
Abstract
Background: Previous studies have investigated the longterm outcomes of slipped capital femoral epiphysis (SCFE) treatment but have not fully elucidated the specific underlying risk factors for the need for secondary surgery. The purpose of this study was to examine a series of patients treated for SCFE at a single institution to identify risk factors for the need for secondary procedures following in situ pinning.
Methods: The medical records of 87 patients (125 hips) ranging in age from 9 to 16 years who underwent in situ pinning for SCFE between 2008 and 2013 were retrospectively evaluated. Patients with less than 1 year of follow-up were excluded. Demographic information, slip classification, and slip severity were determined. Secondary procedures were defined as hardware removal, femoral osteotomy, or total hip arthroplasty. Both individual hips and individual patients were analyzed to determine the risk of requiring a secondary procedure.
Results: A total of 46 patients (65 hips) with average follow-up of 28 months (range: 12 to 78 months) met inclusion criteria. In total, 18 hips (28%) required a secondary procedure, including femoral osteotomy (4) and hardware removal (14). There were no cases of total hip arthroplasty. There was a significantly higher risk of requiring secondary procedures in female hips (HR = 4.91, 95% CI = 1.48-16.3, p = 0.01). There were no significant differences related to age, BMI, race, hip pain, slip classification, Southwick angle, slip grade, or tri-radiate cartilage status. Similarly, analysis of individual patients showed a significantly higher proportion of secondary procedures in female patients (p = 0.002).
Conclusion: Female sex was the only factor associated with a higher risk for secondary surgery following in situ pinning with a 4.9 time higher rate for secondary procedures compared to males. Slip classification and slip severity were not found to be associated with the need for secondary surgery. This data helps predict surgical outcomes following SCFE treatment with in situ pinning.
Slipped capital femoral epiphysis (SCFE) is the most common hip disorder in adolescents, with a reported incidence rate of 10.80 per 100,000 children in the USA. 1 It is characterized by a posteroinferior displacement of the capital femoral epiphysis in relation to the metaphysis, occurring through the physis. 2 The average age of SCFE onset is 12 years, and patients can present with ipsilateral groin, thigh, or knee pain, as well as an abnormal gait.1-3
Cases of SCFE can be classified as either stable or unstable. A patient with stable SCFE maintains the ability to ambulate, while a patient with unstable SCFE is unable to ambulate, even with the help of crutches. 2 , 3 They can also be classified as acute or chronic based on the duration of symptoms prior to presentation, with less than 3 weeks being considered acute. 2 The standard treatment for stable SCFE is single screw fixation in situ, while the standard treatment for unstable SCFE remains controversial, although a combination of joint aspiration, closed reduction with single or double screw fixation, and open capital realignment with or without surgical hip dislocation have been recommended.2-8 Although the long-term outcomes of most SCFE cases treated with in situ pinning are favorable, some patients require secondary procedures for residual pain or deformity. These can include hardware removal, femoral osteotomy, surgical hip dislocation with osteochondroplasty, and total hip arthroplasty.9-12
Previous studies have investigated the long-term outcomes of SCFE treatment and commented on the various secondary procedures involved. However, these studies either examined patients originally treated by methods other than in situ pinning or did not fully elucidate what the specific underlying risk factors may be to help predict the need for a secondary procedure. 10 ,13-21 Further understanding of these risk factors could help predict outcomes after initial SCFE treatment with in situ pinning. The goal of the current study was to identify risk factors predictive of the need for secondary procedures following in situ pinning in a consecutive series of SCFE patients treated at a single institution.
Materials and Methods
Following Institutional Review Board approval, 87 patients (125 hips) between 9 and 16 years of age who underwent in situ pinning for SCFE between January 1, 2008, and December 31, 2013, were identified. Departmental databases and billing records from a single institution were searched using Current Procedural Terminology (CPT) code 27176 for treatment of slipped femoral epiphysis by single or multiple pinning in situ and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 732.2 for nontraumatic slipped upper femoral epiphysis. These two lists were cross-referenced to remove duplicate entries. Forty-one patients (60 hips) with less than 1 year of follow-up were excluded. A total of 46 patients (65 hips) met the inclusion criteria.
Electronic medical records and radiographs were retrospectively reviewed to determine demographic information, slip severity, slip classification, and outcome data. Outcome measures were based on secondary surgery or most recent follow-up if no secondary procedure was required. Secondary procedures were defined as hardware removal, femoral osteotomy, surgical hip dislocation, or total hip arthroplasty. Time to outcome was calculated based on the initial pinning date.
Slip severity was assessed by measuring both slip grade and Southwick slip angle. The Wilson method was used to measure slip grade on frog-leg lateral radiographs. 22 Each grade corresponds to the amount of epiphyseal displacement on the femoral neck, with grade 1 less than 33% of the femoral neck, grade 2 between 33% to 50% of the femoral neck, and grade 3 greater than 50% of the femoral neck (Fig. 1). Southwick slip angle, also known as epiphyseal-shaft angle, was measured by drawing a line perpendicular to a separate line connecting the anterior and posterior points of the epiphysis on a frog-leg lateral radiograph. A third line was drawn down the shaft of the femur, and the resulting angle between the perpendicular line and shaft line was noted (Fig. 2). The Southwick angle was then calculated by subtracting the angle on the unaffected side from the angle on the affected side. In cases of bilateral SCFE, 12° was used as the angle on the unaffected side. 2 , 23 Radiographs were reviewed by two junior investigators (SS, DM).

Example of slip grade for a patient with left SCFE as measured on anteroposterior radiographs. The amount of epiphyseal displacement is less than 33% of the femoral neck, which indicates a grade 1 slip.
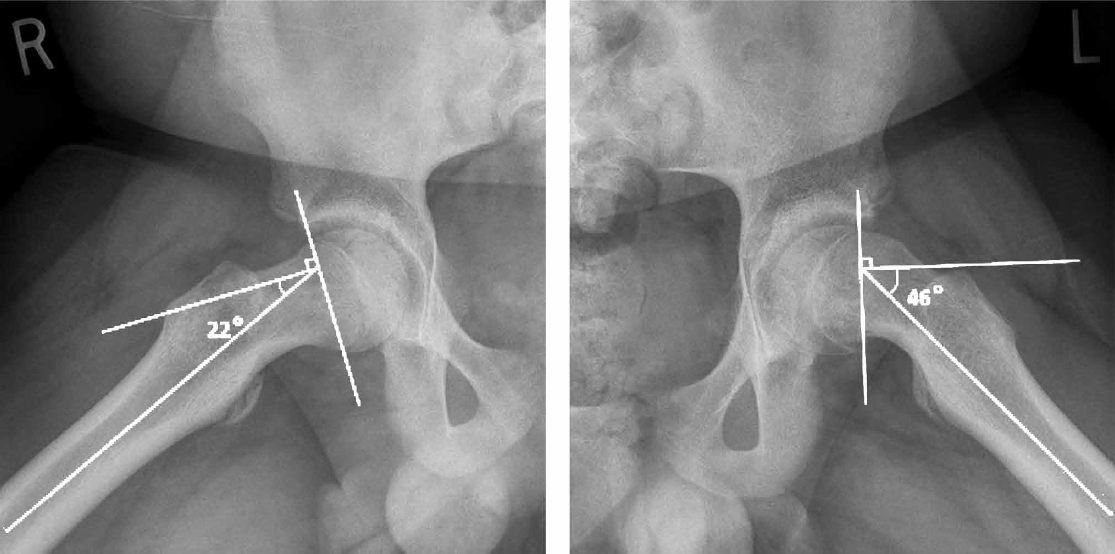
Example of Southwick slip angle for a patient with left sided SCFE as measured on frog-leg lateral radiographs. Angles were 22° on the unaffected side and 46° on the affected side, giving a Southwick angle of 24°.
Slip classification was based on stability, chronicity, and triradiate cartilage status. Stability was assessed using the Loder classification of stable or unstable. 24 In brief, a child with a stable slip is able to ambulate with or without crutches, while a child with an unstable slip is unable to ambulate. Chronicity was based on duration of symptoms, with 3 weeks being the cutoff for acute versus chronic slips. Acute on chronic slips were defined as those patients with an acute exacerbation of a chronic slip. 25 Triradiate cartilage status was judged to be open or closed based on agreement by the two senior investigators (EF, JS).
Risk factors for secondary hip procedures were analyzed by individual hip and by individual patient. For individual hips (65), the Cox proportional hazards model for clustered time to outcome data was used to detect factors predicting secondary hip procedures and to calculate the corresponding hazard ratios. Hazard ratios were provided based on sex, age, race, BMI, BMI%, pre-pinning Southwick angle, affected side, hip pain at most recent follow-up, slip stability, slip chronicity, slip grade, and triradiate cartilage status.
For the analysis by individual patients, 3 of the 46 patients were excluded; 2 patients had bilateral slips but only 1 hip required a secondary procedure, and 1 patient who had 2 hips requiring a secondary procedure but who underwent original pinning of each hip on a separate date. Individual patients were analyzed using Fisher’s exact test for categorical variables and two sample t-tests for continuous variables. For patients with bilateral pinning on separate dates and no secondary procedure, information related to the earlier pinning was used for analysis.
Results
A total of 46 patients (65 hips) with average follow-up of 28 months (range: 12 to 78 months) met the inclusion criteria.
Individual Hips
A total of 65 hips met the inclusion criteria for individual hip analysis. In total, 18 hips (28%) required a secondary procedure, including 4 cases of femoral osteotomy and 14 cases of hardware removal. Indications for secondary procedures included symptomatic persistent deformities, symptomatic pain, or a planned secondary procedure. There were no cases of total hip arthroplasty or surgical hip dislocation. Of the 65 hips, 43 (66.2%) were male and 22 (33.8%) were female. Mean follow-up was 2.5 years (range: 1 to 6.5 years). Average age at pinning was 12 years (range: 9 to 16 years). Average BMI percentile was 92 (range: 23.9 to 99.8). Regarding slip severity, 52 hips (80%) were classified as grade 1, 8 hips (12.3%) as grade 2, 3 hips (4.6%) as grade 3, and 2 hips (3.1%) were unable to be recorded. The average Southwick angle was 25.2° (range: 3.9° to 66.3°). Slip
classification was determined to be stable in 60 hips and unstable in 5 hips. Acute slips accounted for 9 hips (13.8%), 13 slips (20%) were acute on chronic, and 43 slips (66.2%) were chronic. Triradiate cartilage status was determined to be closed in 30 hips (46.2%), open in 32 hips (49.2%), and unavailable in 3 hips (4.6%). There were no cases of AVN or chondrolysis in this cohort.
Analysis of individual hips showed a significantly higher risk of undergoing secondary procedures in female hips (HR = 4.91, 95% CI = 1.48-16.3, p = 0.01) compared to male hips (Table 1). There were no statistically significant differences related to other demographic information, slip classification, or slip severity. A complete list of comparative parameters for individual hips is shown in Table 1.
Individual Hip Hazard Ratios for Requiring a Secondary Procedure

p ≤ 0.05; †1here were no cases of grade III slips that required a secondary-procedure. Time to outcome was defined as the number of days between in situ pinning and either most recent follow-up or secondary procedure date.
Individual Patients
A total of 43 patients met the inclusion criteria for individual patient analysis. In total, 11 patients (26%) required a secondary procedure, including 1 case of femoral osteotomy and 10 cases of hardware removal. There were no cases of total hip arthroplasty or surgical hip dislocation. Of the 43 patients, 28 (65.1%) were male and 15 (34.9%) were female. Mean follow-up was 2 years and 4 months (range: 1 to 6.5 years). The average age at pinning was 12 years (range: 9 to 16 years). The average BMI percentile was 92.2 (range: 23.9 to 99.8).
Analysis of individual patients showed that female patients underwent a significantly higher proportion of secondary procedures (p = 0.002) compared to male patients (Table 2). There were no statistically significant differences in other demographic information. A complete list of comparative parameters for individual patients is shown in Table 2.
Overall Patient Demographics at In Situ Pinning Date
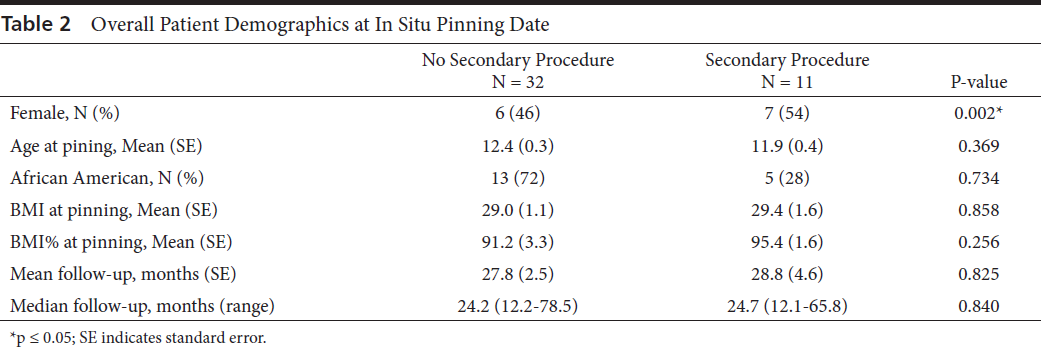
p ≤ 0.05; SE indicates standard error.
Discussion
This study provides further insight into the clinical outcome of patients treated for SCFE with in situ pinning. While previous studies have investigated the long-term outcomes of various treatment modalities, they have not fully elucidated the underlying risk factors for the need for secondary surgery. Secondary procedures were performed in 28% of hips in our cohort, including 4 cases of femoral osteotomy, 14 cases of hardware removal, and no cases of total hip arthroplasty or surgical hip dislocation. These findings are similar to those presented elsewhere in the literature. 10 , 13 , 20 , 21 , 26 , 27
Slip classification and slip severity were not found to be associated with the need for secondary surgery in our cohort. These findings are similar to patient reported outcomes found by Escott and associates, although they did not investigate the association with secondary surgery. 15 It has been proposed that this may be due to the propensity for bone remodeling following in situ pinning. 15 , 28 , 29
Larson and coworkers found no association between slip stability or slip acuity and the need for secondary procedures in their retrospective review of 176 hips treated with in situ pinning for SCFE but did report a statistically significant association between slip severity and more frequent reconstructive surgery, which our findings did not suggest. 10 This variation could be due to differences in the sample populations, as their cohort included more patients with severe slips and greater power as a result.
Female sex was the only factor associated with the need for secondary surgery following in situ pinning, as this was significant in the analyses of both individual hips (p = 0.01) and individual patients (p = 0.002) when compared to males. In essence, this hazard ratio indicates that female hips underwent secondary procedures at 4.91 times the rate per unit time as male patients in our population. Although no studies have investigated this risk factor in relation to secondary procedures, Escott and colleagues recently found a similar association between female sex and negatively associated patient reported outcomes related to pain, physical function, and general health. 15 Although the underlying etiology of these sex specific variations is uncertain, a combination of anatomical and self-perceptual differences has been sug- gested. 15 , 30 , 31
The limitations of this study include those associated with a retrospective review, including availability and consistency of documentation. Additionally, current patient reported outcomes could not be assessed because of difficulty contacting patients, which would have allowed for supplementary comparison to similar studies. Although the follow-up for the majority of our patients (63%) was more than 2 years, 17% of patients had a follow-up of 1.5 years, and 20% of patients had a 1-year follow-up. Increased length of follow-up may have revealed additional patients requiring secondary procedures, although we attempted to account for this fact by using the Cox proportional hazards model and time to outcome data for statistical analysis.
In summary, our study examines specific risk factors for the need for secondary surgery following in situ pinning for SCFE. Multiple analyses of our cohort found that both female hips and female patients demonstrated a significantly increased risk for secondary surgery. Slip classification and slip severity were not found to be associated with the need for secondary surgery. These findings help to predict surgical outcomes following in situ pinning for SCFE and identify specific patients at risk for secondary procedures. As has been suggested elsewhere in the literature, additional research, particularly prospective and comparative studies, is needed to better understand outcomes following treatment for SCFE. 32 It is especially important to understand both expected outcomes and risk factors as treatment modalities continue to evolve.
Footnotes
Conflict of Interest Statement
None of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.