
Abstract
Dirofilariasis is a parasitic disease that typically infects animals. In rare cases, it can be transmitted to humans. The two species that infect humans more frequently are Dirofilaria repens, which causes subcutaneous nodules, and Dirofilaria immitis, causing pulmonary manifestations. Dirofilaria repens is an indirect parasite transmitted to humans by mosquitoes, which act as vectors, while dogs generally constitute the primary reservoir. Their bites allow the larvae to pass into human tissues where they develop. Cutaneous dirofilariasis manifests clinically with the appearance of papules, nodules, abrasions with secondary dryness, lichenification, changes in skin pigmentation, and intense itching. Sonography is the diagnostic tool that allows for easy identification of the dirofilariasis. Treatment is surgical and involves removal of the granuloma containing the parasite. This patient report describes a rare case of cutaneous dirofilariasis, localized to the cheek.
Dirofilariasis is a parasitic disease that typically infects animals, canids, and felids, as well as other carnivorous species. 1 In rare cases, it can transmit the disease to humans. The species that infect humans more frequently are Dirofilaria repens (e.g., 72.22%), which causes subcutaneous nodules, and Dirofilaria immitis (e.g., 6.94%), which causes pulmonary manifestations.2 –4 There are at least 60 species of filarial parasites classified into groups, which is based on their location at the mature state. 5 This can be divided into skin, lymphatic, and body cavity locations and are favored by poor hygienic-sanitary conditions. Like all vector-borne diseases, travel to endemic countries and environmental factors have led to a rapid expansion of dirofilariasis and an increase in its incidence. 6 Dirofilaria repens is an indirect parasite transmitted to humans by mosquitoes, which act as vectors, while dogs are generally the primary reservoir. Mosquitoes then bite dogs (i.e., hemophagia) and then humans, inoculating the parasite, which develops in the subcutaneous tissue. The affected areas are the most exposed and unprotected, such as the periorbital and subconjunctival areas. The nodules grow in relation to the growth of the parasite and generally manifest clinically with papules, nodules, excoriations with secondary xerosis, lichenification, changes in skin pigmentation, and/or intense itching. Unlike animals, where the parasite can penetrate the bloodstream, in humans it remains in the subcutaneous tissues and generally develops at the site of the bite. Humans are not a primary reservoir because they do not allow sexually mature dirofilaria to develop, so microfilaremia is unlikely. The highest frequency of infections occurs in areas most infested by mosquitoes, such as rivers or marshy areas. 7 The most effective treatment for cutaneous dirofilariasis is surgery, which consists of excision of the parasite and granuloma, while in its systemic forms, and the use of drug therapy with antiparasitics. 8 The purpose of this report is to describe the main sonographic features of D repens and to facilitate the differential diagnosis from other superficial masses.
Case Report
A 59-year-old man, residing in Italy, presented for diagnostic imaging with a painless swelling on his right face that had appeared 6 months previously. The patient described intermittent episodes of redness and intense itching in the same area of the swelling, alternating with asymptomatic periods. He had no previous illnesses and/or respiratory or gastrointestinal symptoms. The patient had not had contact with pets, had not been exposed to occupational infections, and had never traveled abroad. Physical examination revealed a firm, mobile, and painless subcutaneous nodule on his right face. No skin changes were present. His laboratory testing results were normal. The patient underwent sonography of the superficial facial tissues using a MyLab 9 XP (Esaote, Genova, Italy) ultrasound equipment system with an 8 to 15 MHz linear transducer. The examination revealed a round, subcutaneous cystic mass, 8 × 4 mm in diameter, in the right parotid region, with mixed solid/fluid content and extended into the subcutaneous adipose tissue. The solid component had a double-tracked, filamentous appearance with autonomous dynamic movements (See Figure 1) (Supplemental Video 1).
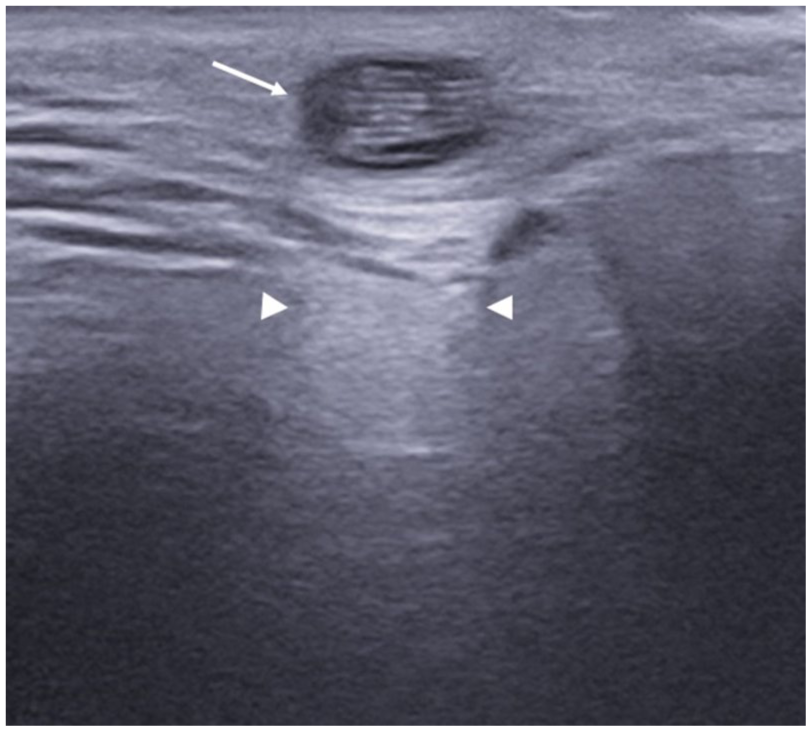
A sonographic image is provided of the superficial facial tissues. The sonographic examination was performed with a high-frequency transducer (e.g., 15 MHz) and revealed a round, fluid-filled subcutaneous mass with a rail-like, filamentous appearance (long arrow). The posterior acoustic enhancement (arrowheads) is caused by the fluid content of the mass.
The examination was further enhanced by the use of color Doppler to demonstrate that there were no intralesional vascular signals (See Figure 2).
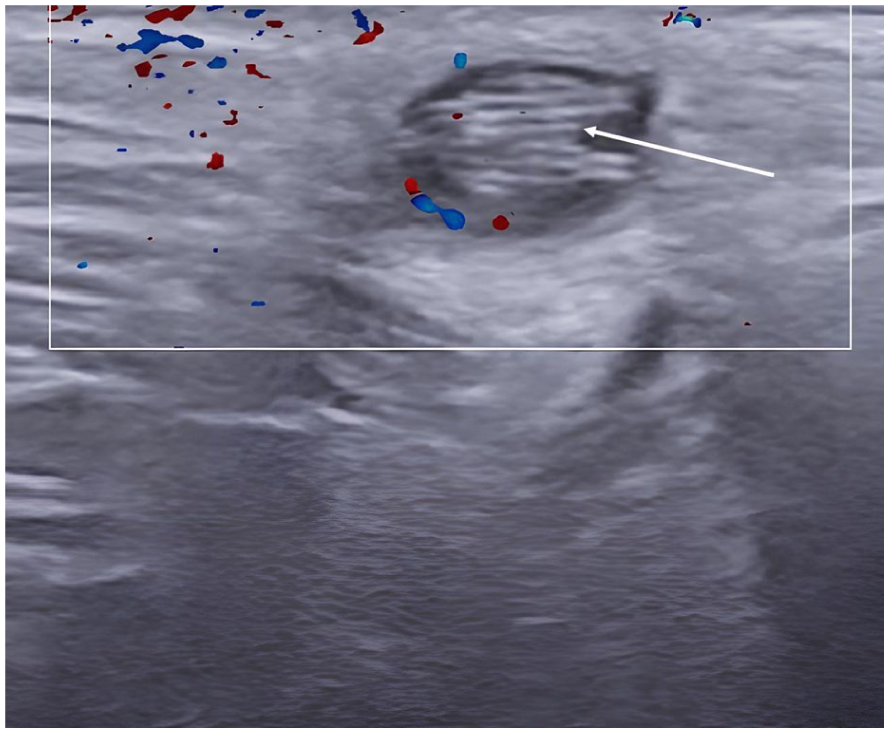
A color Doppler image is provided of the superficial facial tissues. This image demonstrated a lack of vascular signals within the mass. The absence of vascular signals rules out the heterologous nature of the mass. The image also captured the filamentous appearance of the dirofilaria (arrow).
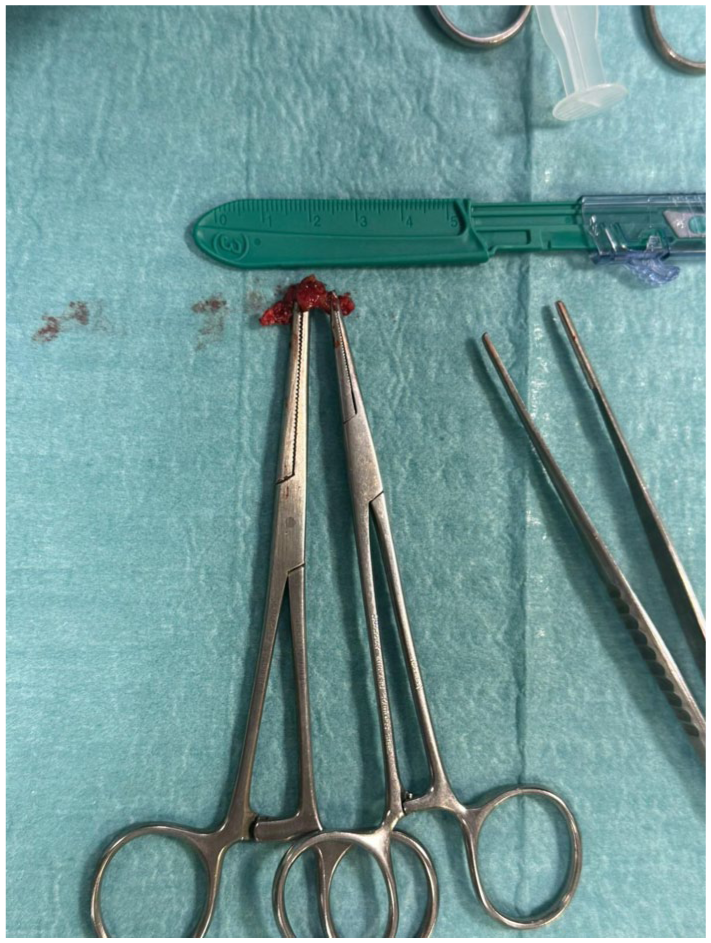
Based on these findings, surgical excision was performed the following day. Macroscopic examination of the surgical specimen revealed a live, white, thread-like nematode (See Figure 3) (Supplemental Video 2), which was inserted into a granulomatous mass (See Figure 4).

A photograph is provided of the surgical findings with an accompanying centimeter scale. The dirofilaria (arrow) extracted from the granuloma appears as a long, thin white filament.
A photograph is provided of the surgical findings. The specimen has the appearance of the granuloma with the dirofilaria inside.
Histological analysis confirmed the diagnosis of a dirofilariasis and was morphologically compatible with the genus “Dirofilaria repens.” The peripheral blood smear was negative for microfilariae, and serological tests revealed no eosinophilia. These results confirmed the diagnosis of localized cutaneous dirofilariasis, without systemic dissemination (hematogenous or lymphatic). No drug therapy was administered as the disease was only localized.
Discussion
The most frequent locations of cutaneous dirofilariasis were the trunk and head, less frequently the scrotum9,10 and the subcutaneous facial tissue. 11 The clinical diagnosis is very difficult because the patient is often asymptomatic, and they are often nonspecific. Eosinophilia is often absent, and serum IgE levels are normal. Sonography is the primary imaging examination and generally concludes the diagnostic process, as it easily identifies the parasite within the granuloma. Sonography of this type should be performed with a linear transducer because it offers the best resolution for superficial tissues. The parasite appears as a filamentous structure with a rail-like appearance and may show movement if observed for sufficient time. Color Doppler may be useful for the differential diagnosis with tumorous masses, which, unlike dirofilaria, exhibit intralesional vascular signals. The definitive diagnosis is established after removal of the lesion, with direct visualization, and identification of the dirofilaria. Morphological study of whole parasites or histological sections of them is still the diagnostic gold standard method for diagnosing human dirofilariasis. 12
It is important to visualize the parasite to differentiate the lesion from other benign masses such as sebaceous cysts, hair cysts, lipomas, or other granulomas. Management of these patients is not complex, as the treatment of choice is surgical removal of the granuloma. In addition to surgical removal, oral pharmacological treatment with diethylcarbamazine (DEC) (e.g., 2 mg per kg three times a day) for a period of 4 weeks is recommended. 13 The limitations of this case report are its single-case nature, lack of histopathological images, and geographic specificity. It may be useful in the future to provide similar case series of this pathology, as well as comparative imaging studies and epidemiological monitoring.
Conclusion
Cutaneous dirofilariasis should be suspected in patients with recent onset of one or more itchy subcutaneous masses, following insect bites or travel to endemic areas. Sonography is essential for rapid diagnosis and provides guidance for surgical intervention. Clinical cases are currently the main source of information on this disease, so contributing to increased levels of evidence can be very important for greater knowledge and understanding of human parasitic diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because all procedures performed were in accordance with the ethical standards of the institution and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from the subject before the release of the report for review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.