
Abstract
Objectives:
Postcoital bleeding is an uncommon cause of gynecologic hemorrhage; however, it can be severe in a majority of cases necessitating surgical management.
Methods:
We report a case of severe postcoital bleeding in a young woman requiring blood transfusion.
Results:
Hemostasis was achieved using subselective embolization of cervical artery by metallic coils.
Conclusion:
Our case demonstrates a minimally invasive treatment for control of non-obstetric hemorrhage.
Introduction
Postcoital bleeding is a relatively common problem in women. The prevalence ranges from 0.7% to 9% according to various studies. The etiology of postcoital bleeding can be related to benign growths, infection, genital/vulvar lesions, malignancy, and trauma. 1 About 80% of patients with coital trauma have marked vaginal bleeding. 2 The management of postcoital bleeding depends on the etiology, but in cases of traumatic bleeding, surgical repair is the standard of care. In a case series of 19 patients, 9 patients presented with a hemoglobin less than 10 mg/dL. 3 Alternatively, transarterial embolization (TAE) has been successfully used in obstetric and gynecologic hemorrhage.4–7 Although interventional management of gynecologic emergencies does not constitute the “bread and butter” of an interventional cardiologist’s practice, knowledge of pertinent anatomy and appropriate techniques can save lives when such expertise is needed. Here, we present the case of a coital lower genital hemorrhage in a young woman that was successfully managed by TAE. We will then review the anatomy and technical details of angiographic management of gynecologic emergencies. Verbal informed consent was obtained from the patient for their information to be used in this publication.
Case history
A 26-year-old G2P1A1 Latina female presented to the emergency department with profuse vaginal bleeding and syncope approximately 1 h after consensual vaginal intercourse. She denied history of vaginal surgery or use of any foreign objects during intercourse. Upon arrival, patient’s blood pressure was 60/30 mmHg with a pulse rate of 140/min. Abdominal examination was negative for peritoneal signs. Pelvic examination showed large clots at vaginal introitus with poor visualization. The vaginal vault was packed with gauze to tamponade the bleeding. Laboratory testing showed hemoglobin of 9 g/dL. Three liters of normal saline solution and two units of packed red blood cells were administered. Bedside pelvic ultrasound showed free fluid in the pelvis and no signs of intrauterine or ectopic pregnancy. After blood pressure improved to 95/55 mmHg, a computed tomography (CT) abdomen and pelvis with intravenous contrast was obtained that showed a heterogeneous mass measuring 6.1 cm × 5.7 cm at the lower half of the vagina representing a hematoma with extravasation of contrast material from its right posterolateral aspect. Given localized nature of bleeding and patients’ desire to preserve fertility and to facilitate repair of the vaginal laceration in a bloodless field, interventional cardiology was consulted for arterial embolization.
Procedure description
Using a left transfemoral artery approach, a 4-F diagnostic catheter (Omni Flush; AngioDynamics, Latham, NY, USA) was brought to the terminal aorta. An aortogram was performed in the anteroposterior projection using digital subtraction angiography that showed normal anatomy except for evidence of bleeding into the vaginal vault from the right cervical artery (Figure 1). Next, the Omni Flush catheter was brought in an up-and-over fashion into the right internal iliac artery (IIA) using a hydrophilic guidewire (Glidewire; Terumo Interventional Systems, Somerset, NJ, USA). The guidewire was exchanged for a stiff guidewire (Supra Core wire; Abbott Vascular, Abbott Park, IL, USA) and the Omni Flush catheter was exchanged for a 55-cm-length, 6-F guiding sheath (Destination; Terumo Interventional Systems). The sheath was brought over the Supra Core wire and parked at the origin of the right IIA. Using an angled 0.036-in guidewire and 4-F guide catheter, the right cervical artery was selectively cannulated. A floppy-tip guidewire (Runthrough; Terumo Interventional Systems) had been used after initially getting the angled Glide catheter into the IIA to subselect the cervical artery. Once the right cervical artery was sub-selected, three 3-mm coils (Tornado; Cook Medical, Bloomington, IN, USA) and two 5-mm coils (MReye; Cook Medical) were deployed and packed into the right uterine artery with success. Final angiography revealed no further blood flow through this artery and no dye blush was noted in the vaginal vault (Figure 2). Patient was then transferred to the operating room where she was examined under anesthesia and found to have a 5-cm laceration in the posterior vaginal wall that was repaired surgically.
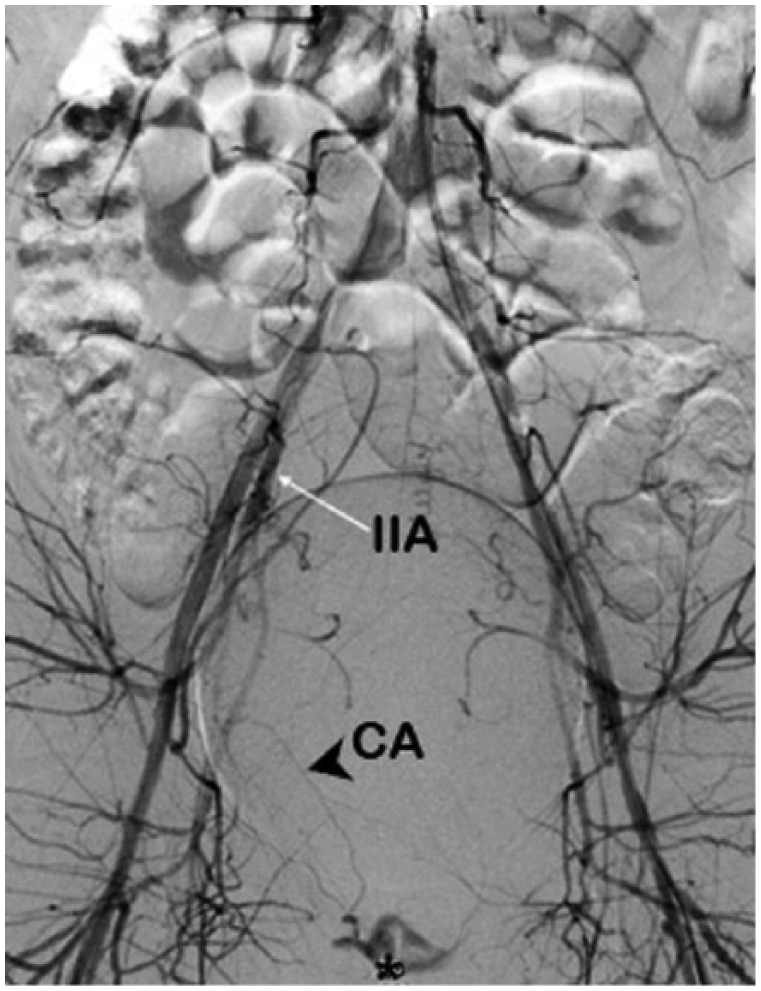
Aortogram showing normal anatomy and * marking extravasation of contrast material from the cervical artery.
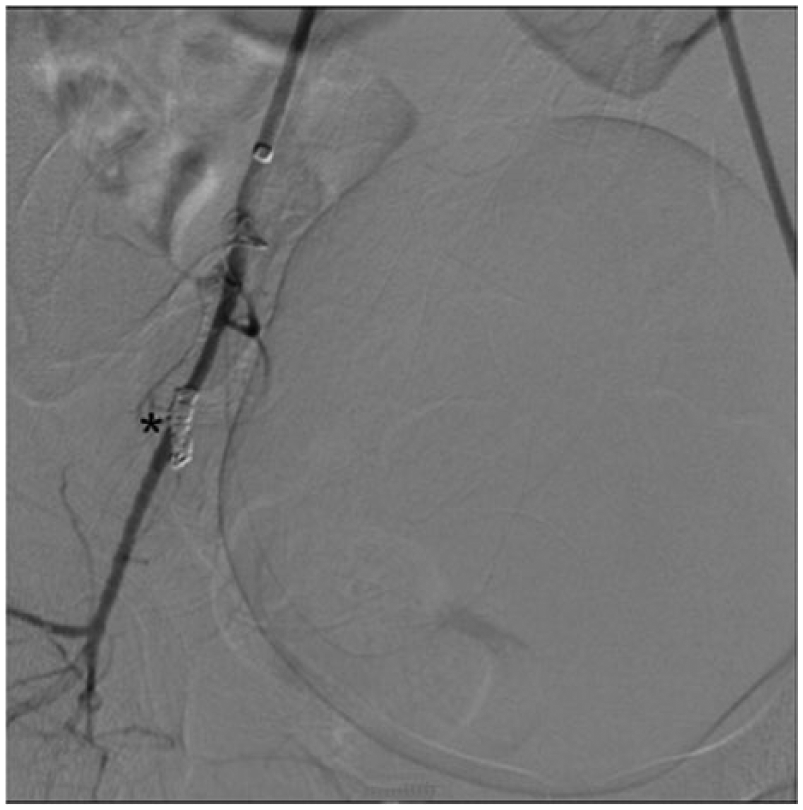
Post-embolization image showing coil (*) in the right cervical artery. No dye blush is seen anymore.
Discussion
We present a case of TAE of cervical artery to control traumatic hemorrhage leading to hemorrhagic shock after consensual vaginal intercourse.
Vaginal trauma after consensual intercourse is not uncommon. The prevalence varies depending on the method used to detect the lesions and spectrum of lesions considered in the study. 8 Nonetheless, coitus remains the most common cause of non-obstetric vaginal injury. 9 A recent study by Astrup et al. reported that 34% of women aged 19–40 years had some kind of vaginal injury after consensual intercourse. Lacerations of the right posterior fornix being were the most common lesion encountered in this study. 10 Risk factors for coital vaginal trauma include first-time intercourse, disproportionate genitalia, vaginal atrophy, stenosis and scarring of the vagina from congenital abnormalities, previous surgery, or pelvic radiation therapy, rough intercourse, insertion of foreign bodies, and dorsal decubitus position during coitus with hyperflexion of the thighs.3,11–13
The use of interventional techniques to control gynecologic etiologies of hemorrhage is less well described due to the relative rarity of these conditions. Indications include gynecologic malignancies, arteriovenous malformations, and trauma. 4 Knowledge of the vascular anatomy of the pelvis is crucial for successful TAE since variations are abundant and outcomes can be potentially disastrous if these are neglected. 14
The IIA bifurcates into anterior and posterior divisions. The posterior division gives rise to parietal branches, namely, iliolumbar, lateral sacral, and superior gluteal arteries. The anterior division has both parietal and visceral branches. The visceral branches include uterine, vaginal, superior vesicle, and internal pudendal arteries. 15 The vaginal arteries can arise from the anterior division of the IIA or the uterine artery itself. 15
In a rare anatomical variation, the blood flow to the lower extremity is supplied by persistent sciatic artery, which originates from the anterior division of the IIA. TAE of uterine artery should only be attempted if distal delivery of embolic material can be safely achieved, otherwise reflux of embolic material can inadvertently embolize the persistent sciatic artery and jeopardize the limb. 16 A case of such complication has been reported during TAE for pelvic trauma. 17
A right common femoral arterial approach is used to access the distal aorta. Use of 5- or 4-F catheters is preferred.4,18 A pelvic arteriography should be performed to identify the source of bleeding and any significant anatomical variations. In a case series of gynecologic bleeding managed by TAE, the most common finding on angiography was reported to be a tumor stain. 19 The interventionist should try to select the bleeding vessel using digital road-mapping for a targeted embolization when possible.
Several embolic materials have been described in the literature including gelatin sponge, metallic coils, poly-vinyl alcohol particles, n-butyl cyanoacrylate, and microspheres. 18 In gynecologic cases, gelatin sponges and metallic coils are used more commonly. Metallic coils are usually preferred for larger vessels or when faster hemostasis is desired. 18
Outcomes and complications of TAE for gynecologic hemorrhage have been reported in a few studies. In case of trauma, studies have reported a success rate of 90%–100%.20,21 Bleeding control rates for malignant causes of gynecologic bleeding are over 90% and similar results have been reported for arteriovenous malformations. 4
Many women who undergo TAE regain normal menstruation and fertility. In a recent study by Lee et al., 22 97.3% of the patients reported normal menstruation and 9.7% had successful pregnancies. There have been several reports of successful pregnancy after TAE for arteriovenous malformations.23,24 There are no data on fertility rates after endovascular management of traumatic non-obstetric bleeding.
This report demonstrates that TAE of pelvic arteries is a safe and effective tool that can be used in cases of emergent gynecologic hemorrhage and requires adequate knowledge of relevant anatomy and endovascular interventional skills.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.