
Abstract
Background
Virtual reality in rehabilitative therapy has long been studied as a new modality of treatment for patients with disabilities. However, despite years of research, formal guidelines on the effective use of rehabilitative virtual reality therapy have not yet been established. This suggests that existing literature does not yet provide sufficient evidence from which to draw generalized conclusions regarding the efficacy of virtual reality therapy.
Objective
To analyze the methodology of recent studies on the use of virtual reality in patients with strokes, spinal cord injuries, amputations, and brain injuries.
Method
A search was conducted for manuscripts using the terms “virtual reality” in combination with “stroke,” “spinal cord injury,” “amputation,” or “brain injury.” Preliminary results were then screened for randomized control trials that compared the use of virtual reality therapy either as an alternative or adjunct to non-virtual reality intervention. We excluded papers that did not provide full text access to ensure thorough methodological review. Studies were then characterized according to the following themes: rehabilitation diagnoses, virtual reality technology, chronicity, outcome measures, and study design.
Results
38 studies were included in our review following the final screen. After characterizing each paper according to the aforementioned themes, we found significant heterogeneity amongst the methodology studies used to investigate the effects of VR therapy. Furthermore, few studies followed their patients for a prolonged period. We also found that most studies were in patients with strokes, with far fewer studies including patients with spinal cord injuries, brain injuries, or amputations.
Conclusions
The substantial heterogeneity we found among virtual reality studies likely contributes to the lack of guidelines regarding the use of virtual reality in rehabilitation. While prior studies have shown significant promise regarding the efficacy of virtual reality therapy, future studies must implement more uniform methodology in order to draw more generalizable conclusions.
Introduction
Patients who suffer from strokes, spinal cord injuries, amputations, and brain injuries frequently sustain substantial functional deficits and mobility alterations that significantly impact their quality of life. Facilitating recovery from these impairments can often determine whether a patient continues to live at home or needs to be sent to a long-term care facility.
Physical, occupational, and speech therapy have traditionally been the cornerstones of rehabilitation treatment, with an emphasis on prioritizing early mobilization to maximize functional recovery. Therapists often employ multiple interventions to facilitate or enhance outcomes, such as TENS, shock wave therapy, bodyweight supported gait trainers, and robotic aids. Virtual Reality (VR) technology has recently emerged as a promising new frontier in the field of rehabilitation. However, despite numerous studies, the effectiveness of VR therapy and standardized practice guidelines regarding its use have yet to be clearly established.
The purpose of this scoping review is to describe the current literature surrounding VR in rehabilitation and to identify possible targets for future research. Specifically, we sought to assess and characterize trends in recent studies across the following domains: type of VR technology utilized, nature of intervention compared with control groups, rehabilitation software, patient populations and diagnoses targeted, outcome measures, and duration of treatment.
Methods
Eligibility Criteria
This review specifically sought randomized controlled trials (RCTs) that directly compared the use of VR therapy either as an adjunct or standalone treatment to a control group treated with non-VR therapy in patients with strokes, spinal cord injuries, amputations, or brain injuries. To capture the breadth of the current literature, we chose to define VR as any form of technology used to create a virtual environment with which a patient could interact, (eg, immersive headsets, traditional gaming consoles, computers, virtual treadmills).
We chose to limit our review to RCTs to assess the methodologies and rigor of those studies that provide the bulk of the evidence supporting the use of VR in rehabilitation, and to identify potential gaps for future research. We also limited our review to studies that were published within the last 5 years (2020-2025). Narrowing our search to this time frame enabled our assessment of the literature to remain current, which, given how quickly technology has been shown to evolve in the modern day, was a high priority for our review.
We excluded any studies for which we did not have full text access to avoid mischaracterization. We also did not include studies that utilized VR therapy to treat patients with chronic neurodegenerative disorders, such as Alzheimer’s or Parkinson’s disease.
Information Sources and Search
Studies were identified using an advanced electronic search of the PubMed database. The initial search was conducted by the primary author using the terms “virtual reality” in combination with “stroke,” “spinal cord injury,” “amputation,” or “brain injury.” Details of the search strategy are provided in Supplemental Figure 1. This search produced 2244 results.
Selection of Sources of Evidence
When our query was limited to publications from 2020 to 2025, the total number to results was narrowed to 1122. After search results were further restricted to publications designated as randomized control trials, 94 total publications were identified.
These 94 publications were then uploaded directly to Covidence for further screening. Initial abstract and title screening performed by the primary author excluded 34 studies. Of the 34 excluded studies, 6 studies were excluded due to having an inappropriate study design, 11 were excluded for investigating ineligible patient populations, 6 were excluded for testing unrelated interventions, and 11 were excluded for having intervention and/or control group designs that did not match our inclusion criteria.
The remaining 60 studies underwent full text screening by the primary and secondary authors. Any papers that were not available for full text access were excluded as there was no way to assess methodology. This resulted in 22 studies being excluded. The remaining 38 studies underwent final data extraction and analysis. There were no disagreements in the screening process between authors. The outline of this process is summarized in Supplemental Figure 2.
Data Charting and Items
Summary of Studies Assessing the Efficacy of Virtual Reality Rehabilitation in Stroke Patients
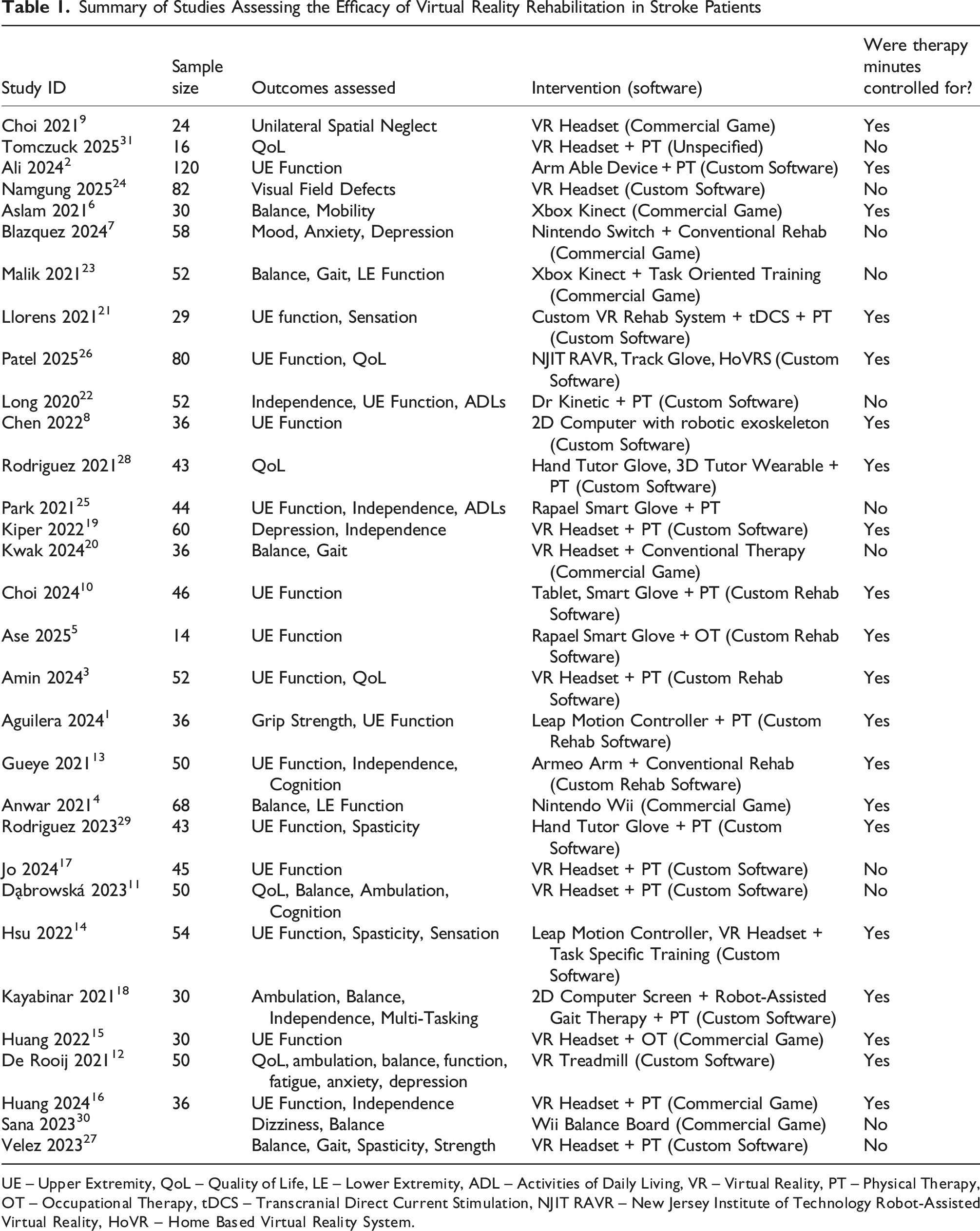
UE – Upper Extremity, QoL – Quality of Life, LE – Lower Extremity, ADL – Activities of Daily Living, VR – Virtual Reality, PT – Physical Therapy, OT – Occupational Therapy, tDCS – Transcranial Direct Current Stimulation, NJIT RAVR – New Jersey Institute of Technology Robot-Assisted Virtual Reality, HoVR – Home Based Virtual Reality System.
Summary of Studies Assessing the Efficacy of Virtual Reality Rehabilitation in Spinal Cord Injury Patients

LE – Lower Extremity, VR – Virtual Reality, PT – Physical Therapy.
Summary of Studies Assessing the Efficacy of Virtual Reality Rehabilitation in Brain Injury Patients

UE – Upper Extremity, VR – Virtual Reality, OT – Occupational Therapy.
Results
Rehabilitation Diagnoses
The majority of the included VR treatment studies involved patients with strokes, with 31 out of 38 studies (81%) focused on stroke patients.1-31 Four studies (11%) involved SCI patients, and 3 (8%) involved brain injury patients.32-38 No studies testing the use of VR therapy in patients with amputations met our inclusion criteria. Four studies involving patients with amputations were included in the early stages of our search. Three of these were excluded due to our inability to access the full text, and one was excluded because it included patients with a range of “lower limb trauma,” including fracture and soft tissue injury.43-46
VR Technology (Hardware and Software)
Given the breadth of available VR technology, we wanted to characterize the nature of the VR hardware and software being used to treat patients with rehabilitation needs. Out of 38 studies, 14 (37%) utilized fully immersive VR (FIVR).3,9,11,14-17,19,20,24,27,31,35,36 We defined FIVR as fully enclosing the test subject within the virtual environment using a head mounted display. Studies using FIVR most commonly utilized commercially available head mounted displays such as the Oculus Rift, or HTC Vive. Six studies (16%) used commercially available game systems including the Nintendo Wii, Nintendo Switch, and Xbox Kinect.4,6,7,23,30,37 The remaining 18 studies (47%) used a wide range of specialized virtual reality rehabilitation systems, all of which were non-immersive. These included systems such as GRAIL VR treadmills, the RAPAEL smart glove, ARMABLE, Dr Kinetic, Hand Tutor, the Kymeia HomeKit, and the Armeo Robotic Arm.1,2,5,8,10,12,13,18,21,22,25,26,28,29,32-34,38
Our analysis of the software utilized in these studies divided results into two categories: commercial and custom. Commercial was defined as VR games intended for use by the general public, while custom programs were those designed specifically for the purpose of rehabilitation. Ten of 38 studies (26%) utilized commercial video games as part of their VR treatment,4,6,7,9,15,16,20,23,30,37 27 (71%) utilized custom rehab software, and 1 (2%) did not specify the nature of their VR software.1-3,5,7-19,21,22,24-29,31-36,38
Chronicity
There was substantial variability in time from condition onset to analysis between the included works. Of the 31 studies that included patients with strokes, 4 (12.9%) limited their inclusion criteria to patients within 30 days of diagnosis,13,16,25,26 1 (3.2%) limited its inclusion criteria to patients between 1 and 3 months of diagnosis, 8 10 studies (32.2%) were limited to patients within 6 months of diagnosis,2,9,11,12,17,23,27-30 11 studies (35.5%) included patients more than 6 months after diagnosis1,5,6,10,14,15,18,20-22,24; and 5 (16.1%) did not specify a time from symptom onset as part of their inclusion criteria.3,4,7,19,31 Among studies targeting patients with SCI, 3 of 4 (75%) only included patients more than 6 months from their injury date while 1 (25%) did not specify a time from diagnosis as part of its inclusion criteria.35-38 Of the 3 studies involving patients with brain injuries: 1 included patients at least 3 months after their brain injury, 1 limited itself to patients more than 6 months after brain injury, and 1 included only those patients who were more than a year out from their brain injury.32-34
Outcomes
Studies used a broad range of primary and secondary outcomes to evaluate the effectiveness of VR therapy. Seventeen of 38 studies (44.7%) assessed upper extremity function before and after treatment using outcome measures such as the Fugl Meyer Assessment for Upper Extremities, Box and Block Test, Action Research Arm Test, or the Jebsen Taylor Hand Function Test.1-3,5,8,10,13-17,21,22,25,26,29,33 Conversely, lower extremity function, balance and ambulation were assessed in 13 of 38 (34.2%) studies using outcome measures such as the Fugl Myer Assessment for Lower Extremities, Berg Balance Scale, Timed up and Go Test, or the Rivermead Mobility Index.4,6,11,12,18,20,23,27,30,32,35,37,38 Functional independence and quality of life outcomes were examined in 16 of 38 (42.1%) studies using tools such as the Bartels index, EuroQoL 5 dimensions, Canadian Occupational Performance Measures, or modified Rankin score.2,3,11-13,16,18,19,22,25,26,28,31-33,38 Seven of 38 studies (18.4%) investigated the impact of VR therapy on mood and cognition, drawing on standardized assessments such as the Hospital Anxiety and Depression Scale, Montreal Cognitive Assessment, Frontal Assessment Battery, or Mini Mental State Exam.7,11-13,19,32,34 Pain and sensation were only investigated as outcome measures in 2 (5.2%) and 3 (7.9%) studies, respectively.14,19,21,31,36 Unique outcomes studied included visual field deficits, unilateral spatial neglect, caregiver distress, and dizziness, each of which were assessed in separate individual studies.9,24,30,32
Study Design
Eleven of 38 studies (29%) compared VR therapy as a standalone treatment to non-VR therapy, while 27 of 38 studies (71%) studied VR therapy as an adjunct to non-VR treatment. Eleven of 38 studies (29%) did not control for the amount of total therapy time received by the intervention and control groups.7,11,17,20,22-25,27,30,31 Study duration, including treatment and follow up, varied significantly between studies, ranging from 2 to 24 weeks, with the average amongst all studies being 8.9 weeks. Only 16 studies (42%) continued following their test subjects after completing treatment.1-5,11,12,14-16,26,28,29,33,36,38 Sample size also varied substantially, ranging from 16 subjects to 120, with the average amongst all studies being 44 subjects.
Discussion
VR therapy has long been seen as an exciting new frontier in the field of rehabilitation medicine. However, despite widespread interest, formal clinical guidelines and best practices regarding the implementation of rehabilitative VR therapy have yet to be established. This indicates that the state of the literature in its current form does not yet provide sufficient evidence to establish such guidelines. The results of our review suggest that this may be due to several reasons.
Firstly, VR therapy studies often appear to be limited by small sample sizes. Of all the studies in our review, the largest study, conducted by Ali et al, included only 120 subjects. The average sample size was even smaller, at only 44 subjects. These smaller sample sizes can limit the generalizability of their findings and have been cited as a key limitation in prior meta-analyses that have previously attempted to consolidate existing VR rehabilitation research.47-50 Further analysis into the methodology of the studies within our review provides insight into why smaller sample sizes seem to be a persistent problem. Larger studies—such as those conducted by Ali et al, Patel et al, Choi et al, and Anwar et al—bolstered their sample sizes by recruiting from multiple centers, inpatient rehabilitation units, or extending the duration of enrollment.2,4,26,33 While Anwar et al recruited their patients over the course of 15 months, smaller studies such as Nicolelis et al, only recruited patients over the course of 4 months. Similarly, Ase et al, Nair et al, and Choi et al, some the smallest studies in our review, relied on singular rehabilitation centers or outpatient practices for recruitment, which likely contributed to their inability to perform larger studies.5,9,37
We also found that the range of time since onset of diagnoses of subjects within these studies was often broad. While some studies focused on the acute phase of recovery, many had no upper limit for time since diagnosis as part of their inclusion criteria. Zwijgers et al, for example, included patients whose time since onset of illness ranged from 2 years all the way to 11 years. Similarly, Kayabinar et al’s and Ase et al’s cohorts showed significant variability, with time since onset of illness ranging from just a few months to several years. Our review also demonstrated a lack of consistency regarding the definition of subacute vs chronic phase of illness. Studies conducted by Hsu et al and Llorens et al defined chronic phase as greater than 6 months since onset of illness, whereas Huang et al defined it as onset greater than 3 months. The definition of the subacute phase of illness appeared to be even more variable. Chen et al defined it as onset of illness between 1 to 3 months, while Patel et al defined it as less than 30 days, and Sana at al and Rodriguez-Hernandez et al defined it as up to 6 months. Multiple studies, such as those written by Nair et al and Tomczuck et al, did not specify chronicity as part of their inclusion criteria at all. Prior literature has shown that the functional recovery curve of illnesses such as stroke, spinal cord injuries, and brain injuries can evolve over time.39-42 However, it has yet to be established at what phase of recovery VR therapy is most appropriate to implement, likely because of the lack of focus on specific phases of recovery or standardized definitions of these phases amongst currently available VR therapy trials. Kenea et al and Leong et al both reference this as a limitation of their subgroup analyses within their own meta-analyses.51,52
In addition, studies in our review were often limited in the duration of their follow-up, with an average observation period of only 8.9 weeks. Studies conducted by Tomczuck et al and Chen et al, only followed their subjects for 2 weeks. We also found substantial variability in whether studies chose to continue monitoring subjects after completing treatment. Some studies, like Rodriguez-Hernandez et al and Patel et al, followed their patients for months after completing treatment. These studies, however, were in the minority. Most other studies only followed their patients for weeks after completing treatment, or not at all. Without sustained monitoring, it is difficult for larger systematic reviews and meta-analyses to establish how durable the effects of VR therapy are, further limiting the conclusions that can be drawn from the available literature. Soleimani et al references this as a limitation in their meta-analysis on the effects of VR therapy on upper extremity function in patients with strokes. 50
Another significant limitation of the current literature appears to be that, while VR therapy has been tested numerous times, there remains a high level of heterogeneity amongst the methodology that these studies often use. While most studies in our review utilized immersive VR headsets to deliver their VR therapy, many studies chose alternative technologies, ranging from traditional gaming consoles and computers to high tech 3D treadmills and robotic arms. Additionally, the forms of VR therapy were often variable, with some studies utilizing rehabilitation specific software, while others utilized commercial games. As a result, it remains unclear whether the results of Kiper et al, which utilized fully immersive VR headsets with customized rehabilitation software, should be considered comparable to studies like Anwar et al, which utilized the Nintendo Wii and commercial games. Even amongst the studies that utilized rehabilitation specific software, each study had its own unique VR therapy program, making uniformity difficult to establish. For example, both Amin et al and Hsu et al utilized fully immersive VR headsets and customized rehabilitation software to improve subjects’ upper extremity function. However, one implemented VR based mirror therapy software, while the other employed VR carnival style games. We also found that VR therapy was frequently tested both in isolation and in combination with conventional therapy and that total therapy time was not consistently controlled between treatment arms. Outcome measures and the clinical assessment tools used to evaluate them also varied substantially between studies, even amongst those treating similar conditions and deficits. For example, while Gueye et al used the Fugl Meyer Assessment to track improvement in upper extremity function in stroke patients, Aguilera-Rubio et al utilized the Box and Block test, the Disabilities of the Arm, Shoulder and Hand questionnaire, and the Action Arm Test. This widespread methodological variability makes it difficult to pool results across studies and formulate broadly applicable clinical recommendations. As a result, studies in VR therapy suffer from procedural heterogeneity that has often been cited as a limiting factor in prior meta-analyses of VR therapy.53-55
There also appears to be an under-representation of patients with spinal cord injuries, brain injuries, and amputations compared to those with strokes within the current literature. We found numerous studies examining the application of VR therapy in stroke patients that matched our inclusion criteria, targeting a wide range of deficits, including upper and lower extremity function, balance, ADL participation, and cognition. However, our search for studies on VR therapy in patients with spinal cord injury and brain injury generated far fewer results. Our initial search for studies pertaining to patients with amputation similarly produced few results, all of which were ultimately excluded due to not meeting our inclusion criteria. Spinal cord injuries, brain injuries, and amputations often lead to marked functional impairment, equivalent to that of a stroke. The relative lack of studies in patients afflicted with these conditions in turn has led to a paucity of the evidence needed to guide the implementation of VR therapy into their recovery. De Miguel-Rubio et al similarly note the low number of available studies as a limitation in their own meta-analyses on the use of VR therapy in patients with spinal cord injury. 48
Future research should attempt to address the above barriers by modifying research protocols to improve upon prior methodology. Increasing sample sizes and standardizing intervention methods would decrease heterogeneity while increasing generalizability of results. Specific targets for standardization could include the type of VR hardware utilized, type of VR therapy software, duration of follow-up and chronicity of illness. By reducing variability amongst future research protocols, the available pool of evidence regarding the effective use of VR therapy will expand and lay the foundation for future guidelines.
Limitations
We encountered a few limitations in the process of writing this scoping review.
The first was our use of PubMed’s database as our sole source of evidence, as we were unable to access databases such as EMBASE or CINAHL. While our search strategy acquired enough articles for us to feel confident in writing this review, it is possible that by not using alternative databases, we missed some relevant results. Future reviews should consider utilizing additional research databases to broaden results.
Another limitation was our lack of studies that tested the effects of VR therapy in patients with amputations. The few relevant studies that we did obtain in the early stages of our search were ultimately excluded for not matching our inclusion criteria. Future studies can address this limitation, either by using alternative databases as mentioned above, or by adjusting inclusion criteria to capture these studies.
Finally, our review did not include other rehabilitation diagnoses such as joint replacements, long bone fractures, or multiple sclerosis. While VR therapy has been explored in these and other conditions, our focus was limited to a narrower set of neurologic and structural impairments. Future research would benefit from incorporating a broader range of rehabilitation diagnoses to better understand the full scope of VR therapy’s potential applications across diverse patient populations.56-58
Conclusion
The future of VR rehabilitation continues to show significant promise. As VR technology advances and becomes more affordable, accessibility will continue to increase. This trend represents an opportunity for clinicians to broaden the use of VR therapy for rehabilitative purposes. But in order for VR therapy to be used effectively, clinical guidelines must be established. In the past, the generalizability of existing studies has been limited by small sample sizes and heterogeneity in both patient populations and methodologies, making guidelines difficult to establish. Addressing these limitations through more rigorous and standardized studies will be essential to the future of VR therapy. As research continues and the evidence base strengthens, the use of VR in rehabilitation is likely to expand, accompanied by the development of evidence-based guidelines to support its application in diverse clinical settings.
Supplemental Material
Supplemental Material - The State of Virtual Reality in Stroke, Spinal Cord Injury, Amputation, and Brain Injury Rehabilitation: A Scoping Review
Supplemental Material for The State of Virtual Reality in Stroke, Spinal Cord Injury, Amputation, and Brain Injury Rehabilitation: A Scoping Review by Rohan Gogoi, Anna Vargo, Moorice Caparo, Mitchell Fourman, Andrew Gitkind, Mohammed Yasin in Montefiore Einstein Journal of Musculoskeletal Medicine and Surgery
Supplemental Material
Supplemental Material - The State of Virtual Reality in Stroke, Spinal Cord Injury, Amputation, and Brain Injury Rehabilitation: A Scoping Review
Supplemental Material for The State of Virtual Reality in Stroke, Spinal Cord Injury, Amputation, and Brain Injury Rehabilitation: A Scoping Review by Rohan Gogoi, Anna Vargo, Moorice Caparo, Mitchell Fourman, Andrew Gitkind, Mohammed Yasin in Montefiore Einstein Journal of Musculoskeletal Medicine and Surgery
Footnotes
Ethical Considerations
There are no human participants in this article and informed consent is not required.
Consent to Participate
There are no human participants in this article and informed consent is not required.
Author Contributions
1. Rohan Gogoi, MD: Authorship, data collection, and data extraction
2. Anna Vargo, MS4: Authorship and data extraction
3. Moorice Caparo, MD: Editing and supervision
4. Mitchell Fourman, MD: Editing and supervision
5. Andrew Gitkind, MD: Editing and supervision
6. Mohammed Yasin, DO: Editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.