
Abstract
Objective:
The principal objective was to compare the diagnostic accuracy of two-dimensional transvaginal ultrasonography (2D TVUS), three-dimensional transvaginal ultrasonography (3D TVUS), and hysteroscopy with histopathology in patients with abnormal uterine bleeding.
Materials and Methods:
Fifty patients were included and underwent the three imaging methods. The negative predictive value, positive predictive value, sensitivity, and specificity of the methods were calculated. Determination of endometrial pathology and endometrial polyps by measuring the endometrial thickness, volume, and uterine area was examined.
Results:
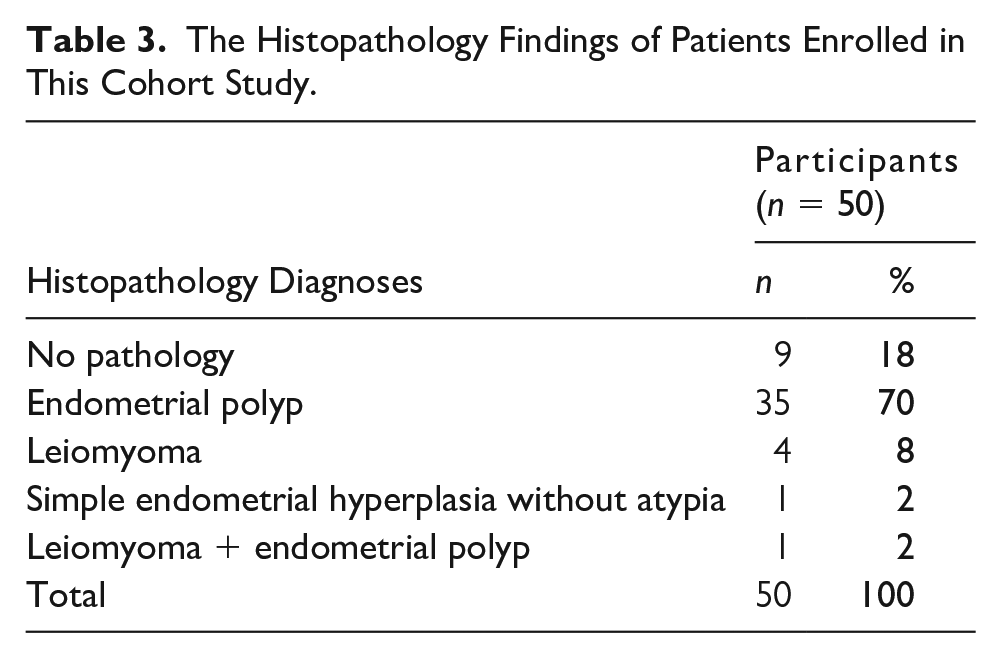
The complaint of menorrhagia was reported by 72.0% of participants. Histopathologically, 70.0% of the patients had endometrial polyps and leiomyoma being monitored. An endometrial polyp was detected in 58.0% of the patients by 2D TVUS, 80.0% by 3D TVUS, and 68.0% by hysteroscopy. While 2D TVUS demonstrated 65.71% accuracy in the detection of an endometrial polyp, 3D TVUS had an 80.0% accuracy, and hysteroscopy had a 77.77% accuracy. An endometrial polyp was detected when the uterine area was ≥237 mm2. If the endometrial thickness was over 10.5 mm, it was found to be related to an endometrial polyp. According to the volume measurements by 3D TVUS, the detection of an endometrial polyp was made with 96.4% sensitivity, provided that the pathology volume was ≥0.082 cm3.
Conclusion:
In this cohort of patients, 3D TVUS achieved a high sensitivity to detect abnormalities and could be considered as an initial diagnostic modality, prior to the surgery, and may rival invasive procedures, such as hysteroscopy.
Abnormal uterine bleeding (AUB) is defined as an irregularity of menstrual bleeding in terms of amount, duration, and frequency. It is a condition that can affect the social, psychological, and sexual qualities of life. 1 AUB occurs in approximately 30% of reproductive aged women and is a common reason for patients to present for a gynecological examination. 2 It is responsible for 70% of outpatient clinic applications and 25% of gynecological operations among perimenopausal and postmenopausal patients. 3 The age and reproductive status are important in the differential diagnosis, and its incidence is higher in the adolescent, reproductive, and perimenopausal period, while it is rare in the prepubertal and postmenopausal ages. The abnormality generally shows structural pathologies but may also be due to endocrinological and hematological disorders. Anatomic causes such as an endometrial polyp or a leiomyoma can be distinguished from functional causes such as anovulation with anamnesis, physical examination, laboratory tests, and imaging methods. Traditional terminologies about menstrual bleeding patterns changed with the classification of the International Federation of Gynecology and Obstetrics in 2011, and the etiological reasons were comprehensively classified by defining structural and nonstructural causes. 4 The diagnostic tests used to evaluate the uterine cavity after anamnesis and pelvic examination are the noninvasive methods such as two-dimensional transvaginal ultrasonography (2D TVUS) and three-dimensional transvaginal ultrasonography (3D TVUS). These imaging choices provide arbitrary planes and a volume measurement opportunity and are minimally invasive, unlike a hysteroscopy.
In this study, the primary objective is to identify the diagnostic accuracies of 2D TVUS, 3D TVUS, and hysteroscopy in patients with AUB when compared to the gold standard of histopathology.
Materials and Methods
This single-center study was designed retrospectively. Its rationale, purpose, approach, and methods were unanimously approved by the members of the Gazi University Clinical Research Ethics Committee, attesting conformity with the Helsinki Declaration.
Collection of Data and Patient Enrollment
The study was carried out by reviewing the 2D TVUS and 3D TVUS images and hysteroscopy records of the patients who attended the Gazi University Faculty of Medicine Hospital gynecology outpatient clinic between August 2018 and October 2020 and had AUB.
Fifty patients in their reproductive period between the ages of 20 and 52 years were included. Patients were reviewed randomly, without regard to menstrual phase, due to their abnormal menstrual cycles. All three diagnostic imaging methods were applied to patients who have no contraindications for hysteroscopy results including pregnancy, excessive vaginal bleeding, early postpartum stage, acute infection, history of cervical surgery, uterine rupture, or sensitivity to anesthesia.
The anamnesis and demographics of the patients were obtained from reviewing the patient’s files. The complaints were divided into menorrhagia, metrorrhagia, menometrorrhagia, and premenstrual spotting.
Patients in the postmenopausal period with insufficient anamnesis and surgery records and who underwent hysteroscopy except the indication of AUB were excluded. Surgery reports and pathology results were accessed via the NUCLEUS v9.29.43 Data Processing System.
Two-Dimensional Transvaginal Ultrasonography
The 2D TVUS was performed using Philips HD11XE (2006), Koninklijke Philips Electronics N.V. and General Electric Healthcare Voluson Logiq 9 (2010), USA. The endometrium was measured perpendicularly from the thickest point of the double layer in the sagittal plane, and the structures in the cavity were evaluated. While the endometrium, which is seen as a hyperechogenic and regular line with distinctly separated endometrium and myometrium borders, was accepted as normal. Structures with various echogenicity levels that disrupted the continuity of the uterine cavity and caused an irregular appearance were considered abnormal. Structures more hyperechogenic than the endometrium were described as endometrial polyps, while structures that were more uniform and denser than polyps were accepted in favor of a submucous leiomyoma.
Three-Dimensional Transvaginal Ultrasonography
The three-dimensional evaluation was performed with a General Electric Healthcare Voluson E6 (2016), USA ultrasound system and a General Electric Healthcare Voluson E6 (2016), USA RIC 5-9-D 3D transducer. Coronal, sagittal, and axial planes were created as arbitrary and three-dimensional images of the pathologies were obtained. Following longitudinal plan visualization, the “Volume Analysis” tab was selected, and the volume was measured with the Virtual Organ Computer-aided Analysis (VOCAL) program. The endometrium was placed between the green arrows, and the traces were drawn using a pointer; finally, the volume image was obtained by clicking the “Done” and then the “Accept Region of Interest” tabs.
Hysteroscopy
The Karl Storz (Tuttlingen, Germany) GmbH Campo Trophyscope, Bettocchi office hysteroscopes, and GmbH 26F monopolar operative hysteroscopy sets were used. The panoramic view of tubal ostia and cavity was provided. Soft lesions with a pedicle or a broad base covered with the endometrium were defined as endometrial polyps. Lesions with a broad base, smooth shape, and vascularization were evaluated as a submucous leiomyoma. Endometrial sampling was performed even when no pathology was visualized. The samples were sent to the Gazi University Faculty of Medicine, department of pathology, in 10% formaldehyde.
Statistics
The data were analyzed in IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA). Descriptive statistics were represented as the number of patients, mean (±) standard deviation, and percentage. Characteristics related to the menstrual history are presented as mean (±) standard deviation, frequency, and percentage. The suitability of continuous variables to normal distribution was evaluated using visual (histogram and probability graphs) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk tests). For categorical variables, whether there is a difference between groups (nonparametric data) in terms of frequency was compared using chi-square (χ2) tests. Variables determined to be normally distributed between two independent groups were compared with the Mann-Whitney U test for all other parameters that were found to be not normally distributed with the independent samples t test. Accuracy was represented using the terms of negative predictive value (NPV), positive predictive value (PPV), sensitivity, and specificity by cross-tabs. The endometrial pathology and endometrial polyps were determined by measuring the endometrial thickness, volume, and uterine area. This was calculated by multiplying the length and width of the uterus in sagittal plane with 2D TVUS, which was searched by using the ROC curves and calculating the area under it. The statistical significance value (P value) was accepted as ≤.05.
Results
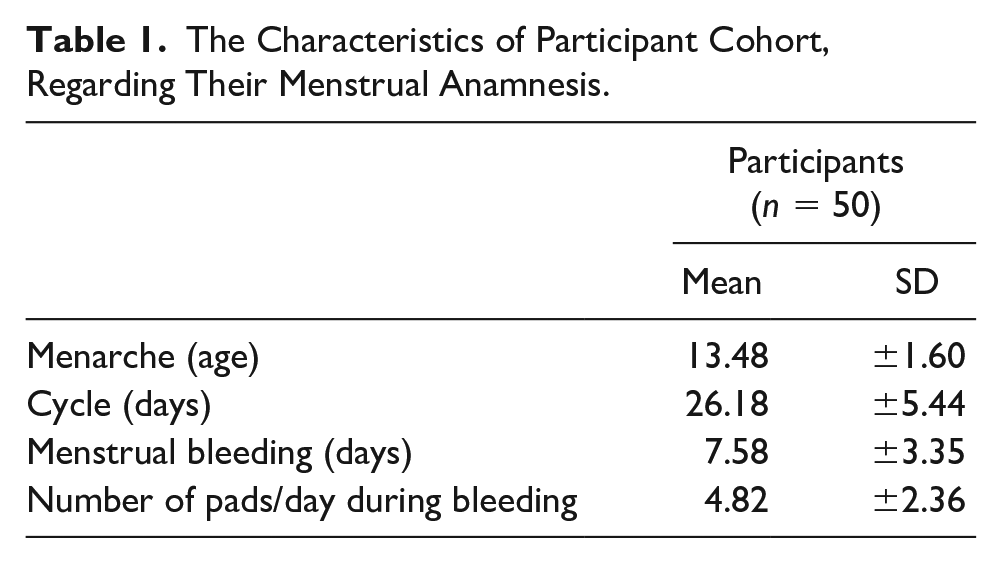
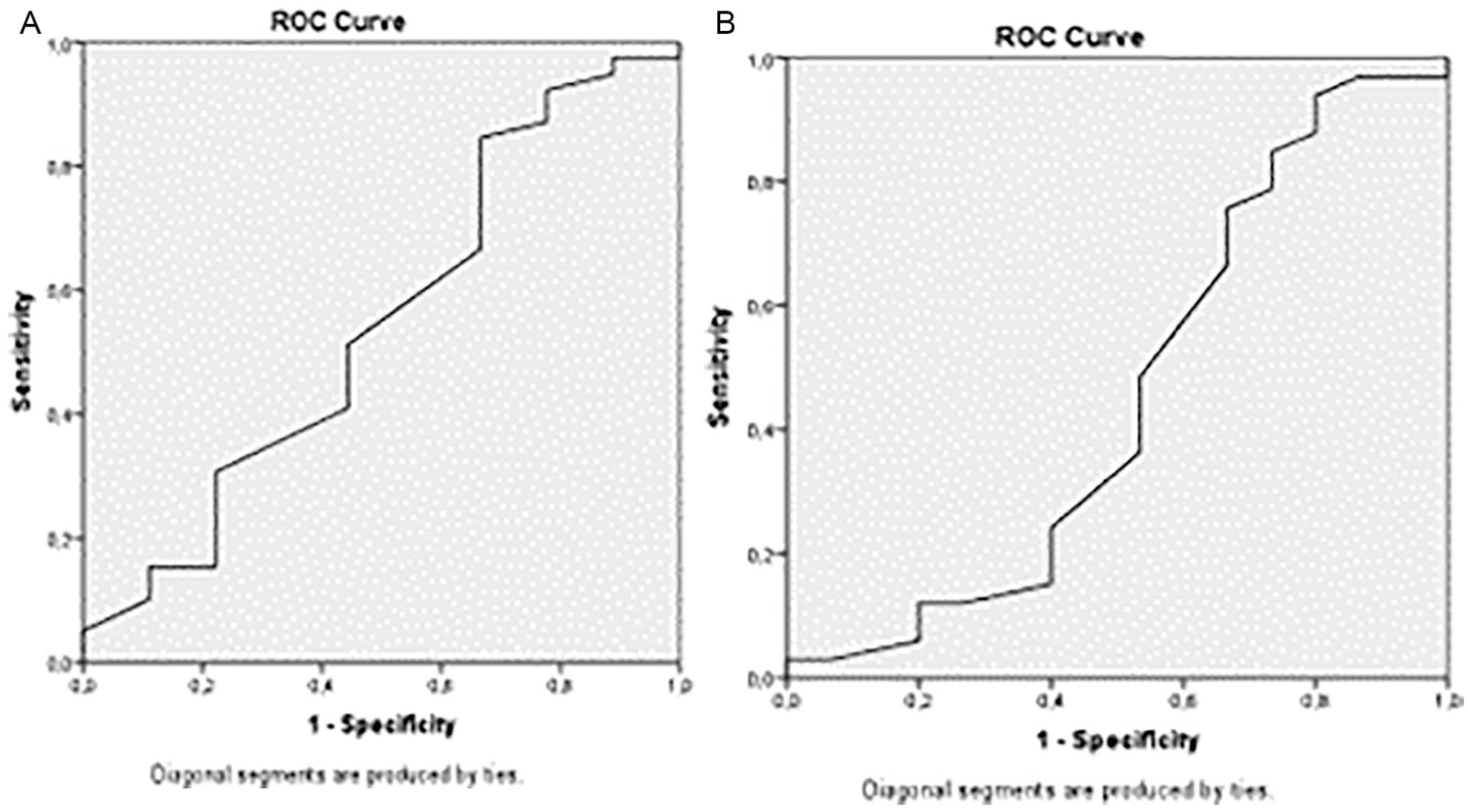
The average age of enrolled participants was 41.04 ± 6.31 years, and all were in their reproductive period. Normal weight was registered in 32% of patients while 40% were overweight and 28% were obese. Three participants were nulligravid, and ten women had a history of abortus. There was no correlation with gravia, para, and abortus history to the pathologies found. All the patients were admitted for AUB with different complaints (Figure 1). The characteristics of the menstrual anamnesis are shown in Table 1, and the diagnoses of participants by 2D TVUS, 3D TVUS, and hysteroscopy are shown in Table 2. Table 3 shows the pathology findings. The PPV, NPV, sensitivity, and specificity of methods compared with gold standard histopathology are shown in Figure 2. A submucous leiomyoma was detected with the highest sensitivity and specificity by 3D TVUS with proper localization identification (Figure 3). An estimation of the correct position of the abnormality was possible by rotation of the image with 3D TVUS (Figure 4). The uterine area is measured in square millimeters for the detection of pathology. There was a pathology with a sensitivity of 83% and a specificity of 62.5% provided that the uterine area was ≥227 mm2 (Figure 5A). An endometrial polyp was detected with a sensitivity of 80.6% and a specificity of 53.8%, provided that the uterine area was ≥237 mm2 (Figure 5B).
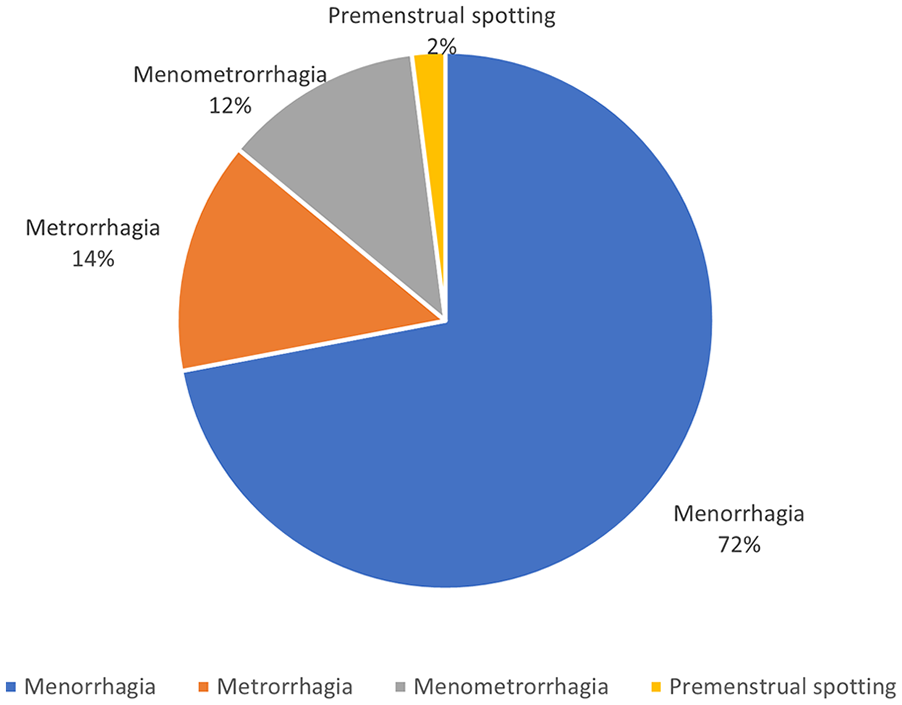
The varied types of abnormal uterine bleeding reported by patients in the study cohort.
The Characteristics of Participant Cohort, Regarding Their Menstrual Anamnesis.
The Diagnoses of Pathologies Found With 2D TVUS, 3D TVUS, and Hysteroscopy.
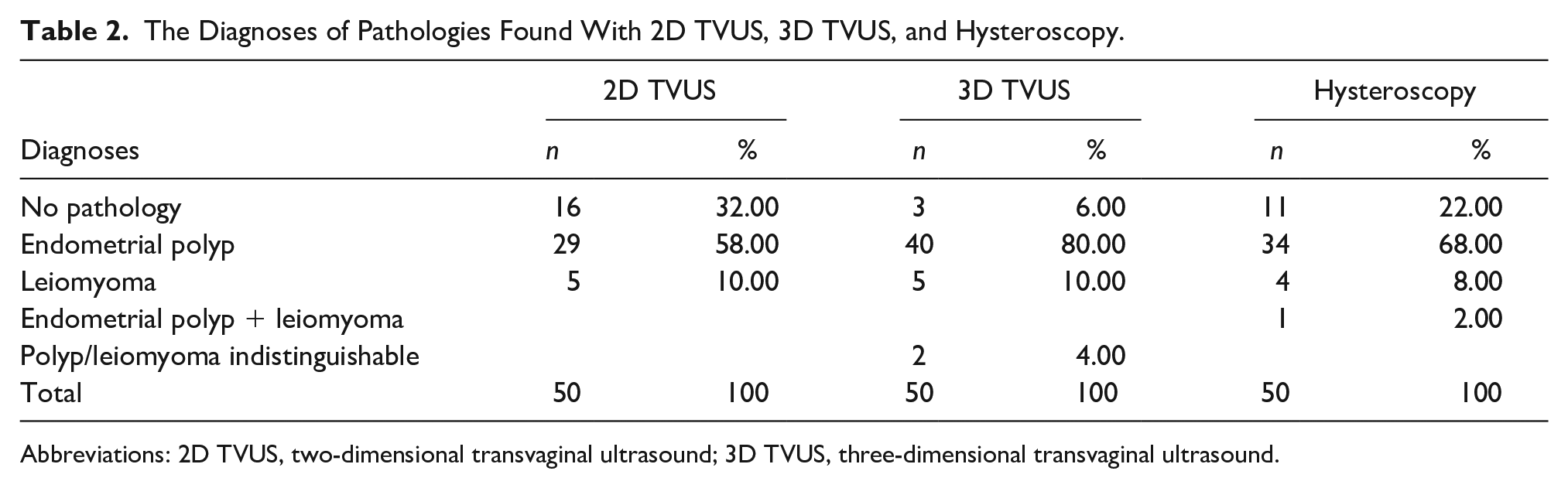
Abbreviations: 2D TVUS, two-dimensional transvaginal ultrasound; 3D TVUS, three-dimensional transvaginal ultrasound.
The Histopathology Findings of Patients Enrolled in This Cohort Study.
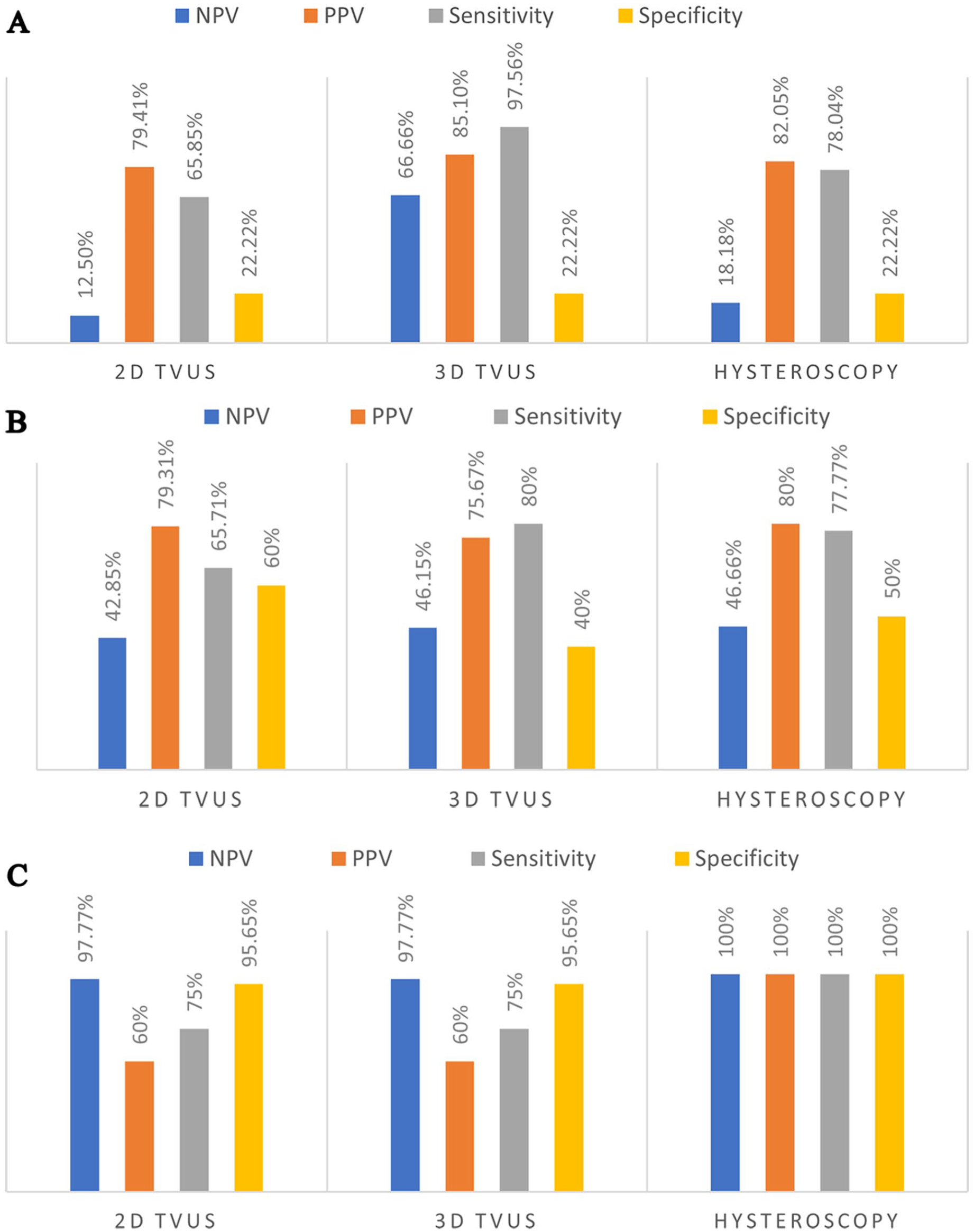
The detection rates of pathology (A), endometrial polyp (B), and leiomyoma, (C), based on the three diagnostic imaging methods. (2D TVUS, two-dimensional transvaginal ultrasound; 3D TVUS, three-dimensional transvaginal ultrasound; NPV, negative predictive value; PPV, positive predictive value).
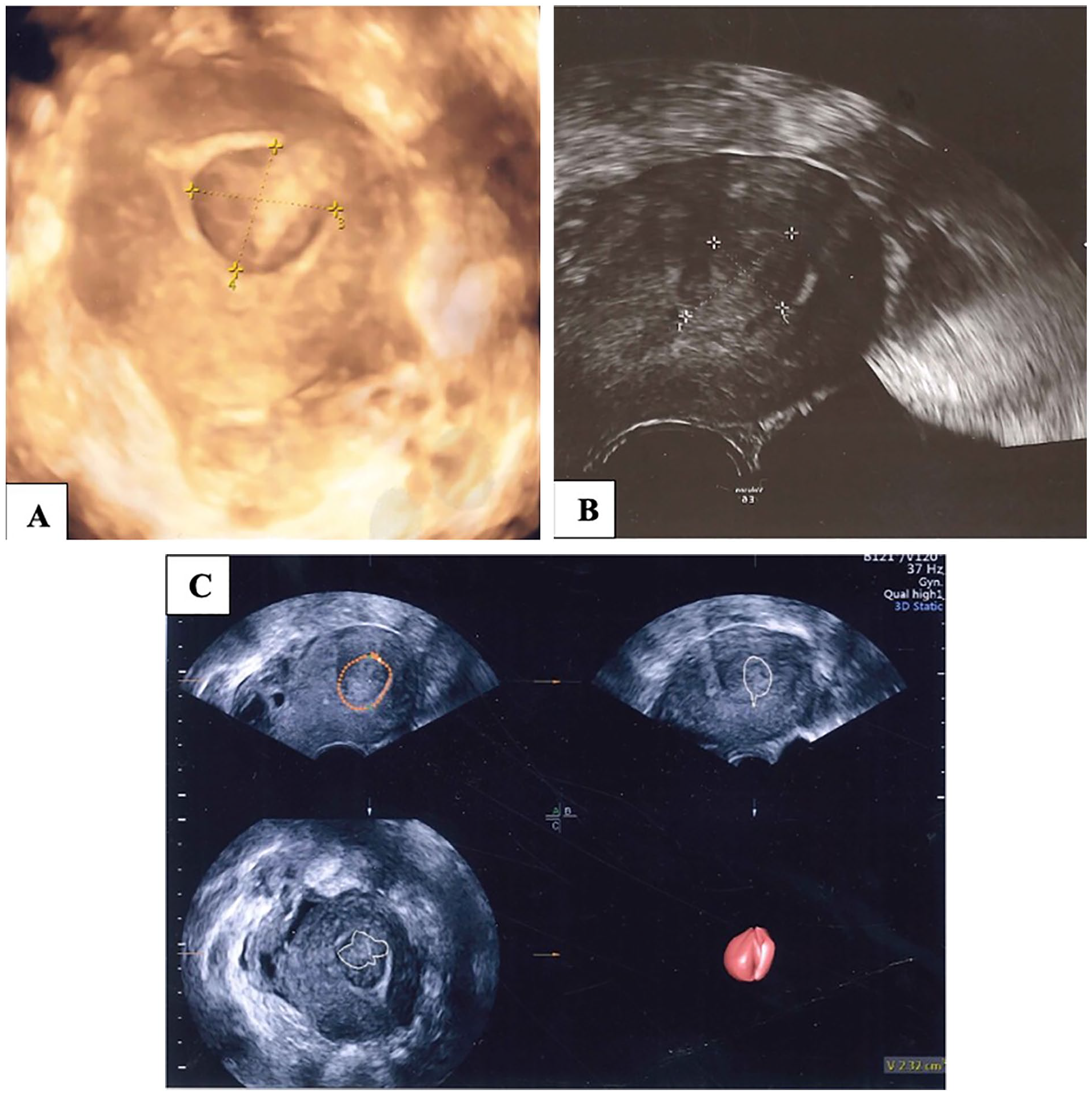
A submucous leiomyoma demonstrated with three-dimensional transvaginal ultrasonography (3D TVUS) (A), two-dimensional transvaginal ultrasonography (2D TVUS) (B), and after utilizing the Virtual Organ Computer-aided Analysis (VOCAL) program (C).
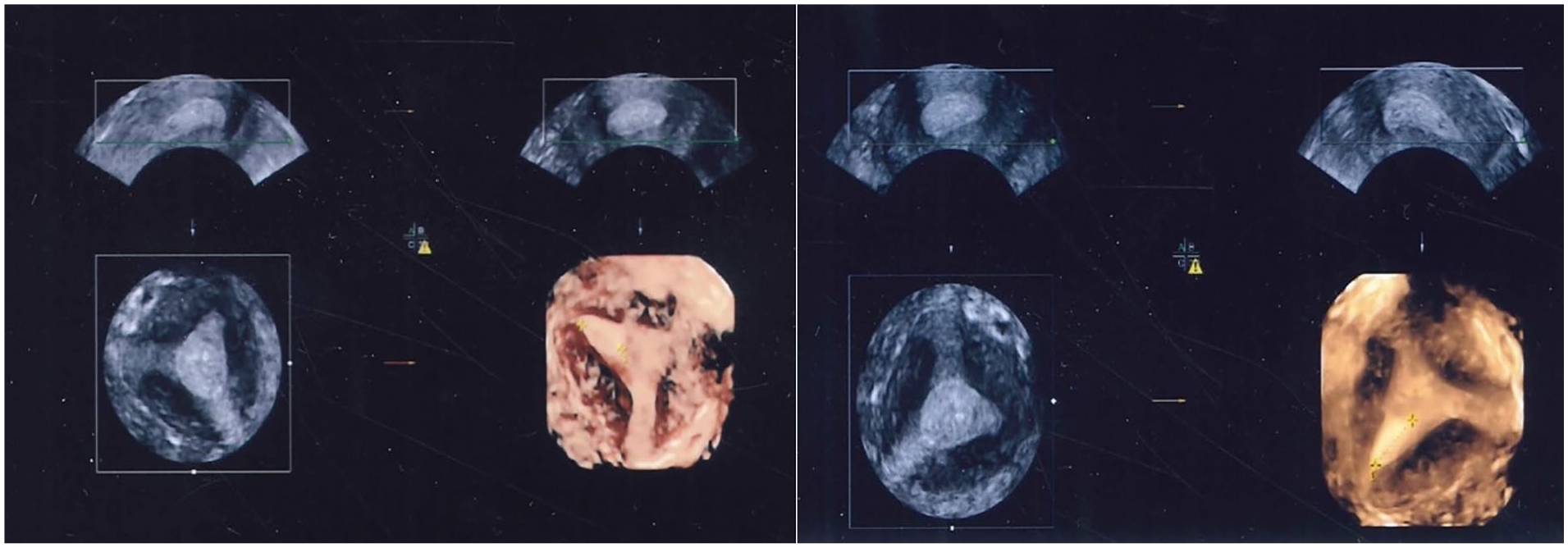
An approximately 1.5-cm diameter polyp located close to the right cornual area. The current image axis can be changed, and the endometrium-myometrium border can be displayed more clearly with three-dimensional (3D) ultrasonography.
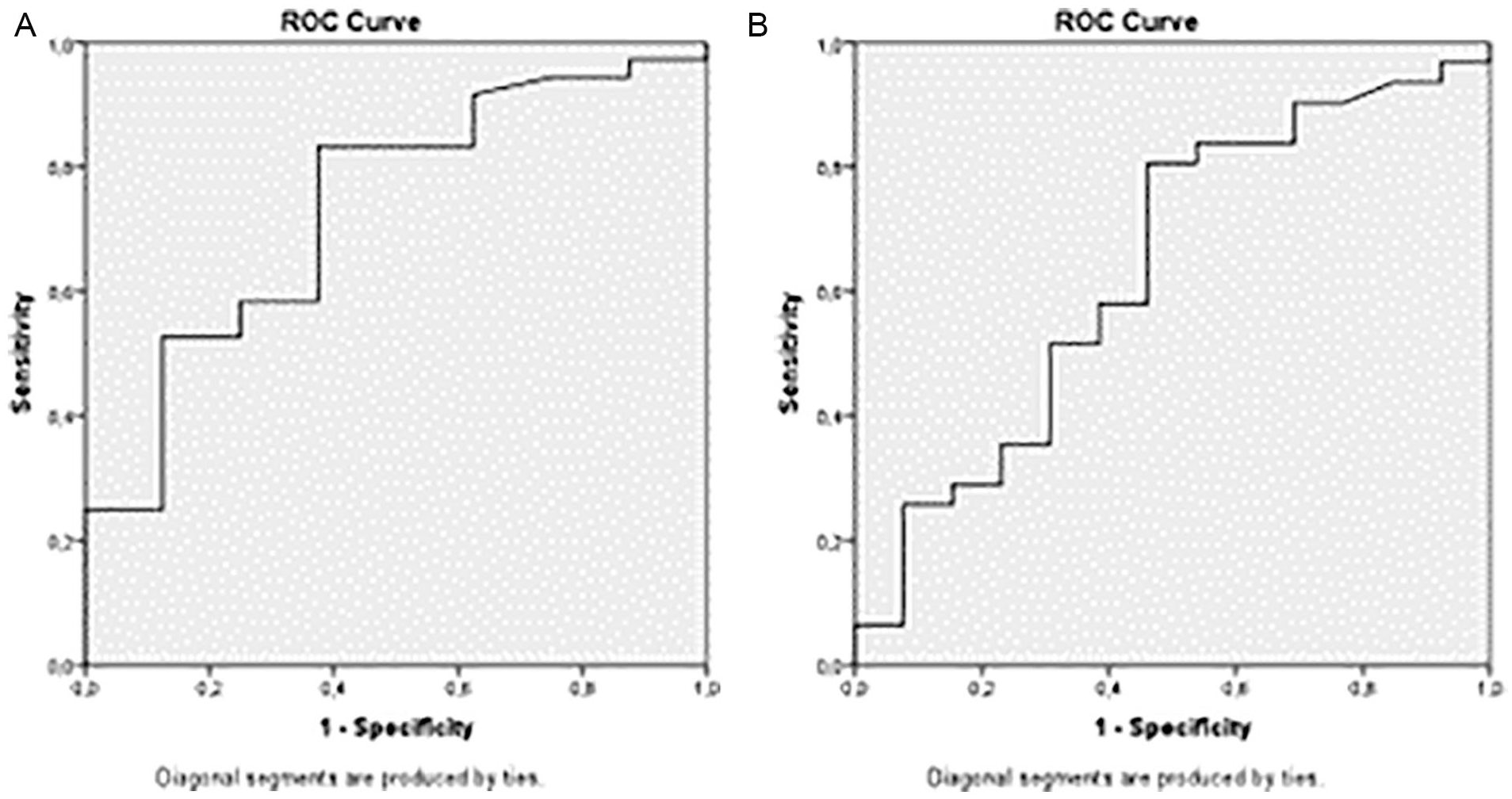
The ROC curve (receiver operating characteristic curve) shows the relationship between the uterine area measured in two-dimensional transvaginal ultrasonography (2D TVUS) and the pathological status (A). The ROC curve (receiver operating characteristic curve) shows the relationship between the uterine area measured in two-dimensional transvaginal ultrasonography (2D TVUS) and the endometrial polyp (B).
The endometrial thickness was measured by 2D TVUS in millimeter unit. The pathologic sensitivity and specificity were 84.6% and 37.5%, respectively, provided that the thickness of the endometrium was ≥8.85 mm (Figure 6A) and an endometrial polyp present, and 75% and 33%, respectively, provided that the thickness of the endometrium was ≥10.5 mm (Figure 6B).
The ROC curve (receiver operating characteristic curve) shows the relationship between the endometrial thickness measured in two-dimensional transvaginal ultrasound (2D TVUS) and the pathological status (A). The ROC curve (receiver operating characteristic curve) shows the relationship between the endometrial thickness measured in two-dimensional transvaginal ultrasound (2D TVUS) and the endometrial polyp (B).
According to the volume measurements made with 3D TVUS, there was a pathologic sensitivity of 97% and a specificity of 40% provided that the suspected pathology volume is ≥0.07 cm3 (Figure 7A). The detection of an endometrial polyp had a sensitivity of 96.4% and a specificity of 30%, provided that the pathology volume is ≥0.082 cm3 (Figure 7B). Patients who underwent hysteroscopy and whose pathology volume was measured by 3D TVUS (n = 38) were divided into two groups: office and operative hysteroscopy. The average pathological volume measured by 3D TVUS for patients who underwent office hysteroscopy (n = 31) was significantly lower than that obtained with operative hysteroscopy (n = 7) (3D volume measurement prior to office hysteroscopy = 0.83 mm3 vs 3D volume measurement prior to operative hysteroscopy = 2.69 mm3; P = .003)
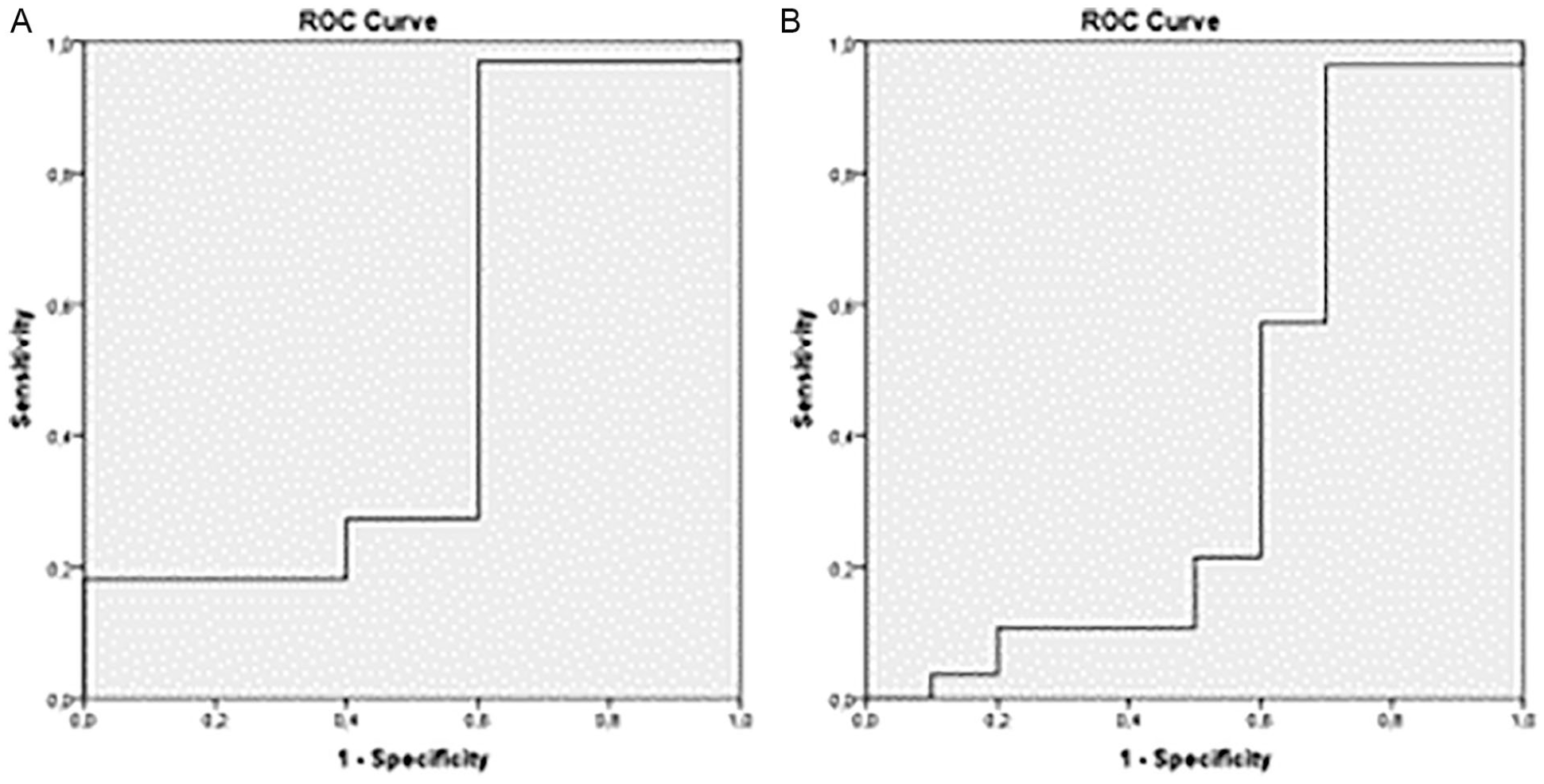
The ROC curve (receiver operating characteristic curve) shows the relationship between the pathology volume measured in three-dimensional transvaginal ultrasonography (3D TVUS) and the pathologic status (A). The ROC curve (receiver operating characteristic curve) shows the relationship between the pathology volume measured in three-dimensional transvaginal ultrasonography (3D TVUS) and an endometrial polyp (B).
Discussion
AUB is the most common symptom of gynecological conditions, and its etiology is complicated. 5 An accurate assessment of the uterine cavity is required for understanding the etiology. One of the most concerning causes of AUB may be endometrial carcinoma, whereas benign etiologies such as leiomyomas and endometrial polyps are more common. 6 Although most of the diagnostic methods do not diagnose with 100% accuracy, sonographic imaging provides sufficient information by means of advances, and it can largely replace magnetic resonance imaging. 7
A systemic review evaluating the success of 2D TVUS in diagnosing etiology showed sensitivity between 60% and 77%.8–12 A sensitivity of 80% has been identified in a large study of 793 reproductive-age women, 13 while in this study, the sensitivity of 2D TVUS was found to be lower than that of the other two methods. A study could not delineate the endometriums owing to the presence of fibroids or adenomyosis 14 while Dreisler et al. 3 investigated the diagnostic accuracy of 2D TVUS between endometrial thickness and detection of an endometrial polyp in asymptomatic patients and found the cutoff value as 5 mm, the PPV as 10%, and the NPV as 99%. In another study, the cutoff value was accepted as 4 mm, and 2D TVUS and hysteroscopy were found to have the same sensitivity and specificity in the detection of endometrial pathology. 15 In another multicenter study, an endometrial thickness greater than 8 mm with 2D TVUS identified endometrial polyps in 80% of patients. 16 In this study, 8.85 mm was significant to interpret a pathology, and 10.5 mm was commented in favor of endometrial polyps.
In the current study, besides the endometrial thickness, the dimensions of the uterus were measured by 2D TVUS, and for endometrial polyp estimation, a sensitivity of 80.6% could be reached. One of the major limitations of the 3D technology is that there are differences in distinguishing between a normal and an abnormal cavity between sonographers, and 3D volume measurements at this stage reduce these differences. 14 Irregular pathologies are displayed in three-dimensions, providing important information regarding size and localization. 17 In our study, all 3D TVUS measurements were made by the same investigator (H.K.) who had no prior experience before and was under the supervision of an experienced sonographer in the first ten patients, after which the investigator performed the measurements independently.
In a study, it has been reported that determining a volume more than 1.2 mL in patients with AUB by the VOCAL program may be diagnostic for an endometrial polyp. 18 In this study, pathology volume measurements had high sensitivities to catch an endometrial pathology and endometrial polyp. By means of these, it is possible to avoid invasive procedures or to choose office hysteroscopy without anesthesia. In a study comparing 3D TVUS with hysteroscopy, 3D TVUS detected endometrial polyps with 80% sensitivity and 100% specificity. 19 In another study, endometrial polyps were demonstrated with a specificity of 69.5% by 2D TVUS and 88% by 3D TVUS. 20 Balen et al. 21 found 3D TVUS to be 100% sensitive in detecting polypoid lesions in the uterine cavity. In a 5-patient pilot study, 3D TVUS showed all intracavitary lesions correctly. 22 In a study conducted by Pasqualotto et al., 23 45.9% of endometrial polyps and 28% of submucous leiomyomas were found in patients with AUB. Another study found that AUB caused by endometrial polyps accounted for 16.2%, as the most common etiology. 5 In addition, Clark and Stevenson 24 reported a slightly higher rate of endometrial polyp, and some other studies showed the rate is between 10% and 30%,25,26 while this study detected 70% of the endometrial polyps as the most common reason and following 8% leiomyoma. The most common symptom in patients with leiomyoma is menorrhagia, at a rate of approximately 30%. 27 In the current study, 72% of all patients had menorrhagia, and specifically all the patients with leiomyoma complained about menorrhagia.
Sonography enables accurate measurement of the size of leiomyomas. Determining the exact position of leiomyomas and whether they extend into the endometrium is very important for them to refer to surgery. 28 Although a study shows a high level of agreement between 2D and 3D ultrasonography in the diagnosis of leiomyoma, 29 2D TVUS was not an accurate method for evaluating submucous leiomyomas protruding into the uterine cavity30,31 and has limitations to assess the uterus. 32 It can be very difficult to differentiate a submucosal leiomyoma from an intramural leiomyoma and to evaluate its relationship with the endometrial cavity by 2D TVUS. A reconstructed coronal plan may attribute useful information for planning surgical management of the case. 33 Three-dimensional ultrasonography can provide more anatomical details because of improvement in the resolution 34 and optimizes the detection of inciting etiologies. 35 In AUB, the main differential includes both endometrial and myometrial causes, 36 and 3D TVUS provides the visualization of the borders of two layers. In four patients we examined with 3D TVUS, leiomyomas were submucous, and operative hysteroscopy was preferred instead of office hysteroscopy. Three-dimensional images were consistent with hysteroscopy. The value of 3D TVUS has been supported in other published studies.22,28,37 Hysteroscopy is an important method for the diagnosis of an intrauterine pathology with AUB and taking a targeted biopsy. 38 The sensitivity and specificity are high in a large series of hysteroscopies performed in postmenopausal patients (98.2%). 39 However, it provides subjective evaluation and indirect information regarding the depth of myometrial extension.
In one study, with 2D TVUS, endometrial polyps were seen in 74% and submucous leiomyomas in 39% accuracy. With hysteroscopy, these rates were 100% and 99% accuracy, respectively. 23 Elsewhere, hysteroscopy was found superior with 71% sensitivity and 100% specificity in the diagnosis of endometrial polyps, and this rate is confirmed by biopsies. 40 Similarly in the some studies, hysteroscopy was found to be more valuable in the evaluation of uterine pathologies.41,42
In a study performed including 285 patients comparing hysteroscopy and 2D TVUS, endometrial polyps even smaller than 1 cm were detected in approximately half of the cases. 43 On the other hand, when the two methods were compared, no statistically significant difference was found in the diagnosis of an endometrial polyp. 44 In the present study, the sensitivity of hysteroscopy in detecting the pathology and endometrial polyp according to the gold standard histopathology was lower than that of 3D TVUS. The authors felt that the appearance of the endometrium in the proliferative phase of some patients with hysteroscopy prevented the cavity to be evaluated as polypoid, causing a decrease in sensitivity and detection of endometrial polyps.
Limitations
Some of the limitations of this study included the research design as well as the small sample size (n = 50). The most common condition was endometrial polyp, and direct comparisons of different problems were low because of the heterogeneous variety of histopathological findings. All 3D TVUS measurements were made by the same researcher (H.K.) who did not perform the 2D TVUS and hysteroscopy procedures. The aim was to prevent any bias in understanding the accuracy of 3D TVUS.
Conclusion
Although 2D TVUS is an effective, easy-to-use, inexpensive initial imaging modality that is widely used in gynecology, 3D TVUS and hysteroscopy were found to be a more sensitive methods in detecting pathology. This study determined that 3D TVUS was more sensitive and specific in determining the location of uterine lesions. It allowed proper evaluation of the intrauterine cavity and myometrium before resorting to invasive procedures. Hysteroscopy is a method that provides direct imaging, but it is not as effective as 3D TVUS in showing the endometrium and myometrium border. Three-dimensional TVUS provides patient comfort, allowing a noninvasive approach and possibility to future nonanesthetic methods such as office hysteroscopy. In this sense, gynecologists and sonographers should continue to develop their skills utilizing 3D TVUS and advocate its widespread use, as an initial diagnostic imaging choice.
Footnotes
Acknowledgements
The authors thank Muhammed Fevzi Kılınçkaya for reviewing the manuscript with supervision and statistical contributions.
Correction (October 2023):
The Ethical Approval section has been updated with the IRB number.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was obtained from the Gazi University Ethics Committee (approval number 367).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
This trial was presented in 27th EBCOG European Congress of Obstetrics and Gynecology, Athens-Greece as oral presentation by corresponding author, Hazal Kutlucan and the abstract was published in European Journal of Obstetrics, Gynecology and Reproductive Health.