
Abstract
Ovarian vein thrombosis (OVT) is an uncommon but potentially serious postpartum complication, typically affecting the right ovarian vein. This case study provides a rare presentation of left-sided OVT in a 26-year-old woman, 1 week postpartum, which followed a vaginal birth after cesarean (VBAC). The patient presented to the emergency department with persistent left lower quadrant pain, beginning 1 day post-delivery. Laboratory findings revealed leukocytosis and anemia. Sonographic evaluation identified abnormal left adnexal findings, raising suspicion for OVT. Subsequent computed tomography (CT) confirmed thrombus within the left ovarian vein extending into the left renal vein, with associated inflammatory changes. She was admitted for treatment with anticoagulants, analgesics, and referred to hematology. This case highlighted the importance of maintaining a high index of suspicion for OVT, even in atypical presentations, such as left-sided involvement or after vaginal delivery. It underscores the diagnostic value of sonography as a frontline imaging technique and the need for further evaluation using cross-sectional imaging. Sonographers should be aware that although right-sided OVT is more common, left-sided cases can occur, particularly in patients with underlying thrombotic risk factors. Timely diagnosis and management are crucial to prevent serious complications, including thrombus propagation and embolism.
Ovarian vein thrombosis (OVT) is an uncommon diagnosis most often occurring during the peripartum period. 1 Pregnancy predisposes the patient to develop thrombosis (i.e., blood clots) based on the factors of Virchow’s triad: hypercoagulability, venous stasis, and endothelial injury. 2 The incidence of OVT, during the postpartum period, has been found to occur in 0.05% to 0.18% of vaginal deliveries and in 2.0% of cesarean section deliveries. 3 In a published review of OVT patient cases, the mean age of women was 37, but ranged from 20 to 60 years. 4 The classic incidence of OVT has been mostly found in the right ovarian vein. 5 Although this occurrence of OVT is more common, a rare case of left OVT is possible and could be detected with sonography and the use of computed tomography (CT). The case study provided is such an example and is linked to the diagnosis of OVT, which followed a vaginal birth after cesarean (VBAC) delivery.
Case Report
A 26-year-old woman who was 1 week postpartum, after a VBAC, presented to the emergency department, complaining of left lower quadrant pain. The patient stated the pain began 1 day after delivery. The patient’s laboratory results were abnormal with an elevated white blood cell count, decreased hematocrit, and decreased hemoglobin. A referral was made for the patient to have a transabdominal pelvic sonogram.
The sonogram was performed with an Epiq Elite (Philips Medical, Bothell, Washington) equipment system and a C5-1 transducer. The examination consisted of grayscale and color Doppler longitudinal and transverse imaging planes, to investigate the uterus, bilateral ovaries, and adnexal areas. Since the left adnexa was the area of concern, careful scanning of the adnexa from superior to inferior and medially to laterally was performed. In the transverse imaging plane, a tortuous, heterogeneous structure was demonstrated (See Figure 1). Color Doppler was used to evaluate the structure and showed mildly increased vascularity (See Figure 2). The radiologist was consulted and observed the real-time examination, noting that the ovary and fallopian tube could not be differentiated from surrounding structures. The recommendation was for a CT examination for further evaluation of relational structures. The final report stated the left fallopian tube and ovary appeared mildly edematous, which was suspicious for an OVT.
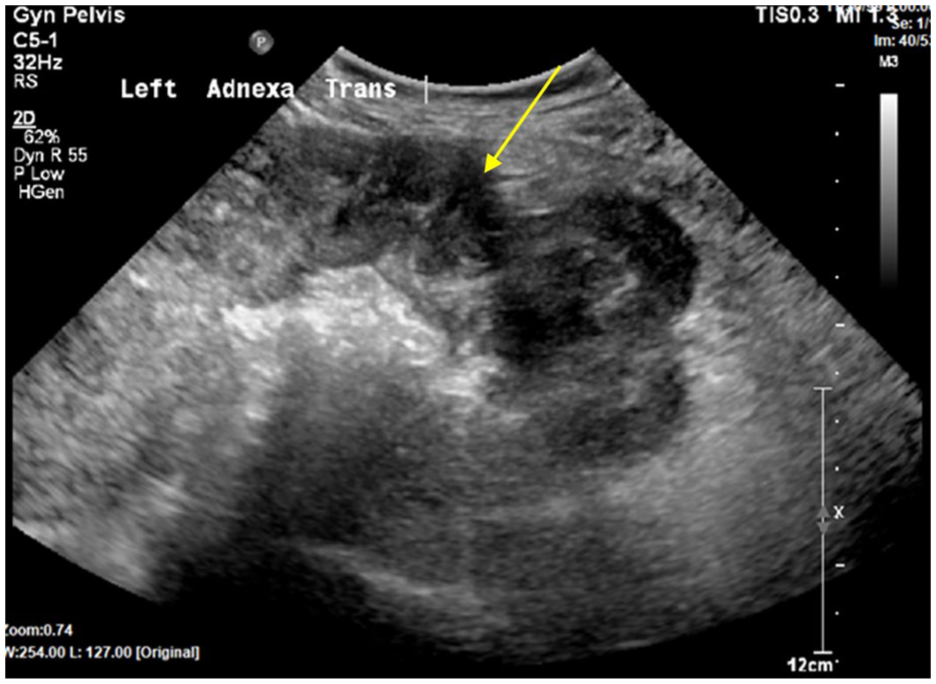
A transabdominal sonogram, in the transverse imaging plane, is provided of the left adnexa and demonstrated a tortuous, echo-filled structure (indicated by the yellow arrow).
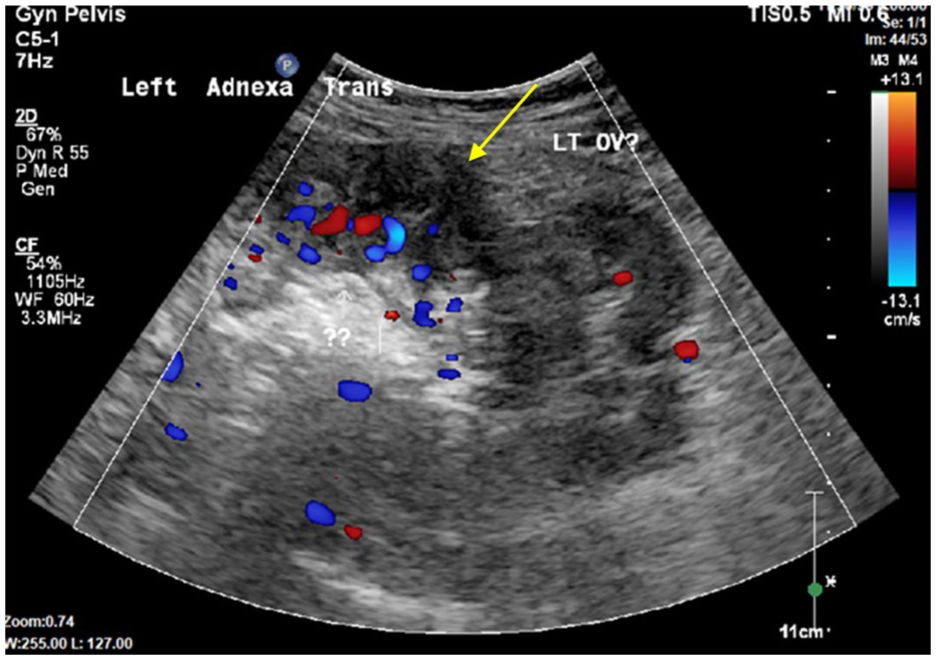
A transabdominal sonogram, in the transverse imaging plane, with color Doppler is provided of the left adnexa and demonstrated a tortuous, echo-filled structure (indicated by the yellow arrow).
A CT angiogram of the abdomen and pelvis was completed on the patient. The pelvic images demonstrated that the left ovarian vein was dilated and filled with thrombus along with surrounding inflammatory changes (See Figure 3). Extension of the thrombus into the left renal vein was identified on abdominal CT cross-sectional images (See Figure 4). These CT diagnostic findings confirmed the presence of a left OVT.
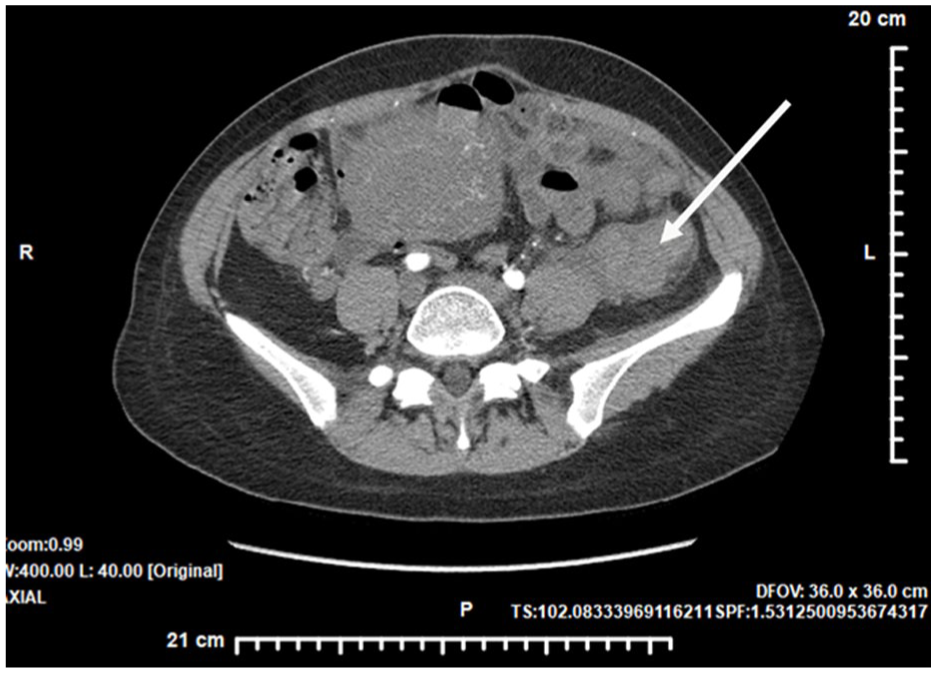
A transverse computed tomographic angiographic image of the pelvis demonstrated a left ovarian venous thrombosis (OVT) (indicated by the white arrow), as well as surrounding inflammatory changes.
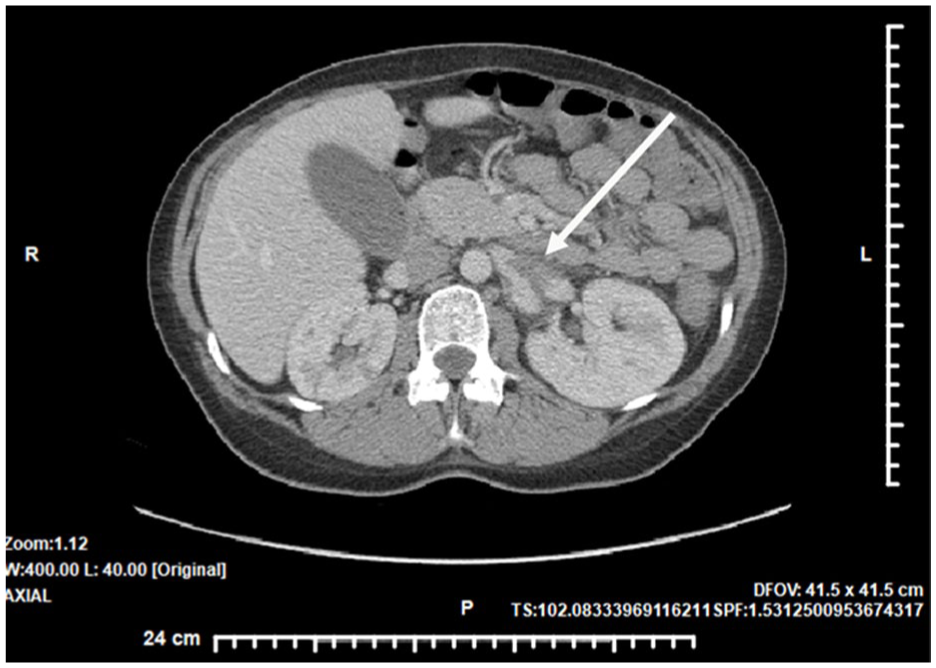
A transverse computed tomographic angiographic image of the abdomen demonstrated thrombus extending into the left renal vein (indicated by the white arrow).
After diagnosis the patient shared they had a clotting disorder with a history of deep vein thrombosis (DVT) and pulmonary embolism. Anticoagulant therapy had been discontinued for an unknown duration prior to delivery. This would have been important patient information provided to the sonographer and radiologist prior to imaging as it may have altered the sonographic protocol, which could have included images of the left renal vein and the inferior vena cava (IVC). This stresses the importance of gathering a thorough patient history prior to performing a sonogram. It is unknown whether the final diagnosis of OVT could have been reached without the CT. The patient was admitted and started on anticoagulant therapy, as well as analgesics. The patient was also referred for further consultation with the hematology department, but no further surveillance information was available.
Discussion
The ovarian veins originate from the plexus of the broad ligament near the ovary and fallopian tube and courses anterior to the psoas muscle. 6 The right ovarian vein drains directly into the IVC, whereas the left ovarian vein drains into the left renal vein. 6 In addition to postpartum delivery, OVT may be caused by malignancy, surgery, trauma, infection, clotting disorders, or other medical conditions that can increase the risk of venous thrombosis. 1
Ovarian vein thrombosis is thought to occur more frequently on the right side because of the increased length of the right ovarian vein, potentially resulting in additional incompetent valves along with the sharp angle, as it enters the IVC (See Figure 5). 7 The right ovarian vein is also more likely to be compressed at the pelvic brim by the natural dextrorotation of the uterus during pregnancy. 8 OVT is more common in cesarean deliveries compared to vaginal deliveries. 3
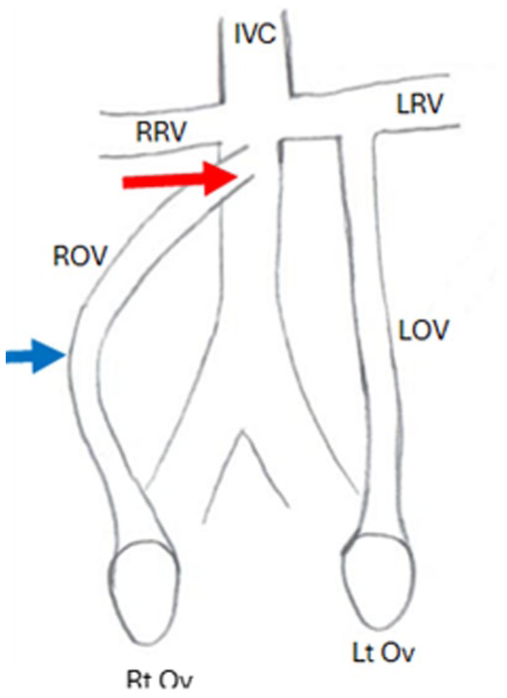
An anatomical diagram is provided to demonstrate the relationship of the renal veins to the ovarian veins. This illustrates the sharp angle of entry of the ROV into the IVC (red arrow) compared with the 90° angle of the LOV into the LRV. The ROV is also longer (blue arrow) than the LOV, creating more potential valve incompetence in the ROV. RRV, right renal vein; LRV, left renal vein; IVC, inferior vena cava; ROV, right ovarian vein; LOV, left ovarian vein; Rt Ov, right ovary; Lt Ov, left ovary.
In the case of OVT, thrombus impedes venous drainage and causes patient symptoms. In a retrospective review of OVT cases by Bannow and Skeith, the main symptoms to raise suspicion for OVT were persistent fever, lower abdominal pain, palpable pelvic mass, nausea, vomiting, or constipation. 9 If left untreated, venous thrombus may result in further venous stasis and growth of the thrombus. Extension of the thrombus into the left renal vein or IVC could become life-threatening if embolization occurs. In addition, since active infection is present in many cases, delayed treatment could lead to the development of sepsis. 10
The most common treatment for OVT is a combination of anticoagulation therapy and antibiotics. 5 In the current patient case, she was given analgesics and anticoagulants, but not antibiotics. The physician’s reason for this choice was unknown. However, a recent scoping review by Monnet et al 4 was based on 1128 patients with OVT and indicated that anticoagulant therapy was an adequate treatment in those cases. As with any DVT, extension and propagation of thrombus will determine the patient’s prognosis. The most likely prognosis with OVT is favorable, but if thrombus extends into the IVC, the risk of pulmonary embolism and decreased mortality rises. 11
Other causes of low abdominal pain, as part of the differential diagnoses for OVT, include appendicitis, pyelonephritis, endometritis, adnexal abscess, and ovarian torsion. 12 It is often necessary for the sonographer to make immediate decisions, during the examination, about deviating from the standard protocol to ensure imaging of additional anatomical structures, as needed. In the current patient case, the sonographer should have imaged the left renal vein and possibly IVC with the use of color and spectral Doppler. Increased awareness of OVT, as a differential for pelvic pain, benefits sonographers and their patients. It is important to note that only transabdominal pelvic imaging is typically used during the postpartum period, due to contraindications associated with transvaginal imaging, which can limit optimal visualization of certain anatomical structures. There is no established lab accreditation protocol that addresses sonographic evaluation of a suspected OVT. In addition, this examination can be further complicated by bowel gas, pain, and other patient factors that limit adequate visualization. Sonography, magnetic resonance imaging (MRI), and CT are all useful diagnostic imaging techniques to detect an OVT. 8 Pelvic MRI is the most sensitive and specific; however, it can be limited by availability, increased examination time, cost, and the imaging of overlying bowel. 13
A recent case study by Jha et al 14 had many comparable similarities to the current patient. While their case study documented a right-sided OVT, following a cesarean section, the imaging findings and progression were very similar to the current patient case. Both case studies used sonography first and documented tubular hypoechoic areas, in the adnexa, which prompted a contrast-enhanced CT that ultimately diagnosed OVT. 14 The many complicating factors that can limit the results of a pelvic sonogram contribute to the need for a multi-modality imaging approach to obtain a definitive diagnosis of OVT.
Conclusion
In this case, the patient experienced postpartum, left-sided pelvic pain. She had a VBAC delivery with minimal postpartum bleeding, but her symptoms began shortly after delivery. After diagnostic imaging and a diagnosis, it was discovered that the patient had a history of blood clots and had stopped anticoagulation medication, prior to delivery, which increased the risk for an OVT. This case is exceedingly rare, due to vaginal delivery coinciding with a left-sided OVT, given that it typically occurs on the right and often after cesarean delivery. Even though the occurrence of an OVT on either side is uncommon, it is still important for sonographers to keep this specific pathology as a potential diagnosis. Understanding that OVT is more common on the right side is essential, considering there are many other potential causes of right-sided pelvic pain.
This patient case is a good example of how important it is for sonographers to be aware of pathology, no matter how rare the occurrence. It might seem easy to assume that OVTs would be more common on the left side, similar to varicoceles, due to the venous anatomy. This case raises awareness for sonographers that OVT may be encountered on either side, although it occurs more frequently on the right. In addition, in cases of patient edema, among postpartum patients, it may be useful to examine the renal veins and/or IVC, for suspected thrombus. While it is known that postpartum OVT after cesarean is more common, compared with vaginal deliveries, further clinical research is needed to determine whether VBAC contributes to an increased risk of OVT.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because all patient information was de-identified.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Generative AI Use in Writing
The authors used OpenAI’s ChatGPT solely to assist with language refinement, including improvements to clarity, coherence, and academic tone. No scientific content, data interpretation, or conclusions were generated by the tool. All ideas, analyses, and final manuscript content were developed, verified, and approved by the authors.