
Abstract
Cerebral oedema has been noted to occur frequently in patients dying of fulminant hepatic failure. Therefore, in the present study, multimodal neuromonitoring was evaluated in an animal model of hepatectomy. Acute liver failure was surgically induced in swine by complete hepatectomy (
The clinical syndrome of fulminant hepatic failure (FHF) is complex and yet only incompletely understood. As mortality rates of at least 50% in humans are reported, FHF is still a major clinical challenge. 1 Hepatic encephalopathy and cerebral oedema resulting in elevated intracranial pressure are the leading causes of death for FHF. 2–5 To study its pathophysiology and new therapeutic approaches, numerous animal models have been investigated within the last decades. 6–9 Surgical models consist of ischaemia, portocaval (PC) shunting, subtotal liver resection or complete hepatectomy. 10–20 We chose a porcine model as swine are a predictable large animal model and most suitable for many experimental studies due to the similarity in many aspects of anatomy and physiology to humans. 21 For our investigation, animals underwent a total hepatectomy followed by the implementation of PC shunt prothesis. 22 As continuous monitoring is even more predictable under conditions of anaesthesia, animals were kept anaesthetized and observed for clinical signs and laboratory parameters of hepatic failure until death.
Up to now, there are no sufficient standardized parameters available that account for hepatic encephalopathy in animal models. 23 Therefore we included a multimodular ‘neuromonitoring’ (intracranial pressure [ICP] monitoring, visually evoked potentials [EVOPs] and liquor sampling) into a previously described hepatectomy model 22 to define an easy, practicable and reproducible method allowing estimation of the severity of hepatic encephalopathy.
Materials and methods
Animals
The study was performed on eight female pigs of the German Landrace breed with a mean body weight (BW) of 37 ± 4 kg (source of the animals: Hartmann, Kalkar, Germany). Prior to investigation the animals were adapted to climate- and light-cycle-controlled environment for at least 14 days. All animals were allowed standard laboratory food and water
Anaesthesia
Premedication (10 mg/kg BW azaperone and 0.025 mg/kg BW atropinsulphate) was applied intramuscularly in all animals. Animals received thiopental (12.5 mg/kg BW) and fentanyl (0.005 mg/kg BW) intravenously for oral intubation. Afterwards animals were ventilated by intermittent positive pressure with 1/3 oxygen using a ventilog respirator (Dräger, Lubeck, Germany). The tidal volume was kept between 300 and 450 mL using a ventilation rate between 10 and 15 per minute. Thiopental was administered continuously and boli of fentanyl were given to maintain the intravenous anaesthesia. 21
Eye movement, character of respiration and heart rate were mainly used to evaluate the depth of anaesthesia. Ventilation was adjusted to the arterial blood gas analysis routinely every hour. Sodium bicarbonate was administered as needed to maintain blood gas parameters within a normal range.
The pigs received NaCl 0.9% as an electrolyte solution, adjusted to arterial and central venous pressure. The total volume of infusion was kept as low as possible to avoid pulmonary and cerebral oedema. The systolic blood pressure was expected to be between 70 and 100 mmHg during operation.
Surgical procedure
Hepatectomy was performed under sterile conditions based on the method previously described by our group. 24 The supra- and infrahepatic caval veins were exposed, mobilized and controlled by a tourniquet. The retrohepatic vena cava was isolated from the posterior abdominal wall; diaphragmatic veins were ligated. The portal vein was then isolated from the porta hepatis to the pancreas and also controlled by a tourniquet. The common hepatic artery was identified, and then all arterial branches to the liver were separated as closely to the hilum of the liver as possible. The common hepatic bile duct was identified in the liver hilum, separated and ligated. The remaining hepato-duodenal ligament was also dissected. Then the portal vein was clamped and dissected. The liver and the hepatic part of the vena cava were removed completely after dissection of the vena cava. To reduce operative stress by shortening the vascular clamping time, a simple shunting system (Y-adapter with three silicon tubes) was implemented into the upper and lower vena cava and portal vein and fixed in place. 25
Neuromonitoring
EVOP
Skin electrodes for registration of cortical activities were positioned on the pig's head. Three stainless steel wires of 4 cm long and with 1 mm diameter were used and connected to isolated cables. Two of them were inserted above the frontal bone close to the periost utilizing the incision already made for the application of the ventricular drainage system. The third electrode was positioned adjacent to the ear. 26
Visual stimulation
A stroboscope was used for visual stimulation. The light flashes were applied as whole-field stimuli with a rate of about 1 Hz. By using a diffusing lens in front of the eye and mydriatic eyedrops, stimulation of the whole retina was achieved. For optimal stimulation the stroboscope was placed in the centre of the visual field of either the right or the left eye. The distance to the eye was 1 m.
Signal recording
In order to achieve high-quality recordings, we used the skin electrodes adjacent to the ear as a recording reference electrode and connected it to the short-circuited inverted inputs of two differential amplifiers. The remaining two electrodes were connected to the non-inverting inputs, respectively. In addition, we connected the ground of the amplifiers to a large indifferent electrode connected with the animal. The signals were amplified with a gain of 10,000 and bandpass-filtered (1–10 kHz). Subsequent sampling of the cortical signals and the trigger channels of the stimulation units by a digital oscilloscope allowed the online calculation of averaged evoked responses and the storage of the data on a hard disc of a personal computer for subsequent data analysis.
Ventriculometry
A genuine ventricular catheter device was used for ICP monitoring (Codman-Microsensor Set, Johnson & Johnson, Raynham, MA, USA), as this seems to be an accurate way of measuring ICP. 27 After a skin incision in the median line above the frontal bone a bur hole was placed. Through the bur hole the catheter was introduced into the third ventricle. The catheter was fixed in place with bone cement and connected with a pressure gauge. 28 ICP and mean arterial pressure were monitored continuously to calculate cerebral perfusion pressure.
Liquor sampling
Liquor samples were taken and ammonia (NH3) levels were determined. After a baseline was taken (prior to hepatectomy), sampling continued during the operation. The results were then compared with the serum NH3 values of the blood samples taken.
General measurements, blood and liquor analysis
Haemodynamic and respiratory parameters (mean arterial blood pressure, central venous pressure, pulse rate, respirator ventilation) were monitored continuously. Blood gas analysis, pH, glucose and electrolyte status were monitored hourly (ABL 700; Radiometer Medical, Brønshøj, Denmark). Blood samples were taken and analysed for the status of the liver function preoperatively, intraoperatively and every second hour in the postoperative course. Blood samples including coagulation factors (BCS; Dade Behring, Marburg, Germany), NH3 and lactate (Dimension RxL; Dade Behring) were measured by standard laboratory techniques according to the manufacturers' recommendation.
Necropsy
Anaesthesia was terminal. In all cases death was caused by cardiocirculatory insufficiency, confirmed by autopsy. Necropsy was performed in all cases, including histopathological examination of brain tissue.
Statistical analysis
Statistical analysis was performed by using SPSS (10.0). Results are presented as mean ± standard deviation (SD). A
Results
After hepatectomy the ‘tube-prothesis’ was successfully implemented without need for extracorporeal bypass circulation. Operation time was 2 h 10 min to 3 h 5 min. Total surgical blood loss was less than 500 mL in all cases. Perioperative surgical and anaesthesiological complications were not observed. Due to loss of the functional liver mass, the dosage of sedative agents to maintain depth of sedation could be reduced after hepatectomy. Mean survival time was 16.7 ± 5.2 h.
Neuromonitoring
EVOP
Shortly after hepatectomy, visual stimulation yielded distinct cortex responses at a delay of up to 30 ms (Figure 1). In the course of each case, an increasing delay of cortex responses up to a maximum of 50 ms was noted together with an increasing extension of the response amplitudes (Figure 2). At the end, cardiac arrest occurred and correspondingly no further cortical responses could be recorded.
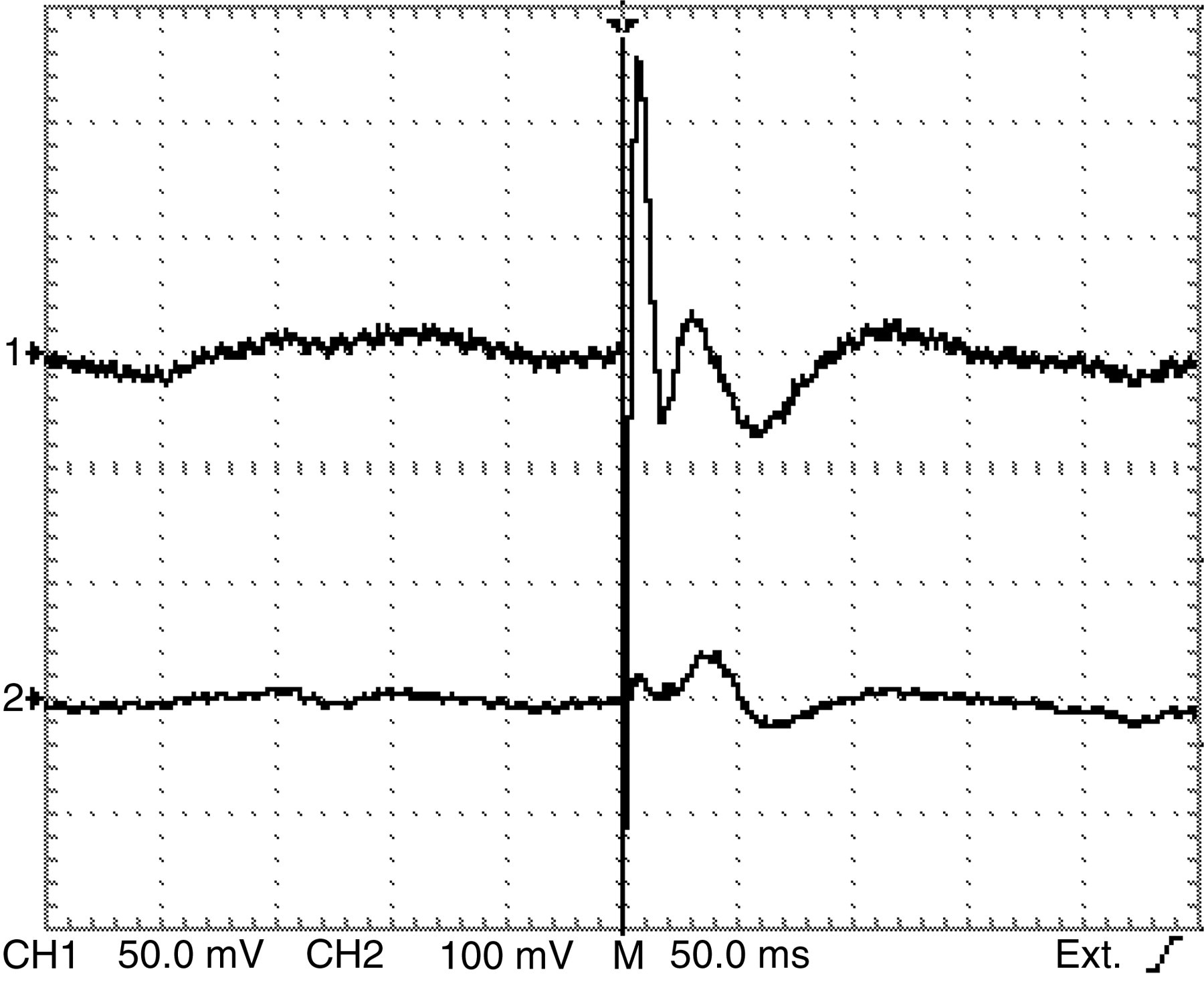
Visually evoked cortical potentials early after hepatectomy in a single case. First wave extrema occur at a delay of 30 ms; 64 signals were averaged. Artefacts appear at 0 ms. Arrow indicates visual stimulation
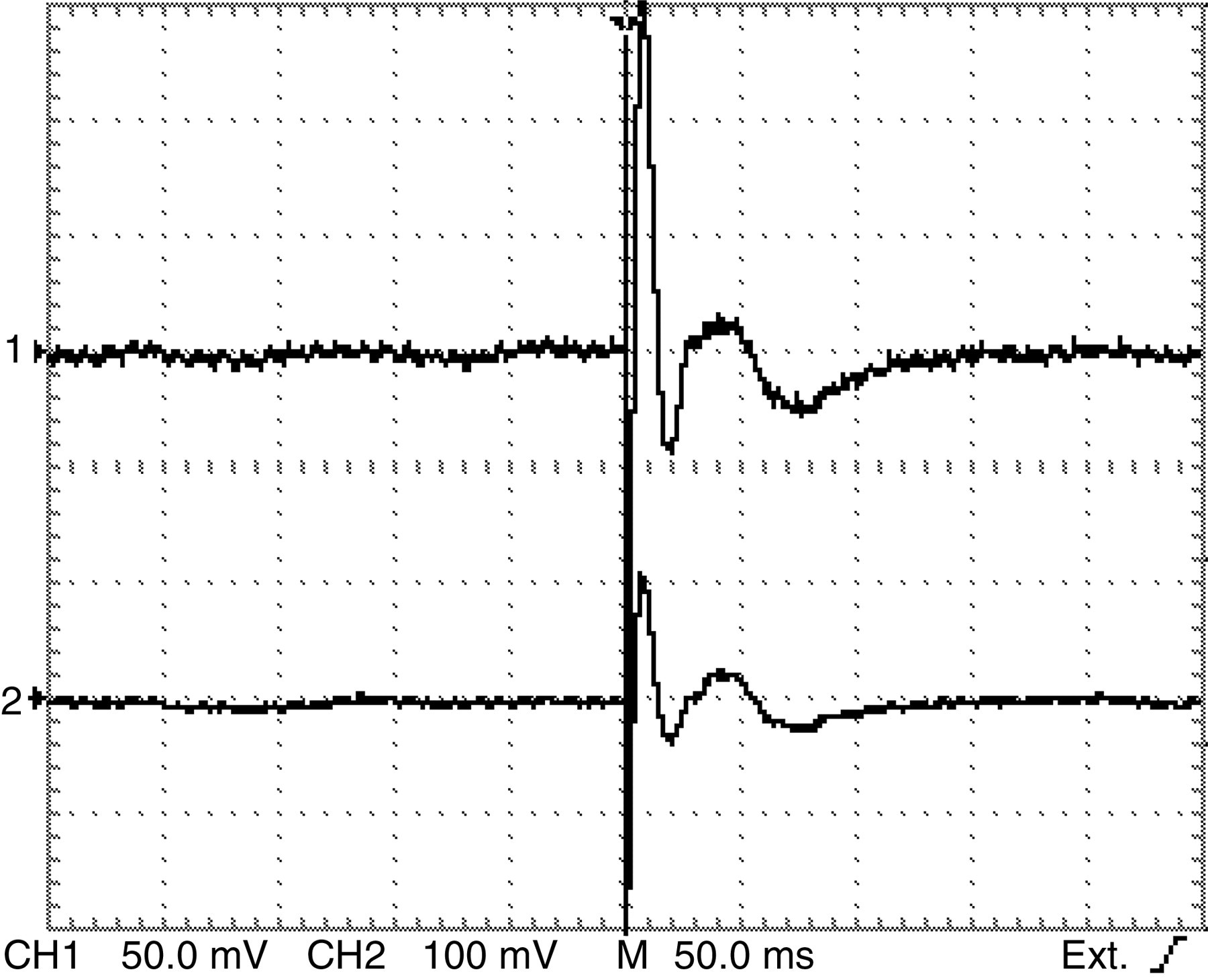
Visually evoked cortical potentials at the end of the same case as shown in Figure 1, 14 h after hepatectomy. First wave extrema occur at a delay of 48 ms; 64 signals were averaged. Artefacts appear at 0 ms. Arrow indicates visual stimulation
ICP monitoring
ICP probes were placed prior to abdominal surgery without any complications. Pigs presented a shallow curve after hepatectomy and total values of ICP below 20 mmHg. Cerebral perfusion remained stable within the first 9 h (Figure 3).
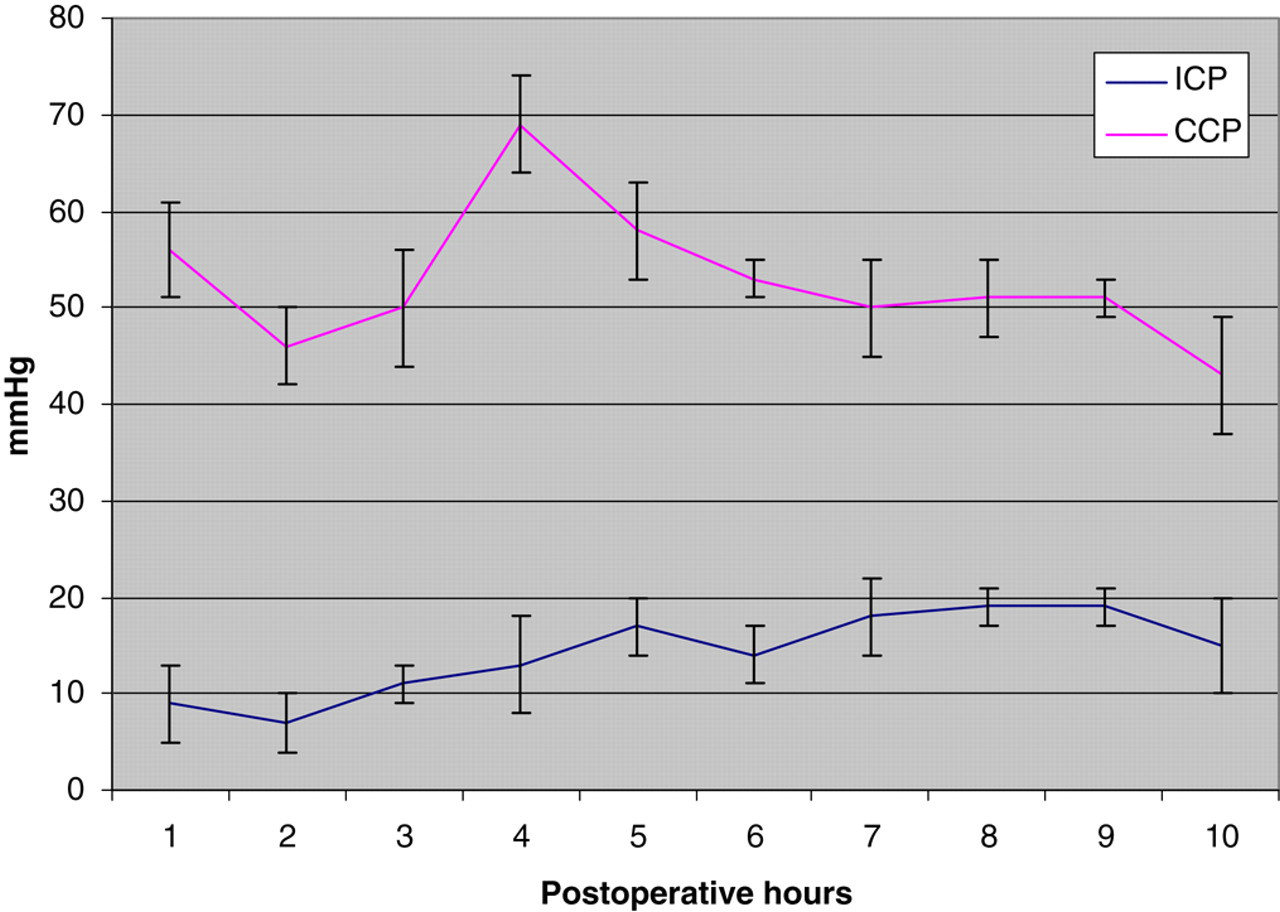
Intracranial pressure (ICP) and coronary perfusion pressure (CCP) values (mean ± SD). Time points are defined as: after trepanation (baseline), prior to hepatectomy (1 h), following course after hepatectomy (2–10 h)
Laboratory analysis
Serum and liquor levels of NH3 were calculated and compared. The increase in serum NH3 levels was paralleled by the liquor levels within the entire postoperative period. The overall increase was more rapid within the first 4 h after hepatectomy and reached a plateau at about 550 μg/dL before a second increase took place after 7 h (Figure 4).
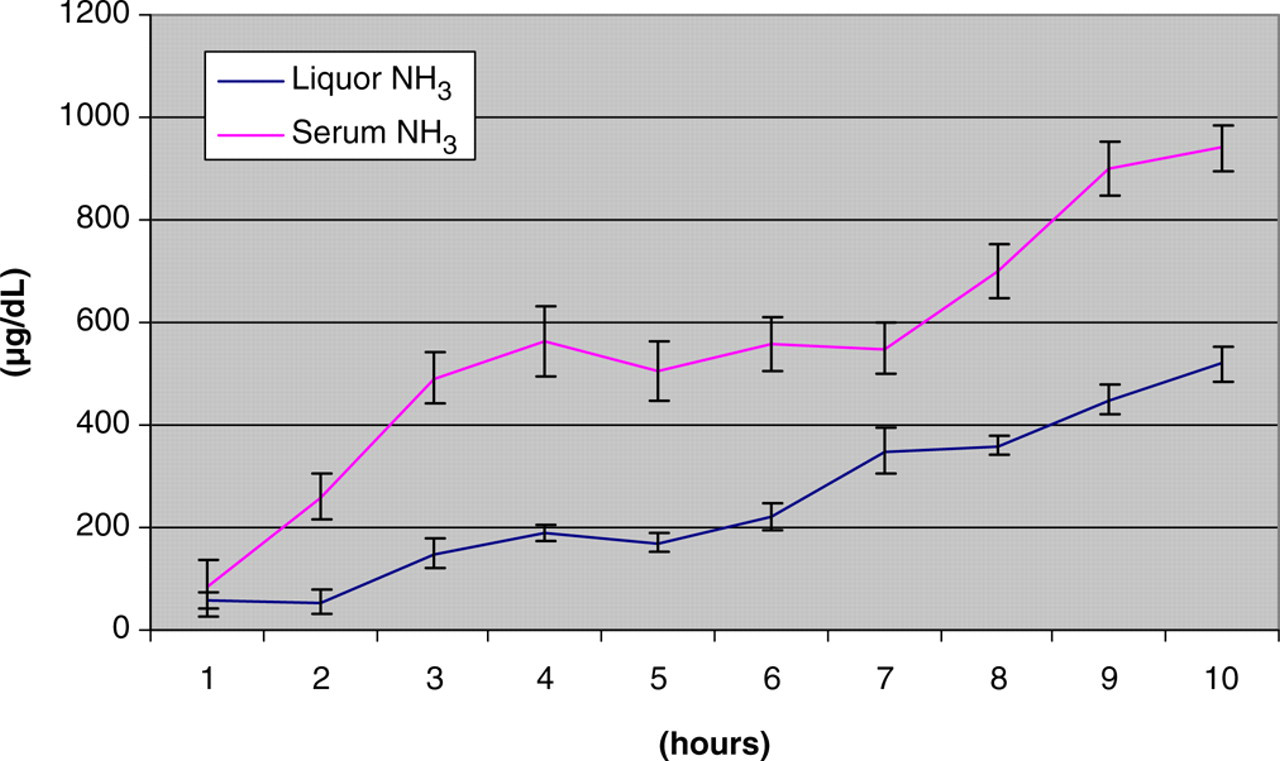
Liquor and serum NH3 levels (mean ± SD) after trepanation (baseline), prior to hepatectomy (1 h), following course after hepatectomy (2–10 h)
Metabolic acidosis was observed after vascular clamping and corrected by administration of sodium bicarbonate. Mean lactate levels remained fairly constant in the hepatectomized pigs (3.9 ± 0.8 mmol/L 16 h postoperatively). As coagulation parameter, INR demonstrated an early onset of hepatic dysfunction by elevation up to 2.9 ± 0.5 after total hepatectomy. Corresponding results were found for the well-evident decline in antithrombin III (ATIII) and increasing of the clotting time (partial thromboplastin time). Aspartate aminotransferase serum levels remained stable after initial increase to a maximum (52 ± 12 U/L). Similar results are shown for serum levels of glutamate dehydrogenase (GLDH). Diuresis remained stable up to 10 h with an increase in serum-creatinine levels up to 1.9 ± 0.6 mg/dL at the end of the experiment.
In all animals, no significant differences were found in heart rate and arterial and central venous pressure for the first 10 postoperative hours.
Necropsy
In all cases death was caused by cardiocirculatory insufficiency, confirmed by autopsy. Evidence of thrombosis or bleeding of the Y-tube was not observed. Postmortem histopathology of brain tissue showed severe oedema and partial necrosis (Figure 5).
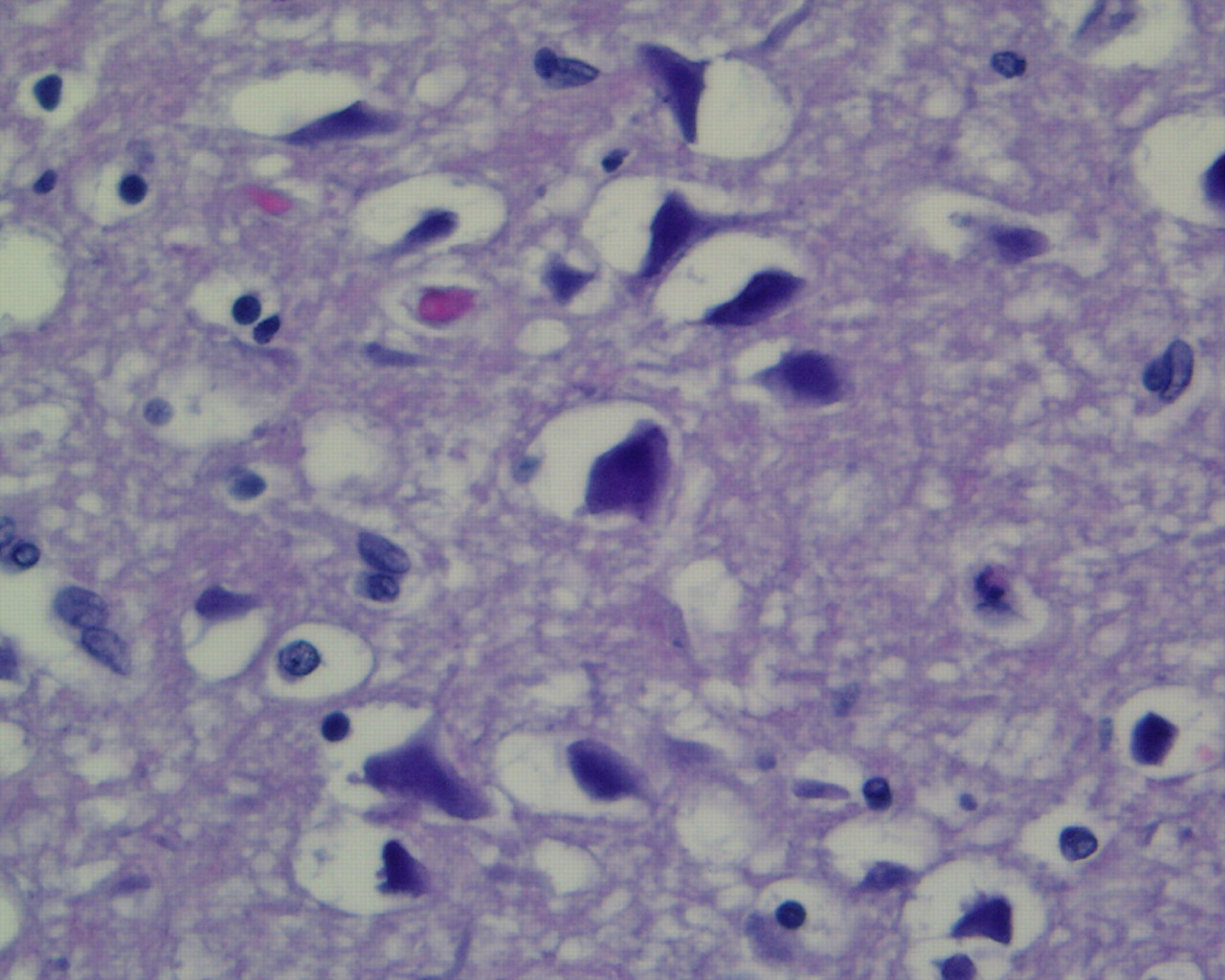
Postmortem histopathology of brain tissue after complete hepatectomy showed severe oedema cellular necrosis, dropout and nuclear debris at a magnification of 1:400
Discussion
Up to 80% of the patients suffering from FHF and hepatic encephalopathy develop cerebral oedema. 29,30 The clinical features of hepatic encephalopathy vary from mild personality change and confusion to deep coma. The progression of hepatic encephalopathy to stages 3 and 4 is commonly associated with raised intracranial pressure. Therefore a differentiated neuromonitoring is substantial in the operating room and intensive care unit. 31
Swine are a predictable large animal model and most suitable for many experimental studies, the similarity in many aspects of anatomy and physiology to the human being is well documented. 32,33 Total hepatectomy represents a loss of all functional liver tissue and can be used as a rescue hepatectomy to exclude toxic side-effects from the necrotic liver tissue in patients. 34 From the surgical point of view, the operation is technically simpler and more easily reproducible than a partial hepatectomy in pigs. To evaluate new treatment modalities, several animal models of hepatic failure have been described within the last decades. It is evident that one model cannot meet all the requirements for an optimal model. 6,7 In our opinion, the model of total hepatectomy should be preferred for the investigations of the anhepatic status and should include neuromonitoring in the future. However, detailed evaluation of neuromonitoring in swine is not reported recently.
Mean survival times in the studies of hepatectomized pigs are described as up to 17 h, which is comparable to our findings with a survival of 16.7 ± 5.2 h. 7,14,15,18 In our study, hepatectomy was a safe procedure with a minimum of blood loss and without persistent severe haemodynamic changes in all pigs. Therefore the hepatectomized pig is a superior model for testing the value of bioartificial liver support systems and for studies of the unhepatic status.
In our experimental set-up the most promising animal model of surgical induced FHF, the status after hepatectomy, was studied by extensive neuromonitoring including EVOP, ICP and liquor sampling. Due to minor influence of thiopental and fentanyl on the ICP, this combination of agents was given to maintain the intravenous anaesthesia. 21 The lactate levels remained fairly constant in the hepatectomized pigs until the end of the experiment. Animals after total hepatectomy showed a rapid decrease of thromboplastin time (TPZ), ATIII and an increase of the clotting time. The serum levels of AST and GLDH demonstrated stable values in animals after initial increase. This was also observed in previous studies although no intrahepatic blood flow exists in the devascularized animals. 20
Worsening of the detoxification function was demonstrated by a significant increase of serum NH3 in the postoperative course. The significant increase of liquor NH3 levels may be interpreted as an indicator of the blood–brain barrier dysfunction. The application of the standardized EVOPs and ICP were uneventful and results were highly reproducible. ICP and cerebral perfusion remained stable within the first 9 h after hepatectomy. As shown, EVOPs demonstrate a prolonged cortical reaction after visual stimulation within the postoperative course after hepatectomy in swine. Therefore, additional monitoring by non-invasive methods of EVOPs gives further information adding to results of ICP monitoring and liquor sampling. Therefore both methods can be interpreted complementarily.
The multimodal technique of extended neuromonitoring offers an advanced option for further developments and investigations in animal models of FHF.