoroscopic guidance, and the option of telescopic rods. 3
Although Sofield and Millar's initial report 2 included a description of the re-alignment and rodding procedure for both the humerus and the ulna in the setting of OI, the focus of long bone surgery for children with OI has historically been the lower extremity. Cases of upper extremity re-alignment and rodding have been included in historical OI case series4–7 and have been the focus of other reports in the OI literature.8,9 Ashby et al10,11 reported on the functional improvements of their OI patients who have undergone humeral and forearm rodding. The purpose of this review was to seek the answers to two questions frequently faced when counseling OI patients with upper extremity fractures and deformity: 1) How long will the upper extremity rodding last and what are the chances of a revision; and 2) How will rodding the humerus or forearm affect the fracture rate of those bone segments?
Patients and Methods
This is a retrospective review of all patients with OI at our institution who underwent humeral or forearm rodding between October 1994 and February 2016. The study was approved by the Institutional Review Board. Patient records were reviewed for patient demographics, surgical information, surgical revisions, and complications.
Fracture data
Fracture data were gathered from patient charts. All fractures of the upper extremity bone segments that underwent rodding were recorded. A fracture of either the radius or ulna or both bones was included as a forearm fracture. Both pre-operative and post-operative fractures were recorded for all primary upper extremity rodding procedures. The dates of the fractures were recorded to calculate the pre-operative and post-operative fracture rates as the number of fractures per year. Fracture numbers and rates were only tabulated for patients with sufficient documentation of fracture history at each visit with our orthogeneticist (MBB) and at visits with the senior author (RWK). It is our practice to treat our OI patients with fractures on a daily basis in our fracture clinic. Fractures that were not reported to our multidisciplinary OI team or treated in our fracture clinic were not included in the data. In utero fractures and those diagnosed at birth were not included. The denominator (in years) for the pre-operative fracture rate included the number of years from the first fracture of the operative bone segment to the date of the rodding. The lowest denominator used was one year.
Surgical treatment
The most common indication for re-alignment and rodding of the upper extremity was progressive deformity and recurrent fractures causing interference with functional abilities. Other indications included nonunion or acute fracture. For patients with severe pre-operative deformity, evaluation by an occupational therapist helped assess hand functional ability. All surgical procedures were performed by the senior author (RWK).
For both humerus and forearm surgery, the patients were in a supine position. The endotracheal tube was directed opposite the operative upper extremity. The ability to obtain unobstructed fluoroscopy views was confirmed. In patients with severe shoulder deformity, the preferred approach was retrograde through the lateral column of the elbow. The antegrade approach through the deltoid and supraspinatus muscles was used for patients in whom a Fassier-Duval rod (Pega Medical, Quebec, Canada) was placed. When the male component of the Fassier-Duval rod was used without the telescoping female component, it was placed in retrograde fashion. Radius rods were placed through a distal approach just proximal to the distal radial physis. The starting point for the ulnar rods was proximally just lateral to the tip of the olecranon. For some patients with particularly small and tortuous intramedullary canals in the forearm, if the forearm was stable following the placement of one intramedullary rod, the other forearm bone was not rodded. Pre-operative planning considered the shape of the bone, the diameter of the bone, and the location of the deformity. The type of implant was determined by canal size and bone quality. The smallest number of osteotomies that permitted passage of the intramedullary device were performed. Osteotomies were performed through open approaches to visualise and protect neurovascular structures. Dissection was minimised when possible by using a guide wire as an intramedullary joystick. Osteotomies were performed with a rongeur or by creating multiple drill holes and completing the cut with an osteotome. To avoid thermal injury, a saw was not used to osteotomise the bone. Patients who underwent re-alignment and rodding of the humerus were immobilised in a long arm cast or splint with a swathe to immobilise the shoulder. Patients who underwent re-alignment and rodding of the forearm were immobilised in well-padded long arm casts.
Results
A total of 45 long bone upper extremity segments (26 humeri and 19 forearms) in 24 patients were re-aligned and rodded at an average age of 8.7 years (3.1 to 19.2). Ten of the patients were males and 14 were females. 21 patients had OI type III, two patients had OI type I, and one patient had Bruck syndrome. All but seven of the patients were treated with bisphosphonate therapy. The indication for surgery for 41 of the upper extremity segments was progressive deformity and recurrent fractures causing interference with functional abilities. One patient underwent rodding of the humerus to treat a distal humerus nonunion. Three patients (two forearms and one humerus) underwent re-alignment and rodding as treatment of an acute fracture.
The intramedullary implants used for the patients who underwent humerus re-alignment and rodding are shown in Table 1. Of the patients who underwent forearm re-alignment and rodding, intramedullary implants were placed in both the radius and the ulna for ten patients, in the radius only for three patients and in the ulna only for six patients. The intramedullary implants used in the forearm included Kirschner wires or flexible intramedullary nails.
Humerus intramedullary implants
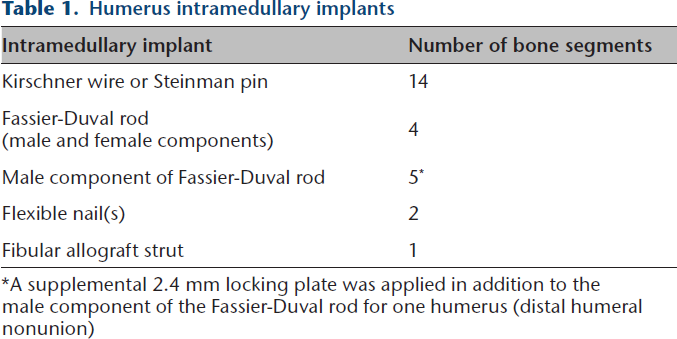
A supplemental 2.4 mm locking plate was applied in addition to the male component of the Fassier-Duval rod for one humerus (distal humeral nonunion)
A total of 15 (33.3%) of the upper extremity bone segments (eight humeri and seven forearms) required a return to the operating room at an average of 30.8 months post-operatively (1 to 90) during a mean follow-up 5.6 years (sd 3.8 years). One additional patient with type I OI returned to the operating room on an elective basis for removal of forearm flexible nails. Nine (20.0%) of the upper extremity bone segments required a revision to a new intramedullary device at an average of 44.4 months post-operatively (6.4 to 90) (Fig. 1).
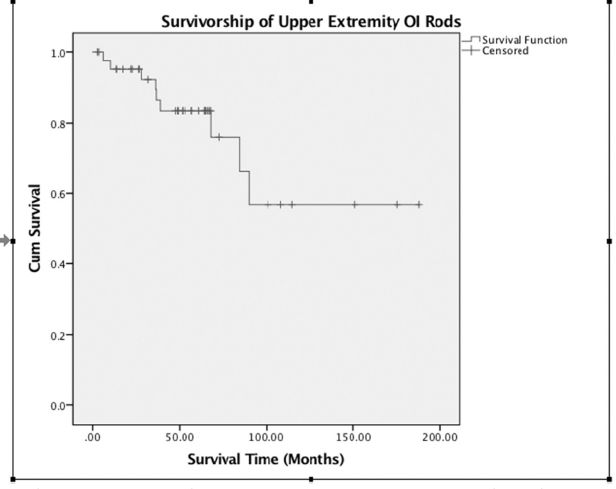
A survival curve demonstrating return to the operating room for revision to a new intramedullary device for nine of the 45 upper extremity bone segments at an average of 44.4 months (6.4 to 90) post-operatively.
Two of the early humeri in the series required trimming and impaction of prominent Steinman pin implants and then went on to each require two more rod revisions. Another early humerus in the series in a four-year-old girl fixed with a Kirschner wire went on to require revision osteotomy and rodding due to recurrent deformity 37 months post-operatively. One Kirschner wire in the humerus that had been inserted in antegrade fashion caused shoulder pain with subacromial impingement and was removed 85 months post-operatively. A Kirschner wire in the humerus of a five-year-old girl went on to be prominent with deformity recurrence and was revised to two Kirshner wires with repeat osteotomy ten months post-operatively. More recently, two of the humerus rodding patients experienced discomfort at the distal site of a Kirschner wire implant and one at the distal site of a flexible nail implant, and the fixation has been revised to a male component of a Fassier-Duval rod. So far, none of our primary humeri fixed with a Fassier-Duval rod (both components) or the male component of a Fassier-Duval rod have required revision (mean follow-up, 45.7 months; 14 to 68).
Of the seven forearm revisions, four included rod cutting and/or impacting to treat rod prominence (two ulnar rods at the elbow, one forearm with a prominent radial rod at the wrist and ulnar rod at the elbow, and one radius with rod prominence at the wrist). Three forearms required revision re-alignment and rodding due to refracture with rod bending. In all three instances, there was a traumatic episode that caused the refracture.
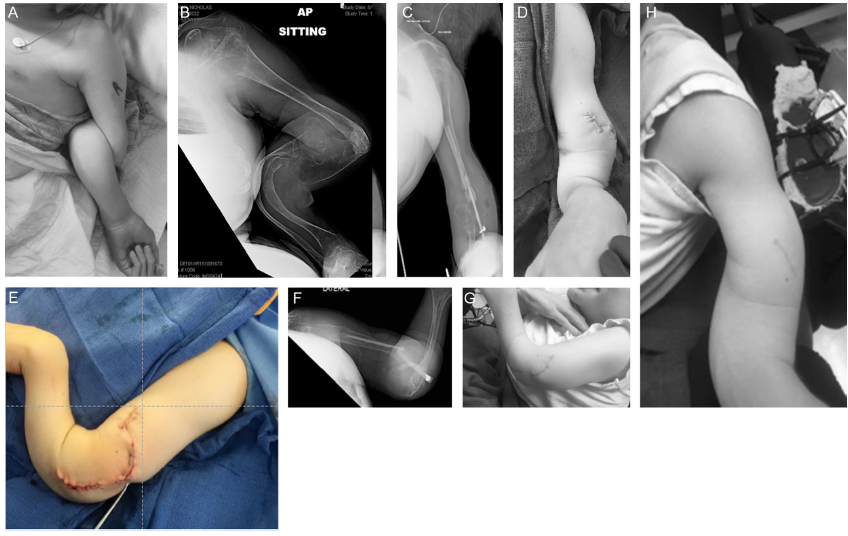
There were two additional complications that did not require return to the operating room. A 19-year-old man with type III OI with a severe humeral deformity (Figs. 2a and b) underwent re-alignment of the humerus, and, due to the friability of the bone, overlapping fibular strut inlay grafts were used as intramedullary fixation with a screw and washer placed distally (Figs. 2c to e). Four months post-operatively, his radiographs demonstrated 40° of angulation of the strut allografts (Fig. 2f). He reported no discomfort, and both the aesthetics and functionality of his arm were much improved. One patient presented with protrusion of the ulnar rod through the skin at the elbow four months post-operatively and underwent removal of the rod at the bedside. No neurovascular injuries or infections were encountered.
(
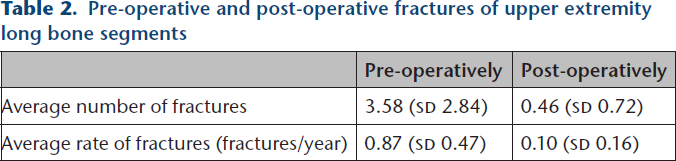
Fracture data were available for 24 of the long bone segments (14 humeri and ten forearms). The average number of pre-operative and post-operative fractures for each segment that underwent re-alignment and rodding was 3.58 (SD 2.84) and 0.46 (SD 0.72), respectively. The average pre-operative fracture rate was 0.87 fractures/year (SD 0.47), and the average post-operative fracture rate was 0.10 fractures/year (SD 0.16) (Table 2). Figure 3 demonstrates the pre-operative and post-operative left humerus radiographs of a seven-year-old boy with severe OI who had nine fractures over a six-year period pre-operatively (1.5 fractures/year) and two fractures over a 5.25-year period post-operatively (0.38 fractures/year).
Pre-operative and post-operative fractures of upper extremity long bone segments

(
Discussion
In our OI population, re-alignment and rodding of the humerus and the forearm reduced the fracture rate of those upper extremity bone segments. In the upper extremity bone segment that was rodded, our patients were experiencing, on average, almost one fracture per year pre-operatively and experienced an almost ten-fold reduction in that fracture rate following re-alignment and rodding.
In their series of 13 patients with OI treated with the multiple osteotomy technique, re-alignment, and intramedullary rod fixation, Tiley and Albright 6 reported on 13 humerus and 11 forearm procedures among a total of 112 long bone procedures. When recurrent fractures were the principal indication for the procedure, they found the re-alignment and rodding operation “almost uniformly interrupted the cycle of fracture and deformity.” Mulpuri and Joseph 12 reported on fracture data in their report of 16 children with OI who underwent intramedullary rodding of long bones during a ten year period, including 66 lower limb segments and five humeri. Although not broken down by upper or lower extremity, they found a pre-operative fracture rate of 2.63 fractures per person per year and a post-operative fracture rate of 0.04 fractures per person per year in their elongating rod group. In their non-elongating implant group, they found a pre-operative fracture rate of 1.58 fractures per person per year and a post-operative rate of 0.21 fractures per person per year.
One-third of the patients in our population required return to the operating room and one-fifth required revision of the intramedullary device. A common source of concern in populations such as this one, with a predominance of severe OI and poor bone quality, has been rod migration and rod prominence. This experience parallels that of many historical and current series in similarly severe OI populations and seems to be fairly consistent across both the lower and the upper extremity.13–17 In their series of seven humeral roddings for patients with severe OI, Gargan et al 9 noted two patients with protrusion of a Kirschner wire through the skin distally, requiring re-operation to trim the end of the wire. Ashby et al 10 noted prominent hardware in seven (five Kirschner wires and two Fassier-Duval rods) of their 35 primary procedures in their report on the functional outcome of humeral rodding in their OI population. In their parallel report on the functional outcome of forearm rodding, including 22 procedures in 19 children, they noted six of 17 (35%) ulna Kirschner wires and two of 21 (10%) radial Kirschner wires were prominent and required removal or advancement. 11
Given the significant revision rate as well as the technical difficulty of realigning and obtaining fixation in patients with severe deformity and poor quality bone, the indications for upper extremity re-alignment and rodding must not be taken lightly. We are constantly seeking ways to decrease the need for return to the operating room. In the humerus in particular, we have noted distal rod migration and prominence to be a common cause of return to the operating room. We have developed a preference for fixation through the lateral column of the humerus to avoid potential risk to the ulnar nerve with rod prominence or migration of a rod inserted through the medial column. We have seen a decreased revision rate with Fassier-Duval instrumentation for the humerus. Even when unable to use both components of the Fassier-Duval rod due to the size of the canal or protrusion of the acromion, our preference is to use at least the male component of the Fassier-Duval rod in retrograde fashion. Retrograde insertion helps us to avoid disruption of the rotator cuff as well as subacromial pain that can be a complication of antegrade insertion. The threaded fixation of the male component of the Fassier Duval rod in the proximal humeral epiphysis helps to prevent rod migration distally. Supplemental fixation in the form of a plate and screw construct at an osteotomy site improves rotational control and is particularly useful in the setting of a nonunion. The advent of locking plate technology facilitates this form of supplemental fixation with an intramedullary rod in place.18,19
It must be emphasised that upper extremity deformity alone, which is present in 37% of OI patients and even more common among those with severe OI, 20 is not an indication for re-alignment and rodding. The effect of the deformity on functional abilities and the effect of recurrent fractures on quality of life must be considered. We are encouraged by the positive effects on functional outcome measures reported by Ashby et al10,11 in their humerus and forearm OI rodding populations. Although we have not reported on functional evaluation data, we do feel that hand function evaluation by an occupational therapist is an important part of the pre-operative evaluation of those with severe deformity. In particular, it helps predict the abilities of the hand once it is in a more functional position post-operatively. The surgical interventions described here are just one small piece of the multidisciplinary care required to maintain and improve the functional abilities of our OI patients.
This study has several limitations. Although the majority of the patients included had a severe form of OI, it is a somewhat heterogeneous population. Additionally, this is a retrospective review without a control group. Although fracture rates were only calculated for patients with a detailed fracture history performed at each visit with our orthogeneticist, many fractures in the OI population may go undocumented. This may result in fracture numbers and rates lower than the true values. We do not believe this likely under documentation has skewed the reduction seen in fracture rates. Based upon our experience, we do believe it is more likely for patients to report a fracture in a post-operative bone segment than those in an un-operated bone segment and thus do not believe that this study over emphasises the reduction in fracture rates. Despite these limitations, this review of our experience helps us guide our patients and families regarding the revision rate and the effect on fracture rate of upper extremity re-alignment and rodding in the setting of OI.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical Approval: Ethical Approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
This study was not funded.