
Abstract
Background: In an effort to satisfy the American Board of Orthopaedic Surgery (ABOS) requirement for a month-long orthopaedic skills rotation, programs often construct a skills curriculum that is procedurally based. As an alternative, we describe a skills program that teaches individual tool skills to fluency (accuracy at speed) using instructional modules that are innovative, challenging, inexpensive, and when combined with an operant learning program, encourage deliberate practice.
Methods: The orthopaedic faculty identified 14 surgical tools that postgraduate year one (PGY-1) orthopaedic residents should use fluently before encountering them in the operating room. A curriculum was designed to teach the foundation and component behaviors necessary to achieve fluency. The curriculum was composed of 16 modules and 72 sub-modules and was presented to the 2014 and 2015 PGY-1 orthopaedic residents during a 1-month dedicated rotation (July 2014 and July 2015). Upon completion of the first rotation, the six members of the 2014 PGY-1 class were asked to complete timed tasks to evaluate their skills. Both the 2014 and 2015 classes were asked to fill out a detailed survey evaluating the tool modules and the module instructors. The costs of the modules were recorded.
Results: All six members of the 2014 PGY-1 class completed all of their timed tasks. One resident did not successfully perform one of four knot tying tasks and another resident did not successfully perform a drill task. Twelve residents, (all six members of both the 2014 and 2015 PGY-1 classes) completed the survey. All of the 2015 class (6/6) considered themselves comfortable with at least half of the tools, and five of the six members of the 2015 class were comfortable with all of the tools. The survey also indicated that teachers successfully communicated the goals of the modules, gave clear instructions and contributed to the module’s success. The total cost for the skills month, for six residents, was $11,730 ($122/resident/module).
Conclusions: A curriculum was designed to teach PGY-1 orthopaedic residents the foundation skills necessary to use 14 orthopaedic tools fluently. The objective of teaching the foundation and complex behaviors required to use the 14 selected tools was achieved. That goal was accomplished using a precisely defined curriculum in a supportive environment that enabled deliberate practice. It was done in a way that was cost-effective and easily reproduced at other academic institutions. However, it still must be determined if these acquired skills transfer to environments outside the laboratory.
In an effort to satisfy the American Board of Orthopaedic Surgery (ABOS) requirement for a month-long orthopaedic skills rotation, programs often construct a skills curriculum that is procedurally based. As an alternative, we describe here a skills program that teaches individual tool skills to fluency (accuracy at speed) using instructional modules that are innovative, challenging, inexpensive, and when combined with an operant learning program, encourage deliberate practice. 1 , 2 Work hour regulations, time and work load constraints on surgeon teachers, minimally invasive surgery, and the decreasing tool skills that orthopaedic learners bring to a residency program make it essential that orthopaedic programs create a curriculum that targets the training of those specific skills. 3 To insure that those skills are acquired, the American Board of Orthopaedic Surgery (ABOS) now requires a 1-month rotation be added to the orthopaedic curriculum that is dedicated to orthopaedic skill training. 4 As part of the response to this challenge, surgical skills education has moved to the laboratory where residents can practice on models, cadavers, and computer simulators to better prepare them for the operating room experience. 3 It is common for skill curricula to be procedurally based and aimed at solving complex problems while attempting to emulate reality. Unfortunately, this can add to the learning challenge. When simulation realism (fidelity) is over-enhanced, the desired learning outcome may be missed as a result of cognitive and sensory overload. 5
Recently, an operant learning methodology has been used in orthopaedic education to create precise skills (complex behaviors) by highly reinforcing a skill’s component behaviors. 2 The component behaviors are then reconnected to form the desired, fluent, complex behavior. To accomplish this for an array of complex tool behaviors, it was necessary to design a curriculum and learning platforms that allowed for the foundation and component behaviors to be taught and reinforced.
The goals of this project were as follows:
Design training modules that were tool specific and focused on teaching and reinforcing the foundation and component behaviors needed to use tools considered essential for performing orthopaedic surgery. Create training modules that were additive and allowed for the formation of the complex behaviors necessary to fluently use the tools in a variety of environmental circumstances. Build modules that used inexpensive tools and substrates, were interesting and challenging, and supported repetition and deliberate practice. Evaluate each module’s performance and acceptance by the learners.
Methods
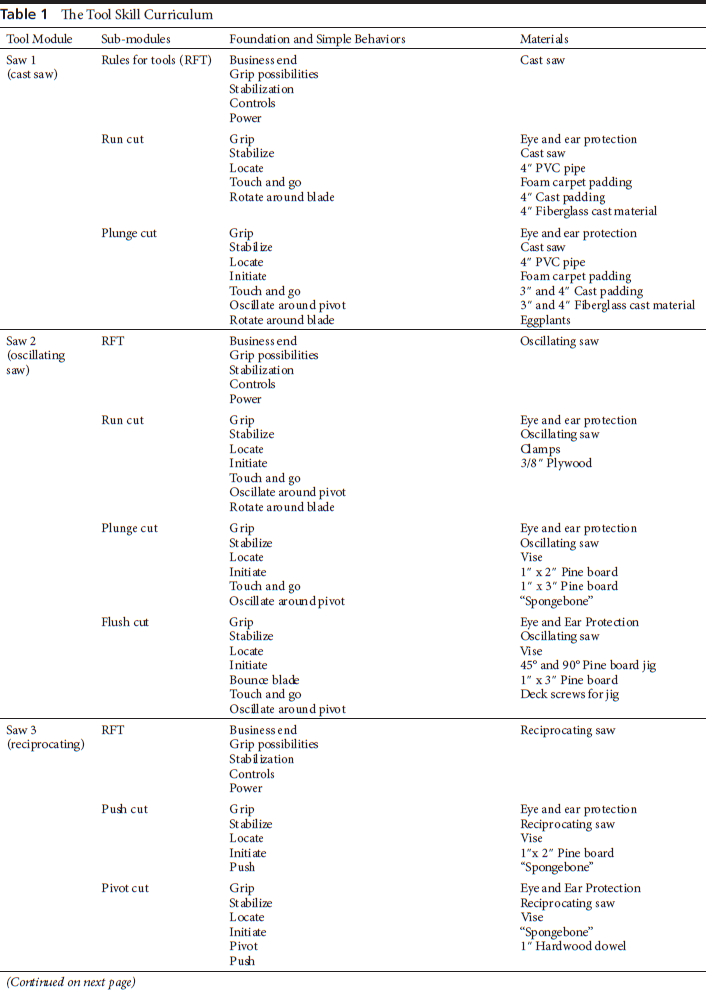
The Albert Einstein College of Medicine’s Institutional Review Board approved testing and found the project exempt because of its use of normal educational practices. Fourteen faculty members of the Montefiore Medical Center Department of Orthopaedic Surgery identified 14 tools commonly used in orthopaedic surgery that they thought should be used fluently by a resident surgeon prior to using them in an operating room. The group identified the complex behaviors needed to use those tools and then delineated the foundation and component behaviors necessary to form those complex behaviors. Modules and their related sub-modules were designed to establish those formative behaviors. One sub-module for each tool was dedicated to delineating the “Rules for Tools” for that specific tool (Table 1). In that sub-module, the point of action (business end), grip and stabilization options, the controls, and the power source were identified. Sixteen, 4-hour, instrument specific modules (the drill was used in three modules; as a drill, a screw driver, and as a reamer) were designed and pre-tested for performance with the 2013 PGY-1 class over a 6-month period (January to June, 2014). The 16 instrument modules and 72 sub-modules were then presented to the 2014 and 2015 PGY-1 classes during each class’s 1-month orthopaedic skills rotation (July 2014 and July 2015). Each module and its sub-modules were supervised by a faculty member who was an expert in the skill’s performance and who was involved in the development of that specific module.
The Tool Skill Curriculum







For the suture module, small caliber cotton rope and 20-pound test Dacron fishing-line (Cabela’s, Sidney, NE) were used for knot tying (Table 1). For the needle holder component of the module, a 7 inch Mayo-Hegar needle holder (Symmetry Surgical®, Antioch, TN) was used along with Martin’s Uterine 1/2 Circle Reverse Cutting Richard- Allan® Needles (Aspen Surgical™ Products, Caledonia, MI), Dacron fishing-line, and baseballs with their stitching removed (Rawlings, St Louis, MO).
For the scissors module, Metzenbaum scissors, Adson forceps (Symmetry Surgical, Antioch, TN), and meat products (breast of veal, pig feet) were used. The materials used for practice for the chisel (Craftsman Studio, Millbury, MA), osteotome (Innomed Inc., Savannah, GA), rongeur and curette (Aesculap Inc., Center Valley, PA) modules, included soft wood, Masonite, butternut squash, pumpkins, and hard boiled eggs.
For the drill modules, 12-volt battery powered drill/drivers (DeWALT Industrial Tool Co., Baltimore, MD) and standard twist drill bits (DeWALT Industrial Tool Co., Ryobi Limited, Anderson, SC) were employed. For reaming activities, a multi-tool with a coupled driver head (Ridge Tool Co., Elyria, OH), acetabular reamers (Stryker Corp., Kalamazoo, MI), and cannulated reamers (Smith and Nephew, Inc., Andover, MA) were used. For the high-speed drilling modules, variable speed rotary tools (Dremel®, Robert Bosch Tool Corp., Mount Prospect, IL) were used. While PVC pipe was useful for most drilling projects, it did not have the ‘feel’ of bone and was not reliable for teaching plunge prevention. A “plunge stick” (a composite of 1”x 2” pine board glued to plywood) was developed, tested, and ultimately used for this purpose. The composite created the feel of cortical penetration. Deck screws of varying lengths were used for screw placement and fixation. A purpose-built material made from large pore sponges and plaster-of-Paris, “Spongebone,” was designed, tested, and used for the reaming modules (Tables 1 and 2, Fig. 1). Eggplants were used to hide the PVC pipe for the “Blind” Drilling and the “Perfect-Circle” sub-modules. A mini-C arm borrowed from the Department of Orthopaedics clinical office was used for these sub-modules.
Making “Sponge Bone”


“Spongebone” is a purpose-built material made from large pore sponges and plaster-of-Paris and was used with the reaming and saw modules.
The saw modules used two sets of AC powered multitool oscillating saws (Craftsman/Sears Holdings, Hoffman Estates, IL and Ridge Tool Co.), an AC powered reciprocating saw (Ridge Tool Co.), a 12-volt battery powered reciprocating saw (DeWALT Industrial Tool Co.), and a cast-saw (Stryker Corp.). Two sets of oscillating and reciprocating saws were required because of overheating of the tools while completing the modules. One inch by two-inch and one inch by three- inch boards of untreated pine, along with PVC pipe of varying diameters were used for the saw modules. “Spongebone” was also used in these modules. The cast saw module used fiberglass-casting material and cast padding placed over 4” PVC pipe covered with carpet under-padding. Eggplants covered with fiberglass-casting material and cast padding were also used in the cast saw module (Table 1, Fig. 2).

Eggplants were covered with fiberglass-casting material and cast padding and were used in the cast saw module.
Video, hand, and power equipment for the arthroscopy modules were loaned or donated by the manufacturers (Stryker Corp. and Smith and Nephew, Inc.). Arthroscopy modules used grapefruits as a practice medium. Celery and carrots were placed in the grapefruits for practice with hand and power instrumentation as well as for suture placement (Table 1, Fig. 3). Small vacuum pumps (Medline Industries, Inc., Mundelein, IL) were available to maintain a dry working field.

Grapefruits were used as a practice medium for the arthroscopy modules. Celery and carrots were placed in the grapefruits for use with hand and power instruments.
Compartment pressure monitors (Stryker Corp.) were deployed on oranges and standard intravenous saline bags as recommended by the ABOS. 6
All of the module curriculums emphasized positive reinforcement of foundation and component behaviors. 2 At the end of each module, the residents were asked to complete projects that required each resident to apply the learned behaviors to more challenging situations. Weekly practice and project sessions were directed, observed, and coached by the curriculum director (IML).
At the end of the orthopaedic skills rotation, the PGY-1 participants were given a task oriented final exam and an anonymous survey (Tables 2 and 3). In this survey, the participants were asked to evaluate their experience, the teaching methods, the instructors, and each of the modules. The faculty was asked to evaluate their specific module.
Final Exam Tasks Give to the 2014 PGY1 Class

The cost of each module was recorded, and materials were divided into reusable (tools and accessories), replaceable (drill bits and blades), and disposable (wood, PVC tubing, and vegetables) items. Costs were tabulated for the entire skills month along with individual reusable, replaceable and disposable total cost. A reusable, replaceable, and disposable averaged cost per module was determined. Using the total costs, a cost per module per student was calculated. The cost of the room itself was not considered in the calculation as it was pre-existing, and we determined that all of the modules could be completed in non-dedicated facilities.
Results
Observations by the learners and faculty indicated that the materials used for the modules were effective, and the modules and sub-modules were challenging. The meat products (specifically breast of veal) were an excellent substrate for the scissor sub-modules. Dacron fishing-line had the stiffness of suture without the cost. The baseballs proved valuable for targeting with a needle. PVC pipe of varying diameters, untreated pine board, and “plunge sticks” were excellent drill sub-module substrates. “Spongebone” was an inexpensive and worthwhile material for the acetabular reaming module. Saw related behaviors were easily acquired using pine board, plywood, PVC pipe, and Spongebone. Casts placed on eggplants were used to evaluate plunging with cast saws and were very effective for both instruction and evaluation. Pine board and butternut squash were effective substrates for the hard tissue instrument (osteotome, rongeur, and curette) modules. Grapefruits made for an effective and challenging arthroscopy training model. Carrots and celery placed within the grapefruits allowed for arthroscopic hand and power instrument practice.
All six members (three males and three females) of the 2014 PGY-1 orthopaedic surgery class and all six members (six males) of the 2015 PGY-1 class participated in all 16 modules during their respective orthopaedic skills rotation. All six members of the 2014 PGY-1 class completed the final exam tasks. One member of the class was unsuccessful at one knot tying task and another member did not successfully perform the plunge board test (Table 3). All six members of the both PGY-1 (2014-2015) classes filled out the anonymous survey (Table 4). Results of the survey indicated that for July of 2014 and 2015 teachers clearly communicated the goals of the modules 77% (2014) and 100% (2015), gave clear instructions 85% (2014) and 100% (2015), and contributed to the success of the module of 85% (2014) and 100% (2015) of the time. When asked about where they had achieved a “comfort level,” the reamer, cast saw, and arthroscope remained challenging at end of the skill module, for both years. For the 2014 group, the osteotome and rongeur modules were not considered valuable. For the 2015 class, the acetabular reamer and the pressure modules were not considered valuable. Both groups asked for more time with the cast saw and oscillating saw. All 12 participants would recommend the skills laboratory to others, wanted to participate in future teaching sessions, and would like refresher modules to be offered.
The 2014-2015 Survey and Results


A wide range of inexpensive materials were used for the sub-modules. The total, one time, fixed equipment costs for all 16 modules was $10,032 ($1,672/resident, $627/module) and $105/resident/module. The total, replaceable equipment (bits, blades, etc.) cost was $774 ($129/resident, $48/module) and $8/resident/module. The total, disposable items cost was $924 ($154/resident, $58/module) and $9/resident/module. The total cost for the skills month was $11,730 ($1,955/ resident, $733/module) and $122/resident/module.
Discussion
The ABOS now requires all residency programs to incorporate orthopaedic skills training into their PGY-1 educational cur- riculum. 4 While surgical skills can be trained or enhanced with models, cadavers, or simulators in the laboratory setting, it is not clear that these measures improve performance in the operating room. 7 In addition, the models, simulators, and cadaver specimens used in the laboratory can be expensive and often use resources that are limited. This can result in an experience that is
Footnotes
Conflict of Interest Statement
During the study period, the institution of three authors (IML, EDF, JFS), Montefiore Medical Center, received research funding from the American Board of Orthopaedic Surgery and the OMeGA Medical Grants Association. One author (TRK) is an employee of TAGteach International. One author (KWP) is a retired employee of Karen Pryor Clicker Training. The authors declare no competing interest.