
Abstract
Left ovarian vein thrombosis is a very rare and infrequent thrombotic condition that mainly occurs in the postpartum or postoperative period. We report a case of a 25-year-old para-1 woman who presented with 2 weeks of postpartum fever and dull aching abdominal pain more on the left side. Before operation, the diagnosis was left adnexal mass secondary to questionable ovarian cyst torsion and she underwent laparotomy. Her intraoperative findings revealed a firm left broad ligament mass with extension to retroperitoneum and it was difficult to demarcate the proximal end. Moreover, on the second day of postoperation, abdominal Doppler ultrasound indicated enlargement of the left ovarian vein that was filled with thrombi having hypoechoic and intermediate echogenicity. After the confirmation of left ovarian vein thrombosis, the case was treated with anticoagulants and broad-spectrum antibiotics and then well improved. Our case climaxes an instant diagnosis and therapeutic significance concerning ovarian vein thrombosis to early manage/avert complications. Besides, the ovarian vein thrombosis diagnosis requires a high index of suspicion for a case presented with fever and abdominal pain.
Introduction
Ovarian vein thrombosis (OVT) is a rare thrombotic condition that affects mostly postpartum women; however, it can be linked to different pelvic-related diseases like pelvic inflammatory disease, gynecological surgery, and malignancies.1,2 OVT is a condition that occurs in 0.02%–0.18% of pregnancies and 80%–90% of it can be identified on the right side of the affected cases. 2 Therefore, prompt diagnosis and treatment of such condition are important to prevent morbidity and mortality related to thrombosis and associated infections. 3 OVT can be diagnosed based on clinical signs such as abdominal pain and fever in combination with abnormal imaging findings that include ultrasound, computed tomography (CT) scan, 4 and magnetic resonance imaging (MRI). 5 Here, we present a rare case of postpartum left ovarian vein thrombosis (LOVT).
Case presentation
A 25-year-old para-1 woman was admitted to our hospital due to dull aching abdominal pain more on the left side of 2 weeks duration. The patient gave a full-term alive baby with normal spontaneous vaginal delivery in the primary hospital. The patient had also low-grade intermittent fever, nausea, and malaise. Otherwise, she has no history of smoking, sexually transmitted diseases or abnormal vaginal discharge, diabetes, and hypertension before or during pregnancy follow-up.
On physical examination, she was tachycardic with a pulse rate of 107 beats/min and her body weight was 54 kg. She had tenderness on the left lower quadrant area by deep abdominal palpation. Her pelvic examination revealed cervical motion tenderness (CMT) and left adnexal tenderness. In addition, she had a 6 cm × 6 cm size abdominopelvic mass located more on the left adnexal region.
Her laboratory findings indicated leukocytosis (17,800 white blood cells/µL) and thrombocytosis (873,000 platelets/µL). The first abdominal ultrasound showed a 6.3 cm × 6.1 cm echo complex left adnexal mass with probe tenderness and an empty endometrial cavity (by bed-side ultrasound). Her pre-operative diagnosis was left adnexal mass secondary to questionable ovarian cyst torsion and she underwent laparotomy. Pre-operative Doppler ultrasound was not done because the OVT was not suspected initially.
Her intraoperative findings indicated 6 cm × 5 cm sub-serous myoma on the left fundal part of the uterus with minimal cystic changes (Figure 1).
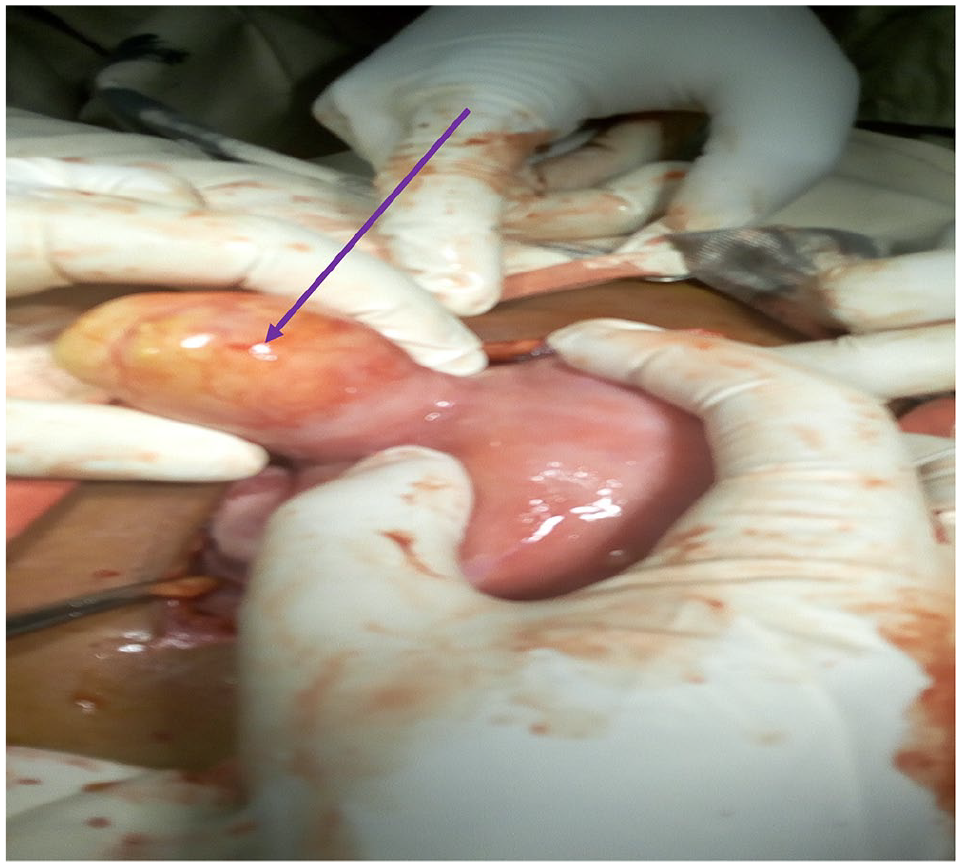
Laparotomy image of the patient ovary (arrow indicates sub-serous myoma).
In addition, there was minimal reactive fluid in the cul-de-sac. Her left side fallopian tube was edematous, inflamed, and there was a firm left broad ligament mass which extended to the retroperitoneum and it was difficult to outline the proximal end (6 cm × 3 cm). However, the right ovary and fallopian tube appeared to be normal. With the above findings, the intraoperative diagnosis was sub-serous myoma with questionable postpartum LOVT.
On the second day of post-operation, an abdominopelvic ultrasound revealed an engorged left side ovary with an internal arterial flow on Doppler. The engorged left ovarian vein was filled with thrombi having hypoechoic and intermediate echogenicity.
Therefore, her diagnosis indicated the presence of postpartum LOVT, and she was treated with ceftriaxone 1 g intravenously (IV) BID and metronidazole 500 mg IV TID. In addition, unfractionated heparin was started within 12 h of operation and continued for the first 5 days with warfarin 5 mg PO/day. Then, antibiotics and heparin were discontinued after 5 days, while she was afebrile and responded well. Her international normalizing ratio (INR) value became 2.69, and it achieved the target value (2.0–3.0) after she took 5 mg PO/day warfarin for 5 days. Then, she was discharged improved with warfarin 5 mg PO/day for 1 month and appointed for a follow-up to the medical referral clinic. Furthermore, she came to referral clinic for follow-up after 1 month of warfarin treatment and she became symptom-free, and her INR was within the target value. Finally, she was appointed to come after a total of 3 months of warfarin treatment to have imaged.
Discussion
The incidence of thrombo-embolism is high and affects females particularly during pregnancy and postpartum period. 6 The incidence of OVT ranges from 1/600 to 1/2000 pregnancies and its sign and symptom is a triad of pain, fever, and abdominal mass. 7
OVT of our case was left side ovarian vein implicated. The study reported by Assal et al. 8 indicated an equal occurrence of right and left OVT; however, in a peripartum condition, the right-side OVT was predominant. In addition, another study indicated that 80% of OVT patients were affected by the right-side ovarian vein, whereas the left ovarian vein and both ovarian veins occur only in 6% and 14% of patients, respectively. 9 The right OVT might be due to the dextrorotation of the uterus through pregnancy compressing the vein and due to the increased length of the right ovarian vein and the existence of incompetent valves. 10 However, the left-side ovarian vein drains into the left renal vein if there is any pathological condition that affects the left kidney like nephropathy, cancer, or trauma that can affect the left-side ovarian vein. 10 Our case of LOVT might be explained by the left fundal sub-serous myoma. 11 The present case had abdominal pain and intermittent fever. Similarly, studies reported that patients with OVT usually have a fever, pelvic pain, and palpable abdominal mass.12,13 Moreover, patients with OVT also will have non-specific symptoms like malaise, diffuse abdominal pain, or difficulties of breath. In occasional cases, a mass could be palpable; however, this is an uncommon finding. 14
Therefore, OVT prompt diagnosis is vital to avert morbidity and mortality and it should be considered among postpartum patients with fever and abdominopelvic or flank pain. 15 In our case, OVT was not considered initially even if she had abdominal pain and fever. Therefore, our case LOVT was diagnosed by laparotomy with the support of Doppler. In this case, if OVT was suspected initially, we would have prevented the invasive surgical procedures.
Studies recommend magnetic resonance angiography, and it has high sensitivity and specificity but CT scan with intravenous contrast can also be used.4,5 Normally, CT scan shows a thick-walled engorged ovarian vein with rim enhancement and central hypodensity. 16 However, the non-functioning of CT scan and MRI in our institution, non-affordability for the high cost of diagnostic modality in the private institutions for our patient, and the absence of laparoscopic surgery led us to a big challenge in identifying LOVT before undergoing unwanted surgery.
Our case was treated with anticoagulants and broad-spectrum antibiotics and responded well. Likewise, several studies recommended antibiotics and anticoagulants as a treatment option for OVT.16,17
Conclusion
In conclusion, LOVT is a very uncommon treatable condition, and its sign and symptoms in postpartum patients are acute abdominal pain, fever, and pelvic pain. Nevertheless, left-side OVT like our case is very rare when compared to right-side OVT; this might be due to the left fundal sub-serous myoma problem in this patient. Also, OVT might happen after delivery and during pregnancy with a possible significant risk of morbidity and mortality if the problem is not early identified and treated properly. Therefore, OVT diagnosis requires a high index of suspicion in any pregnant/postpartum woman complaining of fever and lower abdominal pain.
Footnotes
Acknowledgements
We acknowledge our client who gave us consent to publish her intraoperative and postoperative medical condition. Besides, our appreciation goes to Hawassa University’s comprehensive specialized hospital for the provision of care service for this patient.
Author contributions
M.T. had initial contact with the patient, took care of follow-up of the case, and did intraoperative postoperative medical conditions. S.T. did therapeutics consultancy management and drafting of the case report, and A.T.H. did correction for article text and appraisal. Additionally, all authors critically revised the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approval from the ethics committee was not required and the patient consented for case report participation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.