
Abstract
A 3-year-old female presented with a biopsy proven stage IIB proximal femur Ewing sarcoma. Following neoadjuvant chemotherapy, she underwent local control consisting of a wide proximal femur resection and subsequent reconstruction using a custom minimally invasive expandable prosthesis. Following revision to a larger device and serial expansions spanning a number of years the prosthesis slowly subluxated and eventually dislocated. A pelvic osteotomy was not successful in maintaining a concentric hip and a total hip arthroplasty was ultimately required. Dislocation is a known complication of expandable prosthesis. However, there is a paucity of literature describing the management and outcomes of patients who develop this complication. Close ongoing monitoring of hip joint congruency and limb length is recommended. If necessary, early intervention should be undertaken to maintain a reduce hip. Patient-specific management is essential when dealing with skeletally immature patients with more than 10 years of growth remaining.
Ewing sarcoma is a malignant tumor that arises from neuroectodermal tissue bone and soft tissue. The peak incidence of Ewing sarcoma is in the second decade. 1 The current treatment algorithm includes neoadjuvant chemotherapy to eradicate micrometastatic disease and facilitate effective local control measures, definitive local control with surgical resection or radiation, and adjuvant chemotherapy for systemic control. The 5-year survival rate with local disease is approximately 70% but with metastatic disease decreases to 15% to 30%. 1
Case Presentation
A 3-year-old female was transferred from an outside facility with a chief complaint of right hip pain after falling from a chair. The patient had no history of prior hip pain or functional difficulties. Radiographic imaging demonstrated a nondisplaced pathologic fracture through a lytic lesion within the subtrochanteric region of the proximal femur. The lesion appeared permeative and exhibited surrounding periosteal reaction (Fig. 1
Radiographic anteroposterior pelvis and lateral imaging of the hip demonstrating a lytic lesion with permeative borders, full thickness cortical defect, and surrounding periosteal reaction in the subtrochanteric region of the right proximal femur. The hip spica cast is present.
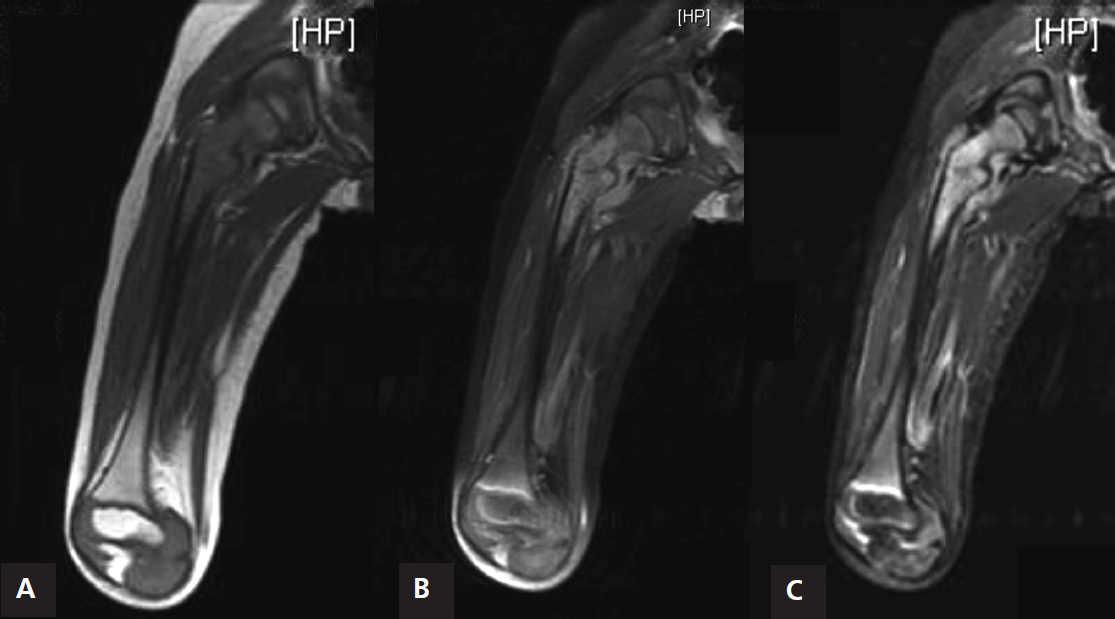
MRI coronal imaging of T1 (A), STIR (B), and post-contrast (C), demonstrating a marrow replacing lesion with heterogeneous uptake of contrast and surrounding soft tissue mass.
Surgical Management
Prior to surgical management, all possible alternatives and their benefits and drawbacks for local control, including amputation, radiation, and limb salvage, were discussed with her family. Their decision was to realize local control us-ing surgery, and a wide surgical resection and reconstruction was planned. A custom-made minimally-invasive growing prosthesis was fabricated based upon preoperative imaging prior to surgery. This consisted of a modular design that included both cemented and press-fit stem options as well as multiple head size options. Approximately 8.5 cm, as measured from the greater trochanter, of the proximal femur was resected in accordance with standard orthopaedic oncologic principles. Intraoperative marrow margins were negative. Histologic examination of the resection confirmed negative margins throughout. Thereafter, reconstruction was accomplished with the custom-made endoprosthesis using a press-fit fully-coated stem (Fig. 3). Excellent leg length and hip stability was realized (Fig. 4). The patient was subsequently a candidate for a percutaneous lengthening procedure based upon clinical and radiographic examination of the patient’s limb length discrepancy (Fig. 5).

The expandable customized implant. A, The press-fit stem and customized expandable endoprosthesis. B, Intra-operative photo of the press-fit stem in place. C, The customized expandable endoprosthesis fit over the press-fit stem implanted in the patient. To view this figure in color, see https://doi.org/10.12678/2470-3680.2.1.24.

Anteroposterior and lateral radiographic imaging of the initial resection and reconstruction. A custom-made endoprosthesis with lengthening capability was utilized.

Intra-operative imaging of lengthening and postoperative imaging of the lengthened prosthesis.
Once the maximum length of the prosthesis was obtained, a second custom-fabricated expandable proximal segment was placed. Due to stress shielding of the femur at the implant-bone junction, an allograft strut was used in an effort to augment stability of the construct and prevent peri-prosthetic fracture. Once again, the clinical and radiographic examination indicated that the patient was a candidate for a percutaneous lengthening procedure. The patient did well during the early postoperative period, but over time it became apparent that her femoral head was becoming increasing uncovered and, furthermore, that lengthening was worsening the position of her femoral head. On examination, she had a limb length discrepancy, positive Galleazzi test, and limited range of motion of the hip joint. Ultimately, she frankly dislocated her hip joint, and additional intervention was planned (Fig. 6).

Radiographic imaging of the prosthesis after a longer prosthesis was placed, and the bone-implant junction was grafted. The hip joint dislocated slowly as the prosthesis was lengthened.
She underwent exchange of her modular implant resulting in what was effectively a shortening of the proximal prosthesis, which permitted reduction of her hip. In an effort to improve femoral head coverage and stability, a pelvic shelf osteotomy was concurrently performed, after which she was protected in a hip spica cast for 6 weeks (Fig. 7). Thereafter, she underwent periodic lengthening as needed. Unfortunately, she exhibited ongoing instability clinically and radiographically and again dislocated despite prior efforts. The dislocation resulted in a persistent reliance on either crutches or a rolling walker; therefore, it was decided that she should undergo conversion to an unconstrained total hip arthroplasty with a new modular lengthening unit that could be exchanged (Fig. 8). The patient once again underwent serial percutaneous lengthenings as clinically indicated. Currently, at 8-months after conversion to a total hip arthroplasty, the construct is reduced and the patient is walking without the use of assistive devices. To manage her projected limb length discrepancy and limit the potential number of percutaneous lengthening procedures, she recently underwent contralateral epiphysiodeses of the proximal and distal femur.

Radiograph demonstrating the reduced hip joint after prosthesis shortening and shelf osteotomy.

Radiographs demonstrating the reduced total hip arthroplasty. A, Immediate postoperative imaging. B, Fluoroscopic imaging before, during, and after percutaneous lengthening demonstrating maintenance of the reduced total hip arthroplasty.
Discussion
This case illustrates a challenging reconstructive dilemma for the orthopaedic oncologist. The patient was 3 years old at the time of presentation, with potentially over 10 years of growth remaining. The goals of the orthopaedic oncologist include first and foremost, complete extirpation of the tumor followed by limb-salvage reconstructive surgery. Additional charges include obtaining acceptable functional and aesthetic outcomes and minimizing the burden of further surgery in as much as possible. In considering these aims, local control options, including both surgical and radiation, need to be carefully weighed. It was recognized that there was no perfect solution for this patient. Limited bone stock with such a large potential for remaining growth were recognized hurdles.
Radiation
Radiation can potentially provide durable local control in patients with Ewing sarcoma and is well-described. 2 Radiation can also be used if negative margins are not obtained during surgical resection or if there is a poor response to chemo- therapy. 3 However, radiation is not without its complications. Secondary sarcoma remains the most concerning long-term complication 4 , 5 and serves as the primary rationale favoring surgery in cases where adequate margins and reasonable surgical outcomes can be expected. Short-term radiation-associated complications of the bone include osteopenia, growth arrest, and fracture. 6 Both early and late soft-tissue toxicities are also well-recognized.
Amputation
Radiation and chemotherapy has allowed limb-salvage to be the primary surgical option for local control in Ewing sarcoma. Although amputations are theoretically within the surgical armamentarium, unresectable tumors are usually addressed with radiation with the understanding of the inherent risks previously discussed. Unlike osteosarcoma, which requires complete resection of all bulk disease in order to effect cure, the radiation-sensitive nature of Ewing sarcoma usually precludes the need for amputation. In theory, amputation benefits include early mobility and weightbearing. The more proximal amputations require higher energy and metabolic demands for ambulation. 7 Complications include phantom pain, bleeding, infection, bone overgrowth, soft tissue stump migration, and muscle imbalance. Bone overgrowth is more common in patients who are less than 10 years of age and may lead to skin perforation, pressure ulcers, and poor prosthesis fit. Disarticulation and osteomyoplasty can be utilized to minimize the risk of overgrowth. 8
Rotationplasty
Initially described as a procedure for severe limb deformity secondary to tuberculosis, Van Nes utilized rotationplasty for proximal focal femoral deficiency. 9 In the 1970s, it was applied to oncologic cases as an alternative to above-knee amputation. Its benefits include recreating the knee joint by utilizing the ankle joint and biologic fixation, which creates a durable construct. By utilizing the projected limb length discrepancy, the surgical limb can be left longer with the expectation that the contralateral limb will eventually match its length. Multiple long-term studies demonstrate that it offers a durable reconstruction. 10 , 11 Quality of life and emotional difficulties associated with the reconstruction are more evident in adolescence and are usually overcome by adulthood. 11 Complications associated with rotationplasty are most commonly associated with occlusion of the vessel anastomosis. Less common complications include deficient wound healing, transient nerve palsies, irreversible nerve palsies, pseudoarthrosis, and rotational malalignment. 10
Limb Lengthening
Another alternative to restore lower extremity length is to resect the segment of diseased bone and then use distraction osteogenesis to replace it. This can be done using two methodologies: external fixation or with an intramedullary device. The description of the original technique involved circular or monolateral external fixators that were used to lengthen the bone 1 mm per day. 12 This allowed for an accurate lengthening; however, the external fixators are extra-corporal devices that are prone to pin site infection, hardware breakage, scarring, joint stiffness, and muscle contractions. 13 , 14 Recently, the FDA approved an intramedullary device that utilizes a rare metal magnetic motor to allow for precise lengthening. The PRECICE® nail (Ellipse Technologies, Inc., Irvine, CA, USA) uses an external controller that contains two revolving magnets to allow for adjustable distraction rates. 15 A retrospective review of 25 patients undergoing femoral and tibial lengthenings demonstrated accurate and precise lengthening along the anatomic axis. There was one implant complication of a non-functional motor that was treated with exchange nailing. There was one femoral complication due to early consolidation secondary to not following the specified distraction schedule. Delayed union, equinus contracture, and toe clawing occurred in patients undergoing tibial lengthen- ing. 16 Additionally, it is recommended that upon bony union, the nail should be removed to prevent future complications associated with the magnet. 15
Limb-Salvage Surgery
Alternatives for reconstruction include osteoarticular allograft, vascularized fibular allograft, combined osteoarticu- lar allograft and vascularized fibular graft, and arthroplasty. Allograft reconstruction has a limited ability to remodel and revitalize outside the host bone and allograft interface. 17 Additionally, there is a difficulty attaining an appropriately sized bulk allograft in the pediatric population that becomes more difficult with younger patients. The most common short-term complications are infection, nonunion, and frac- ture. 18 Long-term, articular allografts develop joint arthroses and lack capacity for longitudinal growth. Vascularized fibular allografts introduce viable bone and reduce the rate of infection and nonunion. 19 , 20 They have demonstrated the ability to hypertrophy. However, the risk of fracture is still present. 21 Initially described for the upper extremities, there have been case reports and small case series describing the use of vascularized fibular epiphyseal transplants to reconstruct the proximal femur. 22 , 23 The epiphyisis of the proximal fibula remodels to create a stable hip joint to allow for range of motion. The diaphysis hypertrophies to allow for weightbearing. The viable physis allows for longitudinal growth. 24 The surgery is technically difficult, creates donor site morbidity, and there is risk of fibula fracture. 25 To augment the mechanical properties, structural allograft can be combined with vascularized fibular allograft. 26 , 27 This is usually performed for intercalary reconstruction, but case series describe its use with articular allografts. In one study 21 of 18 pediatric patients who underwent vascularized fibular graft with and without allograft, 15 required more than one revision or secondary procedure. Of note, one patient was 18 months old at the time of the diagnosis of Ewing sarcoma of the proximal femur. He underwent resection and reconstruction with vascularized fibular graft. Within the 12-month follow-up period, he developed a nonunion and required two additional procedures. 21
Pediatric arthroplasty is an uncommon and complicated procedure. In the USA, estimates range from 10,000 to 30,000 pediatric arthroplasties being performed over the last 5 years. 28 Arthroplasty in this population is complicated by limited bone stock and smaller implant size. Pediatric total hip arthroplasty has an average revision rate of 5.4%, approximately five times greater than the published average for adults. For younger patients, the revision rates can be as high as 33% over 13 years. 29 The most common causes are aseptic loosening and polyethylene wear. 29 , 30 Of note, the case series presented by Bessette et al. and Clohisy et al. only included adolescents and teenagers. Extrapolating the results of the above studies to patients with potentially 10 years of growth remaining implies an even greater risk of revision.
Complications associated with limb salvage surgery with expandable endoprosthesis include infection, nerve damage, dislocation, peri-prosthetic fractures, contractures, and mechanical failure. Infection is the most prevalent complication. One series of 40 patients that underwent reconstruction with expandable prosthesis describes 3 patients that required revision surgery to permit additional lengthening. 31 Another series of 38 patients of a similar population described 6 dislocations, 1 of which was treated with closed reduction and the others were treated with open reduction and acetabular osteotomies. At last follow-up, all patients had a stable hip joint. 32 The average age of the cohorts in the studies was 10.4 and 10.5 years. It was concluded that the younger the patient, the shorter the time to failure.
Limb Length Discrepancy
Almost 90% of patients with bone sarcomas of the extremities are candidates for limb-salvage surgery. 33 Limb-salvage surgery can be demanding, requiring careful preoperative planning, particularly for skeletally immature patients. Among other considerations, careful attention must be paid to the potential limb length discrepancy expected following physeal resection and radiation. There are multiple methods for calculating the potential leg length inequalities. The arithmetic method is based on an assumed age of growth completion and annual physeal growth. The Eastwood-Cole method is based on graphic arithmetic determined by CT scans. The Green-Anderson growth remaining method is based on chronologic age and growth percentile. The Paley multiplier method is based on chronological and bone age. The Moseley straight-line graph method corrects for skeletal age. No method is without its limitations, and the potential accuracy is improved by having longitudinal data. 34 , 35 None of the methods have been validated for radiated bone.
Limb length inequality can be managed using a number of techniques, depending in part on the quantitative extent of the inequality. For symptomatic patients with discrepancies up to 2 cm, a shoe lift can be used. Differences between 2 cm and 5 cm require a shoe lift, acute shortening, or a contralateral epiphysiodesis, assuming adequate potential growth remains. Differences from 5 cm to 15 cm require a lengthening procedure on the ipsilateral extremity either over an intramedullary nail or utilizing a multi-planar circular frame. Finally, management of differences greater than 15 cm includes both lengthening procedure on the shortened extremity as well as shortening of the contralateral limb. In extreme cases, amputation of the shorter limb has also been described to allow for ambulation with a prosthesis. 35 In general, growth modulation’s impact is greater in younger patients; however, timing is often dictated by oncologic treatment and time of presentation.
There is no clear threshold above which symptoms always develop. It is clear that the greater the inequality, the more likely the patient will experience functional and symptomatic effects. The shorter limb can develop tibiotalar equinus, muscular atrophy, and pelvic tilt. There is anecdotal evidence of lower back pain also being more common in people with limb-length inequality. As limb length discrepancy increases, perceived exertion, oxygen consumption, and quadriceps fatigue increases. 36
Conclusion
In summary, we present a case of a 3-year-old female with stage IIB proximal femur Ewing sarcoma treated with an expandable endoprosthesis that was ultimately revised to a total hip arthroplasty for recurrent dislocation. There is a paucity of literature describing the management of tumor resection and reconstruction in skeletally immature patients with potentially 10 years of growth remaining. In our experience, it is recommended to preoperatively balance the risks of local control with the perceived benefits carefully explaining all relevant issues with the family. Intra-operatively, careful capsular reconstruction or augmentation needs to be performed. In the developing hip, reliance on the implantbone joint congruity is not sufficient. Postoperatively, hip subluxation and congruency monitoring during and after the lengthening procedures needs to be performed. Surgeons should consider early utilization of a pelvic osteotomy or arthroplasty if subluxation occurs. These cases are rare and challenging, and management requires careful planning and consideration of patient-specific needs and expectations.
Footnotes
Conflict of Interest Statement
None of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.
Acknowledgments
We would like to thank Jeremy Berger, P.A.-C., Samantha Armstrong, N.P., and Christine Moloney, P.A.-C., for their contributions in the clinical care of this patient and in providing some of the details and information relevant to the patient’s clinical course.