
Abstract
Ever since the introduction of spinal fusion in 1911, the procedure has continued to evolve and improve as the demand of the aging population increased and as new technological advances emerged. With better technology and better instruments, spine surgeons have been able to develop newer and better approaches that achieve stable constructs but with less morbidity. This article will discuss the advantages and complications associated with each of the approaches, including the anterior, posterior, laparoscopic, axial approach, lateral, minimally invasive, and oblique approach. Ultimately, there seems to be no clear advantage to using one approach over another as they all carry similar risks. There has been an increase in interest in more minimally invasive approaches as these present shorter operative times and less morbidity; however, these approaches are newer and present a steep learning curve with little long-term data on efficacy and safety.
Since the introduction of spinal fusion in order to treat tuberculous spondylitis in 1911 by Hibbs and Albee, the potential surgical applications of spinal fusion have grown to include progressive scoliosis deformity, tumor, fractures, and degenerative conditions. 1 , 2
Various methods of lumbar fusion have been proposed in order to relieve axial low back pain. Of all the methods available to surgeons for lumbar fusion, there seems to be an increased number of lumbar interbody fusions over the past 5 years. Interbody fusion increases the chance of fusion and also has a biomechanical advantage. The anterior column has to bear about 80% of axial load in the spine. Ani et al. first discussed the significance of the anterior column, which was also supported by Lowery and Harms. 3 , 4 The use of interbody support provides structural stability, and the system becomes load sharing as opposed to load transferring. This helps provide a stimulus for healing according to Wolff’s law, which dictates that healthy bone will adapt to the load under which it is placed. An interbody fusion also helps to prevent screw-bone interface strain. First published in 1944 by Briggs and Milligan, lumbar interbody fusion initially had little success without combined instrumentation. 5 They described the procedure using bone chips from the laminectomy as graft to facilitate fusion. Their technique resulted in many graft failures and subsidence, which led to the investigation of the utility of interbody cages. Interbody cages were developed to prevent graft collapse and loss of interspace height.
Despite the rapid development of lumbar interbody fusion techniques with innovative interbody cages, lumbar interbody fusion is not without complications. There have been sporadic reports regarding complications associated with lumbar interbody fusion, mostly limited to specific approaches and techniques. Therefore, this review will discuss the complications of lumbar interbody fusion. Each complication, as well as prevention of those complications, will be discussed in relation to the different surgical approaches.
Anterior Approach
Anterior lumbar interbody fusion (ALIF) is indicated for spine fusion, psoas abscess drainage, biopsy or resection of a vertebral body, and intervertebral disc replacement. It allows access from L1 to the sacrum and involves an incision from the posterior half of the 12th rib to the lateral border of the rectus abdominis muscle. The vertebrae are exposed by way of dissection through the abdominal musculature, retraction of the peritoneal cavity and ureter, and ligation of segmental lumbar arteries in the operative field (Fig. 1). This approach has been suggested to be an excellent option to treat degenerative disc disease in selected patients. One of the initial Food and Drug Administration trials showed up to a 95.1% fusion rate in 4 years. 6 However, as suggested by McAfee and Towson, the surgical outcomes depend heavily on surgeon factors. 7
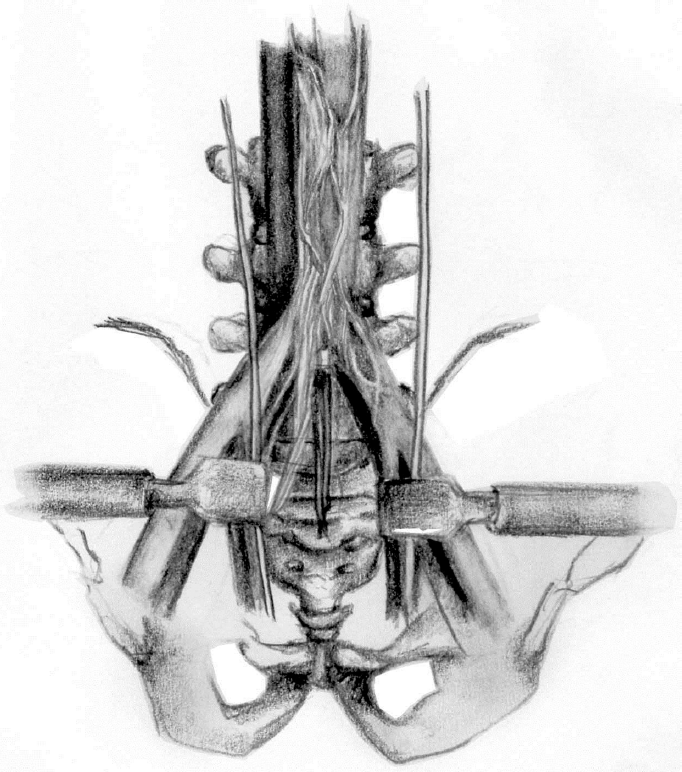
Relevant anatomy to the anterior approach of the lumbar spine. Illustration by Rachel Hong-Kei Ho
A study that was presented by O’Dowd et al. showed a high rate of complications when lumbar interbody fusion was performed using an anterior approach, including major vessel injuries and psuedarthrosis. 8 A review of vascular complications of the anterior exposure noted a 6.1% rate of intraoperative vascular injury. About 60% of these were minor and a result of avulsion of a branch of the left common iliac vein, which were subsequently repaired by a simple closure. The remaining 40% were major injuries, including injuries to the left iliac and femoral arteries requiring immediate thrombectomy and stent placement. 9 To mitigate this risk, approaches performed by vascular surgeons are strongly recommended.
Another study by Yuan et al. suggested similar complications but also included retrograde ejaculations, urological complications, and postoperative ileus, with postoperative ileus and retrograde ejaculations being most prevalent at rates of 2.2% and 1.9%, respectively. 10 , 11 When approaching L5-S1 anteriorly, damage to small nerves overlying the disc interspace compromise the sphincter valve that normally propels semen forward. Without the functionality of this valve, ejaculate travels retrograde into the bladder. Tiusanen et al. investigated retrograde ejaculation in nine patients who experienced this complication out of a cohort of 40 who received the procedure—7 of these 9 cases were ultimately permanent. 12 Some investigators have suggested that these complications are the result of the approach as well as surgeon-related factors; therefore, it has been recommended that patient should be positioned in a lateral decubitus position and that the cage be inserted in a transverse direction. Also, using Bovie electrocautery around the lumbar plexus should be avoided. 13
Sasso et al. reported an intraoperative urethral avulsion, which they believed to be secondary to the ureter getting caught in the double barrel sleeve and becoming avulsed during reaming, suggesting that threaded devices are associated with a higher complication rate than non-threaded devices. 14
Another complication associated with ALIF is subsidence. Beutler and Peppelman found an incidence of 10% for subsidence greater than 2 mm in their BAK (Bagby and Kuslich) cage interbody constructs. 15 They also found that subsidence was associated with an increased reaming depth and the use of larger cage sizes. A rare complication of cage fracture was reported by Klezl et al. 16 with the anterior approach, which they explained as potentially attributable to the patient’s body weight.
Retraction of the great vessels during this approach slows down vascular flow and may cause damage to vessel walls, leading to thrombotic events. In the literature, the incidence of DVT ranges from 0% to 5%. 11 , 17 - 20 Of note, however, is that the incidence of fatal pulmonary embolism is only 0.16% as reported by Faciszewski et al. 21
Posterior Approach
Posterior interbody fusion can be performed either as posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF), (Fig. 2). The posterior approach is indicated for spine fusion, intervertebral disc excision, nerve root exploration, and tumor resection. It is performed through a midline incision by way of palpation of the spinous processes, which are then exposed through superficial dissection through fat, lumbodorsal fascia, and paraspinal musculature. Deep dissection requires removal of the ligamentum flavum from its attachment to the edge of the lamina to expose the dura.

Transforaminal lumbar interbody fusion. Illustration by Rachel Hong-Kei Ho.
The posterior approach to interbody fusion was initially thought to be associated with more complications than the anterior approach. 22 , 23 Scaduto et al. 23 found that previous lumbar surgery was a risk factor for complications with the posterior approach. Glassman et al. 22 reported a case of a retropulsed cage after a posterior approach was adopted, and they recommended further investigation into the utility of posterior fusion cage insertion. Hacker 24 reported on a patient who had operative exploration because of a compressive radiculopathy that had developed after a PLIF with the use of a BAK cage. More recently, as TLIF has become more popular, those complications are becoming less common.
Dural tears were reported as an exclusive complication to the posterior approach by Yuan et al. 10 The hospital where the surgery was performed and number of segments of fusion were found to be predictors of the occurrence of dural tears in posterior spinal fusion. In fusions of four or more segments, the risk of dural tears was found to be increased threefold. 25
Cage migration was reported to be 8% in a study by Chen et al. with four of seven cage migrations cases receiving revision surgery. 26 Kim et al. reported an incidence of posterior migration and extrusion of expandable polyetheretherketone (PEEK) interfusion body device. 27 Postoperative cage migration may result in the loss of lumbar lordosis, narrowing of the disc space and foraminal region, and possibly direct compression of the dural sac and nerve roots. Another study by Zhao et al. 28 found that cage migration is closely correlated with the lack of posterior instrumentation and patients who underwent total facetectomy. Cho et al. showed that different cage designs do not affect the chance of cage migration if used with a pedicle screw construct. 29 A study 30 has proposed that medio-medial cage placement increased the rates of cage migration. Also, titanium open box cages seem to have a lower rate of cage migration. 30 Cage migration can be an issue especially when a small cage is used; however, large cages can be dangerous. Therefore, surgeons have a tendency to use small cages. In order to avoid this dilemma, expandable cages were recently introduced. The concern of using an expandable cage is that bone cannot be packed inside of the cage. Therefore, long-term outcome studies using expandable cages are needed.
Lumbar fusion with a posterior approach was also investigated with carbon cages. Brantigan et al. found that there were no major device-related complication while 13.5% of their patients experienced minor device-related complications such as broken cages and broken screws. 31
Laparoscopic Approach
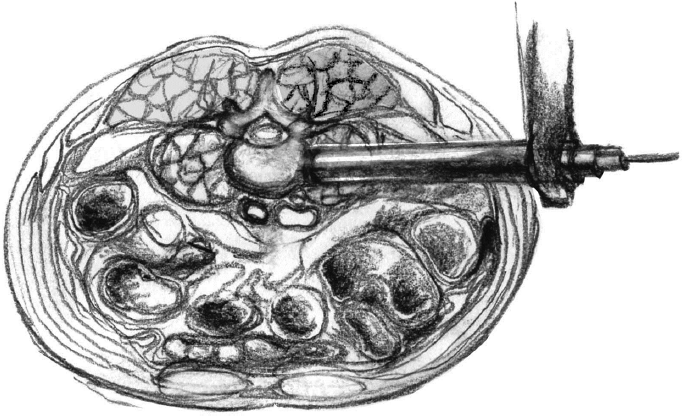
The laparoscopic approach has been investigated as it offers a smaller incision as well as a potentially shorter hospital stay compared to an open approach. The typical technique involves insufflation of the abdomen through a small incision at the umbilicus. With endoscopic visualization, the two lateral portals are introduced through lateral incisions to avoid the epigastric vessels in line with the L5-S1 disc space and slightly staggered from one another to expand the visual field. Retractors are then introduced through the portals, and the L5-S1 disc space can be exposed with gentle dissection of the retroperitoneum (Fig. 3).

Laparoscopic exposure of L4-5. Illustration by Rachel Hong-Kei Ho.
Sclafani and Kim 32 reviewed the learning curves associated with minimally invasive procedures for the spine and found that the most common complications for fusion procedures using a laparoscopic approach were implant malposition, neural injury, and nonunion, and that there was an overall postoperative complication rate of 11%. 32 Regan et al. 33 performed a retrospective review to compare the outcomes between a laparoscopic approach and an open approach and found that the complication rates were comparable between the two; however, the re-operation rate was higher in the laparoscopic group. 33 Probably due to the high complication rate, the laparoscopic approach is not currently utilized.
Axial Approach
Axial lumbar interbody fusion (AxiaLIF), initially reported as a minimally-invasive option for presacral lumbar fusion, is now considered an option for the treatment of degenerative disc disease, spinal stenosis, and low grade spondylolisthesis. It has even been suggested to be indicated for additional anterior correction after scoliosis correction, especially in patients with a lumbosacral fractional curve, large body habitus, or severe spinal stenosis requiring decompression. 34 It is performed via a small incision lateral to the coccyx, which is identified via palpation of the paracoccygeal notch. A blunt guide pin inserter is introduced superiorly and midline under fluoroscopy; the guide pin is then advanced into the sacrum at the S1-S2 level, and a transosseous channel is created with sequential dilators to allow access to the disc space of interest (Fig. 4).

Minimally invasive presacral retroperitoneal approach for lumbosacral axial instrumentation, AxiaLIF. Illustration by Rachel Hong-Kei Ho.
An early investigation into the safety of AxiaLIF using cadavers and three human pilot patients showed that surgeons performed the procedure successfully without vascular or neural injury. 35 Since then, further studies have reported fusion rates of 96% and 91% at short-term (one year) follow-up. 36 , 37 The most common complications reported in one study at one-year follow-up was superficial wound infection, followed by pseudarthrosis, rectal injury, hematoma, and nerve root irritation by hardware. 36 The risk of rectal perforation leading to pelvic hematoma has given some surgeons pause regarding the safety of performing this procedure on an outpatient basis. It is important to acknowledge that, although this procedure has largely shown satisfactory clinical results with short-term follow-up, the procedure is still relatively new, and therefore additional studies reporting long-term outcomes are required.
Lateral Approach
The direct lateral approach to lumbar interbody fusion (LLIF) is also suggested as a minimally invasive option for spine surgery; specifically it is thought to decrease pain and muscle injury by dissection through the psoas muscle rather than transecting it to allow direct access to the vertebrae and discs. The patient is prepared in the lateral decubitus position, and a transverse incision is made just above the pelvis. An access probe is inserted through the psoas muscle posterior to retracted abdominal contents, and a channel is created directly to bone through a guide wire and successive dilation. The camera, light source, and instruments are all introduced through the same channel (Fig. 5).
Lateral trans-psoas approach. Illustration by Rachel Hong-Kei Ho.
When compared to open approaches, this approach has been shown to be associated with a decreased need for pain medication postoperatively and decreased intraoperative blood loss. 38 , 39 It has been suggested to be as successful as more invasive approaches to the spine with regard to fixation, though surgeons are cautioned that the most common fusion levels of the lumbar spine—L4-L5 and L5-S1—are often difficult or impossible to access with this method. 40 Regarding complications, one series of 62 patients reported a 19% minor complication rate; the most frequent of which was hip flexion weakness that typically resolved after 6 weeks. 41 These investigators also reported one case of pseudarthrosis requiring revision surgery. Another study looked specifically at obese patients and found them to be no more likely to experience complications than non-obese patients: they reported a 7% complication rate with four of 156 patients requiring revision surgery. 42 In a small series of patients with degenerative disk disease and stenosis, all patients showed improvement in radiographic parameters, with 3 of 15 patients experiencing transient psoas weakness and 2 experiencing incomplete decompression requiring further surgeries. 43 More recently, complication rates were evaluated in a study of 43 patients at one-year follow- up. 44 These investigators reported transient postoperative anterior thigh pain in 25% of patients and postoperative hip flexor or quadriceps weakness in another 25%, which persisted 1 year after surgery in two patients. Lykissas et al. 45 showed that neurologic deficits that do occur after LLIF are transient and that the magnitude of correction of spinal deformity was correlated with a higher incidence of postoperative anterior thigh and groin pain, although this finding did not reach statistical significance. 45 Less common complications included nonunion in five cases and vertebral body fracture requiring kyphoplasty, infection, malpositioned cage, and retroperitoneal hemorrhage in one case each. Still, the investigators reported “significant improvement” in outcome scores at 1-year follow-up. Like all approaches, these complications must be weighed against the potential benefits of this option for minimally invasive spine surgery.
Minimally Invasive Approach
Minimally invasive techniques (MIS) for TLIF have been compared to open approaches with varying results. It is performed in a prone position. Once the incision is made, a tubular retractor system is introduced to the facet joint. Serial tubular dilators are then used to dissect muscle off the facet complex. Under a surgical microscope, inferior and superior articular facets are then resected using osteotomes. Once total facetectomy is completed, decompression and discectomy are performed, followed by interbody cage insertion. A percutaneous pedicle screw system may then be inserted through the same incision. 46
Seng et al. compared 40 cases of open TLIF to 40 cases of minimally invasive TLIF and followed patients for up to 2 years with regard to pain (measured by reports using the visual analogue scale) and fusion rates. 47 They found that MIS cases resulted in less blood loss during surgery, less use of narcotic pain medication, earlier ambulation, and shorter hospital stays. There was no difference between the groups with regard to pain, disability, or fusion rates. Parker et al. compared 100 patients (50 MIS and 50 open) in order to investigate the effectiveness and cost-utility of each proce- dure. 48 They confirmed decreased length of hospital stay and earlier return to work in the MIS group, resulting in lower mean hospital costs and indirect costs. Direct health care costs and quality-adjusted life years gained, however, were the same in both groups. Hackenberg et al. looked at 52 consecutive patients who underwent MIS TLIF with 3-year follow-up and found a fusion rate of 89%, which is comparable to a reported fusion rate of 90% and 100% for ALIF, proving it to be a viable and possibly favorable alternative to open approaches. 49
The most common complications to MIS TLIF include immediate postoperative radiculitis, persistent symptoms, and cerebrospinal fluid (CSF) leak. 50 Wong et al. 50 also noted significantly lower rates of respiratory and urinary infections, hematoma, and deep vein thrombosis, which were attributed to earlier mobilization, decreased pain leading to decreased narcotic use, and shorter length of stay.
Oblique Approach
The oblique lumbar interbody fusion (OLIF) was first coined by Silvestre et al. in 2012 and has since also been referred to as the “anterior to psoas” technique and LATERO approach. 51 - 53 This newest approach to the spine provides access between the anterior vessels and psoas muscles, avoiding the associated risks of ALIF and LLIF (i.e., injury to the iliac vessels and psoas muscle splitting). Using an anterolateral lumbar approach, the medial border of the psoas muscle is dissected posterolaterally while the retroperitoneal vessels are retracted in the contralateral direction. 54
From Silvestre et al.’s 51 study of 179 patients, which is the largest cohort to date, OLIF average operating time was 32.5 minutes, and average blood loss was 57 mL per level fused. The most common complication was incisional pain (2.2%) and sympathetic chain injury (1.7%). Injury to iliac or iliolumbar vessels occurred in 1.7% of patients. Of note, they reported that OLIF at L5-S1 level was only performed in six patients given the difficulty of retracting the iliac and lumbar veins. 51 There have since been myriad of follow-up studies and abstracts, most with small cohorts and limited follow-up. Oblique lumbar interbody fusion remains the newest frontier in lumbar interbody fusion but shows promise given its minimally invasive approach and its avoidance of the iliac vessels and psoas muscle splitting; however, further studies with large sample sizes and long-term follow-up are necessary to establish its safety and efficacy.
Summary
The techniques for interbody fusion have evolved and diversified over the last few years. With the advent of new and better technology and tools, spine surgeons have been able to explore and develop new approaches for achieving a biomechanically stable construct with minimal harm to the patient; however, each approach offers its own unique challenges and complications.
With the anterior approach, there is the risk of vascular injury and retrograde ejaculation, which can be mitigated by the collaboration of vascular surgeons as well as better patient positioning. There have also been reports of urethral avulsions with a threaded device as well as subsidence of greater than 2 mm with the use of larger cage sizes or increased reaming depth. Based on the Clavien-Dindo classification system, the complications of the anterior approach range from grade I to IV. 55
With the posterior approach, there is the risk of cage migration causing radiculopathy and loss of lordosis. The posterior approach also exclusively has the risk of dural tears. However, these risks decreased with the advent of the TLIF approach and may also decrease further with the use of expandable cages. Carbon cages may also play a role in decreasing complications using the posterior approach (Clavien-Dindo grades I to IV). 55
The laparoscopic approach at this time seems to have a steeper learning curve and more issues with complication rates when compared to open approaches (Clavien-Dindo grades I to IV). 55 More research will be needed.
The axial approach is complicated most commonly by superficial wound complications and pseudarthroses, though the risks of rectal perforation and pelvic hematoma are the most concerning and call into question the purported option of performing this procedure on an outpatient basis (Clavien-Dindo grades I to IV). 55
The lateral approach involves dissection through the psoas muscle and as such is most commonly complicated by transient psoas weakness, though is also associated with anterior thigh pain, pseudarthrosis, and incomplete decompression (Clavien-Dindo grades I to III). 55
MIS TLIF and OLIF remain the newest approaches to the spine. MIS TLIF has been shown to decrease operative blood loss and length of hospital stay with comparable fusion rates to open approaches. OLIF, the newest of all approaches, has also been shown to have less operative time and decreased blood loss; however, it is lacking in clinical studies and longterm follow-up. Complications with MIS approaches tend to be persistent symptoms given the limited visualization and exposure (Clavien-Dindo grade I). 55
None of the approaches discussed in this article have been proven to be invariably more dangerous or more effective for all patients. It should be underlined that minimally invasive techniques are newer to the field of spine surgery, and as such there is a paucity of long-term follow-up data confirming their safety and efficacy. Moreover, they can be more technically demanding and may not fall within the comfort level of all spine surgeons. Patients with comorbidities necessitating reductions in blood loss or anesthesia times, for example, may be better candidates for MIS. Patients with prior spine surgeries or complex anatomy may be better served by open procedures. As with any surgery, the decision for when to intervene and with which approach should involve a discussion between the surgeon and the patient.
Footnotes
Conflict of Interest Statement
None of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.